You might also like
- Atelectasis, (Lung Collapse) A Simple Guide To The Condition, Diagnosis, Treatment And Related DiseasesFrom EverandAtelectasis, (Lung Collapse) A Simple Guide To The Condition, Diagnosis, Treatment And Related DiseasesNo ratings yet
- Pleural Effusion, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandPleural Effusion, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Community Acquired Pneumonia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandCommunity Acquired Pneumonia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Pathophysiology ARDSDocument1 pagePathophysiology ARDSRoderick Agbuya100% (1)
- Acute Respiratory Distress Syndrome - PathophysiologyDocument5 pagesAcute Respiratory Distress Syndrome - PathophysiologyJoann67% (3)
- Acute Respiratory Distress SyndromeDocument3 pagesAcute Respiratory Distress SyndromeJorie Roco100% (1)
- Respiratory Care Review: An Intense Look at Respiratory Care Through Case StudiesFrom EverandRespiratory Care Review: An Intense Look at Respiratory Care Through Case StudiesNo ratings yet
- Ards Cmap FinalDocument4 pagesArds Cmap FinalPam Araune67% (3)
- Management of COPD in Primary and Secondary Care, TheFrom EverandManagement of COPD in Primary and Secondary Care, TheRating: 5 out of 5 stars5/5 (1)
- ARDS PresentationDocument89 pagesARDS Presentationalexandriaputera30No ratings yet
- Pathophysiology Acute Respiratory FailureDocument2 pagesPathophysiology Acute Respiratory FailureKimberly Regacho88% (8)
- Acute Respiratory Distress Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandAcute Respiratory Distress Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Acute Respiratory Distress SyndromeDocument9 pagesAcute Respiratory Distress SyndromeMatthew Ryan100% (2)
- ArdsDocument53 pagesArdsSophy Sony100% (3)
- Respiratory Failure, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandRespiratory Failure, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- PneumothoraxDocument57 pagesPneumothoraxCamille Marquez100% (9)
- COPD PathophysiologyDocument1 pageCOPD PathophysiologyJustin Ahorro-Dionisio33% (3)
- Pathophysiology of COPDDocument42 pagesPathophysiology of COPDRegineCuasSulib100% (3)
- Pathophysiology of COPD - The BasicsDocument11 pagesPathophysiology of COPD - The BasicstiaranindyNo ratings yet
- RT!: Reflections on a Career in Respiratory TherapyFrom EverandRT!: Reflections on a Career in Respiratory TherapyRating: 3 out of 5 stars3/5 (1)
- Severe Sepsis and Septic ShockDocument39 pagesSevere Sepsis and Septic ShockYogi Agil MurdjitoNo ratings yet
- Acute Respiratory FailureDocument17 pagesAcute Respiratory FailurejulianajosNo ratings yet
- COPD PATHOPHYSIOLOGY DiagramDocument2 pagesCOPD PATHOPHYSIOLOGY Diagramcris_198893% (15)
- Bronchiectasis PathophysiologyDocument1 pageBronchiectasis PathophysiologyRayne Dunstan Pascual VergaraNo ratings yet
- PathophysiologyDocument4 pagesPathophysiologyCee SanchezNo ratings yet
- Acute Respiratory Failure Pa Tho PhysiologyDocument4 pagesAcute Respiratory Failure Pa Tho Physiologyroseanne18100% (4)
- Pleural EffusionDocument3 pagesPleural EffusionRafahiah HaronNo ratings yet
- Pathophysiology ARDSDocument2 pagesPathophysiology ARDSKim AmboyaNo ratings yet
- Pathophysiology of PneumothoraxDocument2 pagesPathophysiology of Pneumothoraxoxidalaj84% (19)
- COPD PathoDocument1 pageCOPD PathoLeah May AnchetaNo ratings yet
- Acute Respiratory Distress SyndromeDocument31 pagesAcute Respiratory Distress Syndromegretchen marie100% (1)
- Chronic Obstructive Pulmonary Disease: Patient Population: ObjectivesDocument28 pagesChronic Obstructive Pulmonary Disease: Patient Population: Objectivesdoni anandaNo ratings yet
- COPDDocument52 pagesCOPDswapnil3250No ratings yet
- Respiratory FailureDocument16 pagesRespiratory FailurealzaabiBMNo ratings yet
- Acute Bronchitis Case StudyDocument6 pagesAcute Bronchitis Case Studyulka0750% (2)
- Hypovolemic ShockDocument8 pagesHypovolemic ShockLyka Flores100% (1)
- COPD ExacerbationDocument12 pagesCOPD ExacerbationJeffrey ShermanNo ratings yet
- Acute Respiratory Distress SyndromeDocument17 pagesAcute Respiratory Distress SyndromeSanjeet SahNo ratings yet
- Case Study - EmphysemaDocument6 pagesCase Study - Emphysemamackie_041992No ratings yet
- Chronic Obstructive Pulmonary DiseaseDocument10 pagesChronic Obstructive Pulmonary DiseaseZinya RobinsonNo ratings yet
- Drug Study in PneumoniaDocument17 pagesDrug Study in PneumoniaKara Kathrina FuentesNo ratings yet
- COPDDocument26 pagesCOPDburjay100% (3)
- BRONCHIECTASISDocument36 pagesBRONCHIECTASISNishanth ReddyNo ratings yet
- Acute Respiratory Failure 375Document65 pagesAcute Respiratory Failure 375Ahsan Javed100% (1)
- Pulmonary HypertensionDocument10 pagesPulmonary HypertensionqingwenNo ratings yet
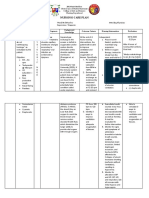
- Cues Nursing Diagnosis Scientific Rationale Goals Nursing Interventions Rationale EvaluationDocument3 pagesCues Nursing Diagnosis Scientific Rationale Goals Nursing Interventions Rationale EvaluationIngrid Nicolas100% (1)
- Acute Respiratory Distress Syndrome (ARDS)Document72 pagesAcute Respiratory Distress Syndrome (ARDS)desyNo ratings yet
- Stevens Johnson Syndrome CASEDocument53 pagesStevens Johnson Syndrome CASEKathrina CraveNo ratings yet
- ArdsDocument81 pagesArdsAmit KlNo ratings yet
- Angina PectorisDocument12 pagesAngina Pectorismardsz93% (14)
- Acute Respiratory FailureDocument2 pagesAcute Respiratory FailurePaolo Luis MontenegroNo ratings yet
- Acute Respiratory Distress SyndromeDocument70 pagesAcute Respiratory Distress SyndromeAndrea Del Villar100% (1)
- Pneumonia Case StudyDocument5 pagesPneumonia Case StudycrisolandNo ratings yet
- (Cor Pulmonale) PATHOPHYSIOLOGYDocument2 pages(Cor Pulmonale) PATHOPHYSIOLOGYmilayango67% (3)
- Pathophysiology of PneumoniaDocument2 pagesPathophysiology of PneumoniaIrene Demegillo SalongaNo ratings yet
- 16 ARDS - Nursing Care ManagementDocument2 pages16 ARDS - Nursing Care ManagementTisha CarretteNo ratings yet
- Covid NCPDocument6 pagesCovid NCPNathalia Cabalse100% (2)
- Acute Respiratory Distress SyndromeDocument36 pagesAcute Respiratory Distress Syndromedr9348345000No ratings yet
- Acute Respiratory Failure For StudentDocument41 pagesAcute Respiratory Failure For Studentapi-379952350% (4)
- Lymphomas With PathophysiologyDocument30 pagesLymphomas With Pathophysiologymabec pagaduan91% (11)
- Leukemia With PathophysiologyDocument34 pagesLeukemia With Pathophysiologymabec pagaduan90% (41)
- ANEMIAS (Sickle Cell Anemia With Pathophysiology)Document31 pagesANEMIAS (Sickle Cell Anemia With Pathophysiology)mabec pagaduan70% (10)
- Disseminated Intravascular Coagulation With PathophysiologyDocument18 pagesDisseminated Intravascular Coagulation With Pathophysiologymabec pagaduan100% (6)
- Multiple Myeloma With PathophysiologyDocument32 pagesMultiple Myeloma With Pathophysiologymabec pagaduan90% (10)
- Oxygen Delivery DevicesDocument19 pagesOxygen Delivery DevicesJaya PrabhaNo ratings yet
- CPR Reporting FormDocument3 pagesCPR Reporting FormRaghvendra singhNo ratings yet
- Selina Concise Biology Solutions Class 6 Chapter 5 Respiratory SystemDocument10 pagesSelina Concise Biology Solutions Class 6 Chapter 5 Respiratory SystemFLANTAMOCKNo ratings yet
- Respiratory and Excretory System ReviewDocument27 pagesRespiratory and Excretory System ReviewJoyce Catherine Buquing UysecoNo ratings yet
- RT Equations Handout: VA (VT-VD) F Normal Is 4-6 L/minDocument15 pagesRT Equations Handout: VA (VT-VD) F Normal Is 4-6 L/minMaria Mercedes AlegreNo ratings yet
- Nursing Respiratory SystemDocument254 pagesNursing Respiratory SystemWendy EvansNo ratings yet
- Respiratory System LessomDocument7 pagesRespiratory System LessomDaliah Wedderburn100% (1)
- Arterial Blood GasDocument12 pagesArterial Blood Gasعزالدين الزوقريNo ratings yet
- Spesifikasi Ventilator Draeger Savina 300 (CO2) : Items DescriptionDocument2 pagesSpesifikasi Ventilator Draeger Savina 300 (CO2) : Items DescriptionAnonymous 7RJm3Aw5DNo ratings yet
- Poseidon Product Range 2021-1-sc811Document29 pagesPoseidon Product Range 2021-1-sc811Урош ypow ypocNo ratings yet
- Relaxation ResponseDocument3 pagesRelaxation ResponseANNA MAE PANONo ratings yet
- PMVDocument28 pagesPMVRajesh VermaNo ratings yet
- RESPI QuestionDocument14 pagesRESPI QuestionPrince Charles AbalosNo ratings yet
- The Six Minute Walk TestDocument4 pagesThe Six Minute Walk Testhm3398No ratings yet
- One Lung Ventilation: General Principles - UpToDateDocument26 pagesOne Lung Ventilation: General Principles - UpToDateAna Belén Artero CastañoNo ratings yet
- Administering Oxygen Therapy Powerpoint 3Document58 pagesAdministering Oxygen Therapy Powerpoint 3RajaNo ratings yet
- Ventilation, Perfusion and Ventilation-Perfusion RelationshipsDocument14 pagesVentilation, Perfusion and Ventilation-Perfusion RelationshipspuchioNo ratings yet
- AsthmaDocument10 pagesAsthmaSameera banuNo ratings yet
- Mang Kanor ANAPHYDocument1 pageMang Kanor ANAPHYChamelli RobinNo ratings yet
- Atelectasis Right LungDocument24 pagesAtelectasis Right Lungnirnay10No ratings yet
- Pediatric Chest PhysiotherapyDocument25 pagesPediatric Chest PhysiotherapyShubha DiwakarNo ratings yet
- A Seminar On Intermittent Positive Airway Pressure BreathingDocument19 pagesA Seminar On Intermittent Positive Airway Pressure BreathingPatrizeNo ratings yet
- Recognizing Interstitial Versus Airspace Disease: in Slide Show Mode, Advance The Slides by Pressing The SpacebarDocument32 pagesRecognizing Interstitial Versus Airspace Disease: in Slide Show Mode, Advance The Slides by Pressing The SpacebarCheska TumulakNo ratings yet
- NEW CHECKLIST Endotracheal or Tracheal SuctioningDocument4 pagesNEW CHECKLIST Endotracheal or Tracheal SuctioningDan Dan ManaoisNo ratings yet
- Endotracheal IntubationDocument7 pagesEndotracheal Intubationsimonjosan67% (3)
- What Is Respiratory Alkalosis?Document3 pagesWhat Is Respiratory Alkalosis?Lorenn AdarnaNo ratings yet
- Form 3 Chapter 1Document6 pagesForm 3 Chapter 1naza977590% (29)
- Test Bank For Mechanical Ventilation 7th Edition J M CairoDocument13 pagesTest Bank For Mechanical Ventilation 7th Edition J M CairocalliopesilasaagyNo ratings yet
- F4Bio (C8) NotesDocument11 pagesF4Bio (C8) NotesGrace LeeNo ratings yet
- ACLS Provider Manual Supplementary Material: © 2020 American Heart AssociationDocument75 pagesACLS Provider Manual Supplementary Material: © 2020 American Heart AssociationpolelNo ratings yet