You might also like
- Seminar Health Care DeliveryDocument39 pagesSeminar Health Care DeliveryangayarkanniNo ratings yet
- National Family Welfare ProgrammeDocument64 pagesNational Family Welfare ProgrammeNityananda Pattanaik67% (3)
- EDUCATIONAL PREPARATIO ShitalDocument28 pagesEDUCATIONAL PREPARATIO ShitalKinjal Vasava100% (2)
- National Family Welfare ProgramDocument27 pagesNational Family Welfare ProgramBhawna JoshiNo ratings yet
- Janni Surakha YojanaDocument18 pagesJanni Surakha YojanaNeelofur Ibran AliNo ratings yet
- National Health and Family Welfare ProgrammesDocument17 pagesNational Health and Family Welfare ProgrammesSandhya s67% (3)
- Biologic and Psychosocial Dynamics in Disease CausationDocument35 pagesBiologic and Psychosocial Dynamics in Disease Causationlivelinami100% (4)
- Health Agencies NGOs Roles and FunctionsDocument23 pagesHealth Agencies NGOs Roles and FunctionsNandhiniC100% (3)
- Training and Supervision OF HEALTH WORKERSDocument27 pagesTraining and Supervision OF HEALTH WORKERSkrupa mathewNo ratings yet
- TelemedicineDocument23 pagesTelemedicineNedhi Singh100% (2)
- Pattern of Nursing Education in IndiaDocument22 pagesPattern of Nursing Education in IndiaSathish Rajamani67% (6)
- Preparation of Professional Teacher Organizing Professional Aspects of Teacher Preparation ProgramsDocument27 pagesPreparation of Professional Teacher Organizing Professional Aspects of Teacher Preparation ProgramsGaoudam Natarajan50% (4)
- Nurses in Implementation of National Rural Health Mission: Dr. Pratima Mittra Sr. Consultant, RCH - Ii / NRHM NihfwDocument32 pagesNurses in Implementation of National Rural Health Mission: Dr. Pratima Mittra Sr. Consultant, RCH - Ii / NRHM NihfwPabhat KumarNo ratings yet
- National Health and Family Welfare Programme: HistoryDocument2 pagesNational Health and Family Welfare Programme: HistorySree Latha100% (1)
- Critical Analysis of M.sc. Program of Teacher Education in IndiaDocument13 pagesCritical Analysis of M.sc. Program of Teacher Education in Indiakiran mahal76% (17)
- National Population Policy 2000 Lect.Document28 pagesNational Population Policy 2000 Lect.livelinamiNo ratings yet
- Major Stakeholders in Health Care SystemDocument5 pagesMajor Stakeholders in Health Care SystemANITTA S100% (1)
- Health Problems in IndiaDocument18 pagesHealth Problems in IndiahemihemaNo ratings yet
- CHN Adolescent HealthDocument25 pagesCHN Adolescent Healthprabha krishnan100% (1)
- Nursing Education in India: ANM, GNM, B.SC and PBB - SCDocument19 pagesNursing Education in India: ANM, GNM, B.SC and PBB - SCPrasanth Kurien Mathew100% (24)
- Research Priorities in Obstetrics SeminarDocument7 pagesResearch Priorities in Obstetrics SeminarSharmistha Debnath83% (6)
- Nursing Council of India SIU Norms For Staffing (Nurse)Document2 pagesNursing Council of India SIU Norms For Staffing (Nurse)CMS SGPGI100% (2)
- Concept of Faculty Supervisior in Dual PositionDocument18 pagesConcept of Faculty Supervisior in Dual PositionDeepa83% (6)
- On Epidemological Aspects of Maternal and Child HealthDocument30 pagesOn Epidemological Aspects of Maternal and Child HealthBisma Maqbool67% (3)
- Changing Focus of CareDocument38 pagesChanging Focus of CareManoj BalaNo ratings yet
- Practice Standards For Obstetric and Gynaecological UnitDocument27 pagesPractice Standards For Obstetric and Gynaecological UnitRDi J100% (1)
- Health Care Envt, Constraints, Policies, Planning Economics and Political Vis-A-VisDocument18 pagesHealth Care Envt, Constraints, Policies, Planning Economics and Political Vis-A-VisDishu100% (8)
- Educational Aims and Objectives-2Document22 pagesEducational Aims and Objectives-2Shruthi Pingula100% (2)
- Family Welfare Programme in IndiaDocument25 pagesFamily Welfare Programme in IndiaTirumalesha DadigeNo ratings yet
- SBA MODULE Guideline For Antenatal CareDocument80 pagesSBA MODULE Guideline For Antenatal CareTmanoj Praveen33% (3)
- Unit 1: Community Health NursingDocument56 pagesUnit 1: Community Health NursingNishaAhsinNo ratings yet
- Presentation ON Health Committee: Submitted To: Mrs. Krishnaveni M.SC (NSG) (Lecturar)Document16 pagesPresentation ON Health Committee: Submitted To: Mrs. Krishnaveni M.SC (NSG) (Lecturar)Krishnaveni Murugesh100% (1)
- Training & Supervision of Various Categories of Health WorkersDocument52 pagesTraining & Supervision of Various Categories of Health WorkersAparna Kingini100% (4)
- Preventive Obstetrics: Presented By-Itismita Biswal M, Sc. Nursing (1) Yr Obstetrics & Gynaecological NursingDocument20 pagesPreventive Obstetrics: Presented By-Itismita Biswal M, Sc. Nursing (1) Yr Obstetrics & Gynaecological NursingPabhat Kumar89% (9)
- Master Rotation PlanDocument10 pagesMaster Rotation PlanAnonymous 0C4OZmR100% (2)
- Nursing Care For Special Groups:Children, Adolescents, Adult, Woman and ElderlyDocument10 pagesNursing Care For Special Groups:Children, Adolescents, Adult, Woman and Elderlypramod kumawatNo ratings yet
- Esi Scheme and CGHS: Mrs. Namita Batra Guin Associate Professor Deptt. of Community Health NursingDocument19 pagesEsi Scheme and CGHS: Mrs. Namita Batra Guin Associate Professor Deptt. of Community Health NursinglivelinamiNo ratings yet
- Importance of Liberal Education in NursingDocument20 pagesImportance of Liberal Education in NursingKomala Rajagopal100% (2)
- Health Planning in IndiaDocument66 pagesHealth Planning in Indiarajatsgr75% (4)
- Epidermological Aspects of Meternal and Child Health Unit 1Document24 pagesEpidermological Aspects of Meternal and Child Health Unit 1Pruthvi100% (4)
- Nursing Practice Framework Scope and TrendsDocument9 pagesNursing Practice Framework Scope and TrendsAru Verma100% (3)
- Health SchemesDocument21 pagesHealth SchemesPankaj Khatri100% (1)
- MissionDocument56 pagesMissionPriyaNo ratings yet
- Patterns of Nursing EducationDocument34 pagesPatterns of Nursing EducationIze C Viji94% (17)
- National Education PolicyDocument34 pagesNational Education Policysona100% (1)
- Problem Statements PresentationDocument7 pagesProblem Statements PresentationAaliyaan KhanNo ratings yet
- History of Development of Nursing Profession J CharacteristicsDocument28 pagesHistory of Development of Nursing Profession J CharacteristicsSushma SwathiNo ratings yet
- Seminar On Skilled Birth SBA ModuleDocument50 pagesSeminar On Skilled Birth SBA ModuleSangita Patir83% (40)
- Role - of - Curriculum - Coordinator 3Document8 pagesRole - of - Curriculum - Coordinator 3kamini Choudhary100% (1)
- Epidemiological Aspects of Maternal and Child Health and Its Issues Word ContentDocument40 pagesEpidemiological Aspects of Maternal and Child Health and Its Issues Word ContentNimi Simon100% (2)
- MiesDocument40 pagesMiessanthiyasandyNo ratings yet
- Trainng and Supervision of Health WorkerDocument14 pagesTrainng and Supervision of Health WorkershivaniNo ratings yet
- CHN Lessonplan (NRHM - National Rural Health Mission)Document23 pagesCHN Lessonplan (NRHM - National Rural Health Mission)Samjhana Neupane100% (5)
- Critical Evaluation GNMDocument7 pagesCritical Evaluation GNMManisha Samson100% (2)
- Framework, Scope and TrendsDocument25 pagesFramework, Scope and TrendsKinjal Vasava100% (5)
- Trends in Development of Nursing Education in IndiaDocument22 pagesTrends in Development of Nursing Education in IndiaShyam82% (11)
- India: Current State of HealthcareDocument15 pagesIndia: Current State of HealthcareYadav MannuNo ratings yet
- Rural Health in Andhra PradeshDocument5 pagesRural Health in Andhra PradeshInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Unit Wise Question Will Come in Final Exam Unit 1: Q 2 ObjectivesDocument54 pagesUnit Wise Question Will Come in Final Exam Unit 1: Q 2 ObjectivesPoonam Yadav roll no.53No ratings yet
- Review-Health Systems in India PDFDocument4 pagesReview-Health Systems in India PDFTehMarianNo ratings yet
- Spencer Glatt - Consultant Agreement - Please Have Consultant Sign - 2816200 1Document2 pagesSpencer Glatt - Consultant Agreement - Please Have Consultant Sign - 2816200 1api-535837127No ratings yet
- 071 Firouzeh SepehrianazarDocument6 pages071 Firouzeh SepehrianazarТеодора ДелићNo ratings yet
- Babcock - Student Application SANDRA NWENEDocument2 pagesBabcock - Student Application SANDRA NWENEnwenes5258No ratings yet
- MUHAMMAD AFFAN BASHIR (SR Reliability Engineer)Document2 pagesMUHAMMAD AFFAN BASHIR (SR Reliability Engineer)darff45No ratings yet
- ConstructivismDocument18 pagesConstructivismJeson A. LongnoNo ratings yet
- Field Study - Ep 2Document5 pagesField Study - Ep 2larenNo ratings yet
- Time Management - TALKDocument22 pagesTime Management - TALKmitch sapladaNo ratings yet
- Grade R Lesson PlanDocument4 pagesGrade R Lesson PlanMegan Parker100% (4)
- Delta Theta Book of RecordsDocument398 pagesDelta Theta Book of RecordsareyoubeefinNo ratings yet
- Üds 2011 Sosyal Ilkbahar MartDocument16 pagesÜds 2011 Sosyal Ilkbahar MartDr. Hikmet ŞahinerNo ratings yet
- The Onto-Semiotic Approach To Research in MathematDocument10 pagesThe Onto-Semiotic Approach To Research in Mathematsamuel carreroNo ratings yet
- Standard: Running Record Case StudyDocument2 pagesStandard: Running Record Case Studymichelleangel14No ratings yet
- SSI3013 Information and Communication Technology in Science: Name Matric NumberDocument7 pagesSSI3013 Information and Communication Technology in Science: Name Matric NumberSiang KeeNo ratings yet
- Joram Mariga and Stone SculptureDocument6 pagesJoram Mariga and Stone SculpturePeter Tapiwa TichagwaNo ratings yet
- AIOU 8613 SampleDocument4 pagesAIOU 8613 SampleAhmed Ali100% (3)
- 8 класс планDocument2 pages8 класс планmukhtar6103No ratings yet
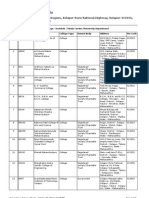
- InstituteCollegeStudyCenter 29102012014438PMDocument7 pagesInstituteCollegeStudyCenter 29102012014438PMAmir WagdarikarNo ratings yet
- HEE Topol Review 2019Document53 pagesHEE Topol Review 2019Roger SenNo ratings yet
- Plumbing History of The PhilippinesDocument4 pagesPlumbing History of The Philippinesjuan dela cruzNo ratings yet
- The Eagle Lesson PlanDocument33 pagesThe Eagle Lesson PlanVirgilio Rosario BiagtanNo ratings yet
- Weekly Home Learning Plan Grade 6-Justice: Schools Division of Misamis Oriental Kimaya Integrated SchoolDocument16 pagesWeekly Home Learning Plan Grade 6-Justice: Schools Division of Misamis Oriental Kimaya Integrated SchoolDaling JessaNo ratings yet
- The Correlation Between Time Spent in Studying and Academic AchievementDocument23 pagesThe Correlation Between Time Spent in Studying and Academic AchievementRizza100% (3)
- Eligible Candidates List For MD MS Course CLC Round 2 DME PG Counselling 2023Document33 pagesEligible Candidates List For MD MS Course CLC Round 2 DME PG Counselling 2023Dr. Vishal SengarNo ratings yet
- National/Caribbean Vocational Qualification (N/CVQ) Evidence Achievement Record SheetDocument2 pagesNational/Caribbean Vocational Qualification (N/CVQ) Evidence Achievement Record Sheetddmarshall2838No ratings yet
- Lesson3 Polyrhythmic Drumming Styles Japan BrazilDocument5 pagesLesson3 Polyrhythmic Drumming Styles Japan BrazilJonathan SpinksNo ratings yet
- Portfolio ReflectionDocument2 pagesPortfolio Reflectionapi-527915551No ratings yet
- Impact of OC and LeadershipDocument8 pagesImpact of OC and Leadershiperrytrina putriNo ratings yet
- Engaging Senior High School Students Through Competitive CollaborationDocument5 pagesEngaging Senior High School Students Through Competitive Collaborationjanapearl.jintalanNo ratings yet
- Graded AssertivenessDocument7 pagesGraded AssertivenessLisaNo ratings yet
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisFrom EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (9)
- Workin' Our Way Home: The Incredible True Story of a Homeless Ex-Con and a Grieving Millionaire Thrown Together to Save Each OtherFrom EverandWorkin' Our Way Home: The Incredible True Story of a Homeless Ex-Con and a Grieving Millionaire Thrown Together to Save Each OtherNo ratings yet
- You Can't Joke About That: Why Everything Is Funny, Nothing Is Sacred, and We're All in This TogetherFrom EverandYou Can't Joke About That: Why Everything Is Funny, Nothing Is Sacred, and We're All in This TogetherNo ratings yet
- When Helping Hurts: How to Alleviate Poverty Without Hurting the Poor . . . and YourselfFrom EverandWhen Helping Hurts: How to Alleviate Poverty Without Hurting the Poor . . . and YourselfRating: 5 out of 5 stars5/5 (36)
- The House at Pooh Corner - Winnie-the-Pooh Book #4 - UnabridgedFrom EverandThe House at Pooh Corner - Winnie-the-Pooh Book #4 - UnabridgedRating: 4.5 out of 5 stars4.5/5 (5)
- Uncontrolled Spread: Why COVID-19 Crushed Us and How We Can Defeat the Next PandemicFrom EverandUncontrolled Spread: Why COVID-19 Crushed Us and How We Can Defeat the Next PandemicNo ratings yet
- High-Risers: Cabrini-Green and the Fate of American Public HousingFrom EverandHigh-Risers: Cabrini-Green and the Fate of American Public HousingNo ratings yet
- Do You Believe in Magic?: The Sense and Nonsense of Alternative MedicineFrom EverandDo You Believe in Magic?: The Sense and Nonsense of Alternative MedicineNo ratings yet
- The Importance of Being Earnest: Classic Tales EditionFrom EverandThe Importance of Being Earnest: Classic Tales EditionRating: 4.5 out of 5 stars4.5/5 (44)
- The Great Displacement: Climate Change and the Next American MigrationFrom EverandThe Great Displacement: Climate Change and the Next American MigrationRating: 4.5 out of 5 stars4.5/5 (32)
- Welcome to the United States of Anxiety: Observations from a Reforming NeuroticFrom EverandWelcome to the United States of Anxiety: Observations from a Reforming NeuroticRating: 3.5 out of 5 stars3.5/5 (10)
- The Meth Lunches: Food and Longing in an American CityFrom EverandThe Meth Lunches: Food and Longing in an American CityRating: 5 out of 5 stars5/5 (5)
- Life at the Bottom: The Worldview That Makes the UnderclassFrom EverandLife at the Bottom: The Worldview That Makes the UnderclassRating: 5 out of 5 stars5/5 (30)
- The Book of Bad:: Stuff You Should Know Unless You’re a PussyFrom EverandThe Book of Bad:: Stuff You Should Know Unless You’re a PussyRating: 3.5 out of 5 stars3.5/5 (3)
- The Comedians in Cars Getting Coffee BookFrom EverandThe Comedians in Cars Getting Coffee BookRating: 4.5 out of 5 stars4.5/5 (8)
- Deaths of Despair and the Future of CapitalismFrom EverandDeaths of Despair and the Future of CapitalismRating: 4.5 out of 5 stars4.5/5 (30)
- The Inimitable Jeeves [Classic Tales Edition]From EverandThe Inimitable Jeeves [Classic Tales Edition]Rating: 5 out of 5 stars5/5 (3)
- The Most Forbidden Knowledge: 151 Things NO ONE Should Know How to DoFrom EverandThe Most Forbidden Knowledge: 151 Things NO ONE Should Know How to DoRating: 4.5 out of 5 stars4.5/5 (6)