You might also like
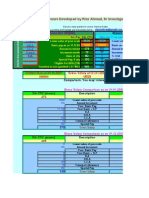
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Musculoskeletal RehabilitationDocument25 pagesMusculoskeletal RehabilitationNadia Ayu TiarasariNo ratings yet
- Neuroscience Physical Therapy Evaluation FormDocument7 pagesNeuroscience Physical Therapy Evaluation FormTaral PatelNo ratings yet
- Spinal Cord InjuryDocument39 pagesSpinal Cord InjuryrahatNo ratings yet
- Orthopedic Physiotherapy Assignment: 1. Patient HistoryDocument4 pagesOrthopedic Physiotherapy Assignment: 1. Patient HistoryarushiNo ratings yet
- Neurological Physiotherapy EvaluationDocument8 pagesNeurological Physiotherapy EvaluationAreeba RajaNo ratings yet
- Muscular Dystrophy Types and PhysiotherapyDocument4 pagesMuscular Dystrophy Types and PhysiotherapyAbdul Ghafoor SajjadNo ratings yet
- The Efficacy of Brotzman Physiotherapy Protocol On Pain and Knee Range of Motion in Post Surgical Total Knee Arthroplasty Subjects With ObesityDocument6 pagesThe Efficacy of Brotzman Physiotherapy Protocol On Pain and Knee Range of Motion in Post Surgical Total Knee Arthroplasty Subjects With ObesityInternational Journal of Physiotherapy and ResearchNo ratings yet
- Interpretting ABG SuccessfullyDocument15 pagesInterpretting ABG Successfullyanimathz100% (1)
- Erectile DysfunctionDocument145 pagesErectile Dysfunctionluna palitoNo ratings yet
- CH 4 ArthrokinematicsDocument17 pagesCH 4 ArthrokinematicsBoddu Suresh BabuNo ratings yet
- Pediatric Neurologic Physical TherapyDocument38 pagesPediatric Neurologic Physical TherapyfagpatelNo ratings yet
- Special Tests of The KneeDocument21 pagesSpecial Tests of The KneeZephyrin Izukw100% (1)
- Physiotherapy Management of Tennis Elbow................ ArticleDocument5 pagesPhysiotherapy Management of Tennis Elbow................ ArticleRupika SodhiNo ratings yet
- Bobath Approach: Concepts and PrinciplesDocument30 pagesBobath Approach: Concepts and PrinciplesJulia SalvioNo ratings yet
- Chest Pulmophysiothera PY: Prepared By: Floriza P. de Leon, PTRPDocument35 pagesChest Pulmophysiothera PY: Prepared By: Floriza P. de Leon, PTRPFloriza de LeonNo ratings yet
- Understanding-Ocd 2016 v2Document27 pagesUnderstanding-Ocd 2016 v2Samanjit Sen Gupta100% (1)
- Avascular Necrosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandAvascular Necrosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsRating: 4 out of 5 stars4/5 (2)
- Motor Recovery in StrokeDocument14 pagesMotor Recovery in StrokefagpatelNo ratings yet
- Ankle Fracture Rehab ProtocolDocument6 pagesAnkle Fracture Rehab Protocolbmj123No ratings yet
- Anatomy of the Lumbar SpineDocument39 pagesAnatomy of the Lumbar Spinepasha100% (1)
- Physiotherapy ManagementDocument137 pagesPhysiotherapy ManagementLavanya AuthimooalmNo ratings yet
- History and Definition of Physical TherapyDocument50 pagesHistory and Definition of Physical TherapyJiggs LimNo ratings yet
- Peripheral Nerve Injury: Relevant Anatomy: Peripheral Neuroanatomy andDocument7 pagesPeripheral Nerve Injury: Relevant Anatomy: Peripheral Neuroanatomy andJulia SalvioNo ratings yet
- Electro NotesDocument9 pagesElectro NotesJulia SalvioNo ratings yet
- Therapeutic ExercisesDocument50 pagesTherapeutic ExercisesBalram Jha100% (3)
- 2 Year Physical Therapy NotesDocument129 pages2 Year Physical Therapy Notesthwiseman94% (17)
- Prostho MCQ Www-Matterhere-Com NRRDocument10 pagesProstho MCQ Www-Matterhere-Com NRRYoung FlameNo ratings yet
- Physical Therapy DocumentationDocument5 pagesPhysical Therapy DocumentationdjdkNo ratings yet
- PT Initial EvaluationDocument6 pagesPT Initial EvaluationJudith Bartolo100% (1)
- MFRDocument30 pagesMFRMfxMazprofx100% (1)
- 861 Drug Prescribing For Dentistry 2 Web 2 Email PDFDocument94 pages861 Drug Prescribing For Dentistry 2 Web 2 Email PDFRaphaela TravassosNo ratings yet
- Physiotherapy for Tennis Elbow Pain ReliefDocument2 pagesPhysiotherapy for Tennis Elbow Pain ReliefenadNo ratings yet
- DeQuervain Disease, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandDeQuervain Disease, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Physiotherapy Assessment for CP ChildrenDocument5 pagesPhysiotherapy Assessment for CP ChildrenAnonymous cCy8GpNo ratings yet
- Pre-Test Maternal and Child Health NursingDocument18 pagesPre-Test Maternal and Child Health NursingDefensor Pison GringgoNo ratings yet
- Dermatome & MyotomesDocument9 pagesDermatome & MyotomesfagpatelNo ratings yet
- Physiotherapy For PoliomyelitisDocument16 pagesPhysiotherapy For Poliomyelitisabdalsucs100% (1)
- Cardio Pulmonary AssessmentDocument7 pagesCardio Pulmonary AssessmentRaj KannanNo ratings yet
- Suspension TherapyDocument52 pagesSuspension TherapyROJA MACHERLA0% (1)
- Peripheral Nerve InjuriesDocument29 pagesPeripheral Nerve InjuriesbrillniksNo ratings yet
- DC Current Enhances Drug Delivery Via IontophoresisDocument32 pagesDC Current Enhances Drug Delivery Via Iontophoresisfagpatel100% (2)
- Marissa Lamanna March 2013Document44 pagesMarissa Lamanna March 2013agung100% (1)
- Coughing TechniqueDocument18 pagesCoughing TechniqueSiva ShanmugamNo ratings yet
- Movement Disorders Types - Mayo ClinicDocument1 pageMovement Disorders Types - Mayo ClinicdrrajmptnNo ratings yet
- Types of GaitDocument3 pagesTypes of GaitLorenzSantosHernandezNo ratings yet
- Role of Physiotherapy in Management of Polio..seminarDocument14 pagesRole of Physiotherapy in Management of Polio..seminarAmandeep SinghNo ratings yet
- Physiotherapy Guidelines For Manual HyperinflationDocument5 pagesPhysiotherapy Guidelines For Manual HyperinflationAhmed Abd Elrauf100% (2)
- Physiotherapy examination questions and answersDocument8 pagesPhysiotherapy examination questions and answersMohan KrishabiNo ratings yet
- Functional Re-Education TrainingDocument24 pagesFunctional Re-Education Trainingtamilvanan3100% (1)
- Upper Extremity: John Ryan H. Paris, PTRP, PT, CFMP, CVKTPDocument12 pagesUpper Extremity: John Ryan H. Paris, PTRP, PT, CFMP, CVKTPJohn Ryan ParisNo ratings yet
- Peripheral Vascular DiseaseDocument32 pagesPeripheral Vascular DiseaseShy PatelNo ratings yet
- Tennis ElbowDocument13 pagesTennis ElbowPadma PadalNo ratings yet
- Arthrokinematics of Body Joints FinalDocument3 pagesArthrokinematics of Body Joints FinalnmahpbooksNo ratings yet
- Chest Physical Therapy Breathing ExercisesDocument28 pagesChest Physical Therapy Breathing ExercisesJulia SalvioNo ratings yet
- Polio Physiotherapy NotesDocument6 pagesPolio Physiotherapy NotesyigoNo ratings yet
- Cyriax IntroDocument14 pagesCyriax IntrodrrajmptnNo ratings yet
- Orthotic Prescription Factors for KAFODocument54 pagesOrthotic Prescription Factors for KAFOFERYANDA UTAMI100% (1)
- Bicipital TendonitisDocument2 pagesBicipital TendonitisJ Cheung100% (2)
- Role of Physiotherapy in Management of Burns-HshDocument25 pagesRole of Physiotherapy in Management of Burns-HshChristopher Chibueze Igbo100% (1)
- Low Back Pain Pearls of WisdomDocument33 pagesLow Back Pain Pearls of WisdomNaveed KhanNo ratings yet
- Neurological Assessment CaseDocument13 pagesNeurological Assessment Casedrrajmptn0% (1)
- Physiotherapy ManagementDocument16 pagesPhysiotherapy ManagementAlagappan ThiyagarajanNo ratings yet
- Complications of Bed Rest 1Document4 pagesComplications of Bed Rest 1Geetha Bhavani100% (1)
- Paraffin Wax BathDocument8 pagesParaffin Wax Bathbhavesh jain83% (6)
- Physiological Response To Immobility and ActivityDocument14 pagesPhysiological Response To Immobility and ActivitywalterNo ratings yet
- Modalities & Wound CareDocument0 pagesModalities & Wound CareAndika Laksmana KurniadiNo ratings yet
- Physiotherapy For Cardiac SurgeryDocument15 pagesPhysiotherapy For Cardiac SurgeryMuruganNo ratings yet
- Antenatal and Postnatal PPT PDFDocument15 pagesAntenatal and Postnatal PPT PDFNikita -0251 ENo ratings yet
- Hemiarthroplasty Hip - Apr20Document10 pagesHemiarthroplasty Hip - Apr20Shalu OjhaNo ratings yet
- Physical Therapy Board Review 1e by Brad Fortinberry PT DPT Scs Michael Dunaway PT 1560534974Document5 pagesPhysical Therapy Board Review 1e by Brad Fortinberry PT DPT Scs Michael Dunaway PT 1560534974Ivan CasaresNo ratings yet
- Articular NeurologyDocument11 pagesArticular NeurologyMitali ChhayaNo ratings yet
- Elbow JointDocument43 pagesElbow JointfagpatelNo ratings yet
- 10Document37 pages10fagpatel100% (1)
- 3Document18 pages3fagpatelNo ratings yet
- 6Document46 pages6fagpatelNo ratings yet
- 7Document38 pages7fagpatelNo ratings yet
- 2Document60 pages2fagpatel100% (2)
- 4Document34 pages4fagpatelNo ratings yet
- 1Document36 pages1fagpatel100% (1)
- Cervical Lymphoepithelial CystDocument6 pagesCervical Lymphoepithelial CystAhmed Al-jumailiNo ratings yet
- Delusional Jealusy - FullDocument17 pagesDelusional Jealusy - FullnicolasNo ratings yet
- NCM101 Health Assessment ExaminationDocument11 pagesNCM101 Health Assessment ExaminationJonah R. Merano100% (1)
- Autism Facts vs Myths: Debunking Common MisconceptionsDocument14 pagesAutism Facts vs Myths: Debunking Common Misconceptionsawardeco01No ratings yet
- Presented By: Meljyn Gomez Cuyos Dy, Arvie Jane Ederango, Nemia Bless Marjory, Epe Aizyl, FloresDocument32 pagesPresented By: Meljyn Gomez Cuyos Dy, Arvie Jane Ederango, Nemia Bless Marjory, Epe Aizyl, FloresJuviely PremacioNo ratings yet
- Safe SexDocument11 pagesSafe SexnathanNo ratings yet
- Smart + Smart Enhancer: Medic MedicDocument11 pagesSmart + Smart Enhancer: Medic MedicmiazainuddinNo ratings yet
- Windkessel EffectDocument11 pagesWindkessel EffectAkhmad HidayatNo ratings yet
- Effects of Malnutrition Among ChildrenDocument3 pagesEffects of Malnutrition Among ChildrenDesiree Aranggo MangueraNo ratings yet
- Necrotizing Soft Tissue Infections GuideDocument21 pagesNecrotizing Soft Tissue Infections GuideHen RyNo ratings yet
- Blood and Tissue Coccidian GuideDocument40 pagesBlood and Tissue Coccidian GuideMichael DawitNo ratings yet
- Basic pharmacology of anaesthesia drugs in 40 charactersDocument56 pagesBasic pharmacology of anaesthesia drugs in 40 charactersrajvikram87No ratings yet
- History of HIVDocument4 pagesHistory of HIVHyrum KamandeNo ratings yet
- Lesson 1Document20 pagesLesson 1Irish Jean AgsawayNo ratings yet
- CLUSTERS LIST - (CHNCS) GO-209Document45 pagesCLUSTERS LIST - (CHNCS) GO-209Gadde Srinivasarao67% (3)
- Experiment #2 - Unit TaskDocument2 pagesExperiment #2 - Unit TaskKagami TaigaNo ratings yet
- NCD High-Risk Assessment (Community Case Finding Form) NCD High-Risk Assessment (Community Case Finding Form)Document1 pageNCD High-Risk Assessment (Community Case Finding Form) NCD High-Risk Assessment (Community Case Finding Form)Claribel Domingo BayaniNo ratings yet
- Kali Bichromicum 30C For COPD 2005Document8 pagesKali Bichromicum 30C For COPD 2005Dr. Nancy MalikNo ratings yet
- Case Study 5 Year Boy With CoughDocument3 pagesCase Study 5 Year Boy With CoughAryl Eduarte100% (1)
- Health Declaration Form For ApplicantsDocument1 pageHealth Declaration Form For Applicantsgopeng glamping park malaysiaNo ratings yet
- English Intervention DialogueDocument3 pagesEnglish Intervention DialogueJihan Irbah TrianiNo ratings yet
- Chapter 15 - Hormones & Endocrine GlandsDocument17 pagesChapter 15 - Hormones & Endocrine Glandsapi-3728508100% (1)
- GROUP 10 Senstive Abt Food and Food AllergiesDocument16 pagesGROUP 10 Senstive Abt Food and Food AllergiesLilis nopita SarryNo ratings yet
- Introducing The Epidermis.: ReallyDocument47 pagesIntroducing The Epidermis.: ReallyNaila JinNo ratings yet