You might also like
- PWD DiscountsDocument8 pagesPWD DiscountsJason TiongcoNo ratings yet
- Cabael Motion For Additional Time To File Memorandum UploadDocument2 pagesCabael Motion For Additional Time To File Memorandum UploadMelvin Jones100% (1)
- NAB Motion To DeferDocument7 pagesNAB Motion To DeferBrendan SassoNo ratings yet
- Dacion en Pago AgreementDocument3 pagesDacion en Pago AgreementHannah Quinones100% (1)
- Preliminary Advice of Loss FormDocument1 pagePreliminary Advice of Loss FormWai Leong Edward Low0% (1)
- Admin Case Against A JudgeDocument4 pagesAdmin Case Against A JudgeMenchie DumaganNo ratings yet
- Property Management Agreement: BackgroundDocument8 pagesProperty Management Agreement: BackgroundAdesinaNo ratings yet
- Rulings On Company Doctor Vs Seafarers DoctorDocument4 pagesRulings On Company Doctor Vs Seafarers DoctorcesarjruyNo ratings yet
- Print Motion To Admit CafsDocument5 pagesPrint Motion To Admit CafsGerard LeeNo ratings yet
- 181 and 182 Vs Carmel Maynilad - Reply Opposition To MTD (02 June 2015)Document13 pages181 and 182 Vs Carmel Maynilad - Reply Opposition To MTD (02 June 2015)ᜉᜂᜎᜊᜒᜀᜃ ᜎᜓᜌᜓᜎNo ratings yet
- M. MischiefDocument18 pagesM. MischiefStefViolaNo ratings yet
- Hoa Annual Meeting Agenda 2021Document1 pageHoa Annual Meeting Agenda 2021api-26988931No ratings yet
- Memo CertiorariDocument31 pagesMemo CertiorariMiklosNo ratings yet
- Accomplishment Report 2Document2 pagesAccomplishment Report 2queen malikNo ratings yet
- RA 10354 Petition SC James ImbongDocument25 pagesRA 10354 Petition SC James ImbongCBCP for LifeNo ratings yet
- Collateral Attack On PropertyDocument10 pagesCollateral Attack On PropertyRommel TottocNo ratings yet
- Wood Technology Corp v. Equitable Bank G.R. 153867Document6 pagesWood Technology Corp v. Equitable Bank G.R. 153867Dino Bernard LapitanNo ratings yet
- Application For Amendment of Master Deed With Declaration of RestrictionsDocument1 pageApplication For Amendment of Master Deed With Declaration of RestrictionsNiel DeygabiNo ratings yet
- Chapter 1 Cases RianoDocument479 pagesChapter 1 Cases RianoAnonymous 4WA9UcnU2XNo ratings yet
- Formal Invitation LetterDocument1 pageFormal Invitation LetterTriyono SoepardiNo ratings yet
- VERA Files's Letter To Antipolo City Legal OfficeDocument1 pageVERA Files's Letter To Antipolo City Legal OfficeVERA FilesNo ratings yet
- Justification LetterDocument1 pageJustification LetterDennis DagoocNo ratings yet
- Accion Publiciana Is The Plenary Action To Recover The Right of PossessionDocument3 pagesAccion Publiciana Is The Plenary Action To Recover The Right of PossessionTosca MansujetoNo ratings yet
- 1989 Darab RulesDocument17 pages1989 Darab RulesJay-r RbarNo ratings yet
- Job Acceptance Letter 03Document1 pageJob Acceptance Letter 03Enock DadzieNo ratings yet
- Petition (Marcial Vs Hon Lerio Castigador CA Final)Document12 pagesPetition (Marcial Vs Hon Lerio Castigador CA Final)felix reyesNo ratings yet
- Republic of The Philippines Department of Transportation Land Transportation Franchising and Regulatory Board Regional OfficeDocument3 pagesRepublic of The Philippines Department of Transportation Land Transportation Franchising and Regulatory Board Regional OfficeAtty. Cca MagallanesNo ratings yet
- Answer With Counterclaims COMES NOW DefendantDocument6 pagesAnswer With Counterclaims COMES NOW DefendantRab Thomas BartolomeNo ratings yet
- Demand Letter Dated 08 August 2022Document2 pagesDemand Letter Dated 08 August 2022theresa bautistaNo ratings yet
- Memorandum of Understanding Davao and Handicap International PDFDocument9 pagesMemorandum of Understanding Davao and Handicap International PDFZac CatulongNo ratings yet
- Domain Name & Web Hosting: 383 9224, Unit 4 Zeraus BLDG., Gorordo AvenueDocument1 pageDomain Name & Web Hosting: 383 9224, Unit 4 Zeraus BLDG., Gorordo AvenueRheneir MoraNo ratings yet
- Opposition To Formal Offer MalversationDocument5 pagesOpposition To Formal Offer MalversationJeremy MorenoNo ratings yet
- Laboratory Activity 7 - HIS Lab - iHOMISDocument2 pagesLaboratory Activity 7 - HIS Lab - iHOMISCaissa Andrea Beatrice BaylenNo ratings yet
- ESTRADA V SandinganbayanDocument24 pagesESTRADA V SandinganbayanJoyleen HebronNo ratings yet
- Coc Appeal Application FormDocument2 pagesCoc Appeal Application FormBalaraman100% (1)
- Motion To Permanently Dismissed 1Document2 pagesMotion To Permanently Dismissed 1Jayson AbreraNo ratings yet
- National Labor Relations CommissionDocument8 pagesNational Labor Relations CommissionChloe Sy GalitaNo ratings yet
- Date - : RE: Notice of Returned Check With Demand To Settle Outstanding ObligationDocument1 pageDate - : RE: Notice of Returned Check With Demand To Settle Outstanding ObligationRomak TranceNo ratings yet
- LWUADocument4 pagesLWUARALSTON TUYOKNo ratings yet
- Affidavit - Arlyn Parreno RevlamDocument5 pagesAffidavit - Arlyn Parreno RevlamLowell MadrilenoNo ratings yet
- CABAGTONG - Position Paper 1Document6 pagesCABAGTONG - Position Paper 1Gerald HernandezNo ratings yet
- Cancellation Motion For ExtensionDocument11 pagesCancellation Motion For ExtensionGhadahNo ratings yet
- Republic of The Philippines Court of Appeals Manila: PetitionersDocument12 pagesRepublic of The Philippines Court of Appeals Manila: PetitionersNetweightNo ratings yet
- Attestation Form TemplateDocument1 pageAttestation Form TemplateconsiNo ratings yet
- Data Privacy Act Form 1Document1 pageData Privacy Act Form 1Irene ToNo ratings yet
- Draft New Template Warrant of ArrestDocument1 pageDraft New Template Warrant of Arrestjanys22No ratings yet
- Acts of Lasciviousness-2Document3 pagesActs of Lasciviousness-2MonicaNo ratings yet
- LOG-2-6-WAREHOUSE-TEMPLATE-Warehouse Rental Contract-RCRCS PDFDocument3 pagesLOG-2-6-WAREHOUSE-TEMPLATE-Warehouse Rental Contract-RCRCS PDFG Vishwanath ReddyNo ratings yet
- MOTION TO REDUCE BAIL TigasDocument2 pagesMOTION TO REDUCE BAIL TigasAike SadjailNo ratings yet
- People vs. Malasoma - Authority To ProsecuteDocument1 pagePeople vs. Malasoma - Authority To ProsecuteChevrolie Maglasang-IsotoNo ratings yet
- Memorandum MonterealDocument6 pagesMemorandum MonterealKING ANTHONY MONTEREALNo ratings yet
- War crimes and crimes against humanity in the Rome Statute of the International Criminal CourtFrom EverandWar crimes and crimes against humanity in the Rome Statute of the International Criminal CourtNo ratings yet
- Appellan'ts Brief CRIM (TO SC)Document7 pagesAppellan'ts Brief CRIM (TO SC)bobbyrickyNo ratings yet
- Case Management Conference CGC 15 547125Document1 pageCase Management Conference CGC 15 547125L. A. PatersonNo ratings yet
- RD Request - Michael Jayson L. Dy 1.28.13Document1 pageRD Request - Michael Jayson L. Dy 1.28.13George MelitsNo ratings yet
- Sample Minutes of HearingDocument3 pagesSample Minutes of HearingRaymond Jade Ravelo SilvosaNo ratings yet
- 04 Real Estate Service ActDocument21 pages04 Real Estate Service ActClarkNo ratings yet
- Rule On Precautionary Hold Departure OrderDocument12 pagesRule On Precautionary Hold Departure OrderGeremae MataNo ratings yet
- 2016 Revised Rules On Small Claims - Sample FormsDocument34 pages2016 Revised Rules On Small Claims - Sample FormsMa. Angelica de GuzmanNo ratings yet
- Walking a Tightrope: Biography of Honorable Mayor Catalino Gabot Hermosilla Sr.From EverandWalking a Tightrope: Biography of Honorable Mayor Catalino Gabot Hermosilla Sr.No ratings yet
- Ra 10354Document13 pagesRa 10354CBCP for LifeNo ratings yet
- PhilHealth Circular No. 0035, s.2013 Annex 1 List of Medical Case RatesDocument111 pagesPhilHealth Circular No. 0035, s.2013 Annex 1 List of Medical Case RatesChrysanthus Herrera80% (5)
- PhilHealth Circular No. 0035, s.2013 Annex 10 List of Alternative Documents For Record of Operative or Surgical TechniqueDocument14 pagesPhilHealth Circular No. 0035, s.2013 Annex 10 List of Alternative Documents For Record of Operative or Surgical TechniqueChrysanthus HerreraNo ratings yet
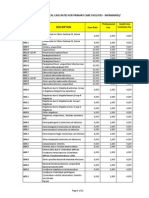
- PhilHealth Circular No. 0035, s.2013 Annex 6 List of Procedure CaseRates For Primary Care FacilitiesDocument22 pagesPhilHealth Circular No. 0035, s.2013 Annex 6 List of Procedure CaseRates For Primary Care FacilitiesChrysanthus Herrera100% (2)
- CF1Document1 pageCF1Kim ViñasNo ratings yet
- PhilHealth Circular No. 0035, s.2013 Annex 2 List of Procedure Case RatesDocument98 pagesPhilHealth Circular No. 0035, s.2013 Annex 2 List of Procedure Case RatesChrysanthus Herrera50% (2)
- PhilHealth Circular No. 0035, s.2013 Annex 4 Examples and Scenarios For The All Case Rates Implementing GuidelinesDocument7 pagesPhilHealth Circular No. 0035, s.2013 Annex 4 Examples and Scenarios For The All Case Rates Implementing GuidelinesChrysanthus HerreraNo ratings yet
- PhilHealth Circular No. 0035, s.2013 Annex 3 List of Medical Conditions and Procedures Allowed As Second Case RateDocument31 pagesPhilHealth Circular No. 0035, s.2013 Annex 3 List of Medical Conditions and Procedures Allowed As Second Case RateChrysanthus Herrera0% (1)
- PhilHealth Circular No. 0035, s.2013 Annex 8 List of Medical Conditions Allowed For Referral PackageDocument7 pagesPhilHealth Circular No. 0035, s.2013 Annex 8 List of Medical Conditions Allowed For Referral PackageChrysanthus HerreraNo ratings yet
- PhilHealth Circular No. 0035, s.2013 Annex 7 List of Procedures With LateralityDocument11 pagesPhilHealth Circular No. 0035, s.2013 Annex 7 List of Procedures With LateralityChrysanthus HerreraNo ratings yet
- PhilHealth Circular No. 0035, s.2013 Annex 5 List of Medical Case Rates For Primary Care FacilitiesDocument22 pagesPhilHealth Circular No. 0035, s.2013 Annex 5 List of Medical Case Rates For Primary Care FacilitiesChrysanthus HerreraNo ratings yet
- PhilHealth Circular No. 0035, s.2013 Annex 11 PhilHealth Claim Form 3 Back Page (Revised November 2013)Document1 pagePhilHealth Circular No. 0035, s.2013 Annex 11 PhilHealth Claim Form 3 Back Page (Revised November 2013)Chrysanthus HerreraNo ratings yet
- PhilHealth ClaimForm1 GuidelinesDocument4 pagesPhilHealth ClaimForm1 GuidelinesAsh CampiaoNo ratings yet
- PhilHealth Circular No. 0035, s.2013 Annex11 - GuidelinesOnTheProperAccomplishmentOfClaimForm2 (November2013)Document8 pagesPhilHealth Circular No. 0035, s.2013 Annex11 - GuidelinesOnTheProperAccomplishmentOfClaimForm2 (November2013)Chrysanthus HerreraNo ratings yet
- Annex11 ImportantRemindersForThePhilHealthClaimForms (November2013)Document2 pagesAnnex11 ImportantRemindersForThePhilHealthClaimForms (November2013)Chrysanthus HerreraNo ratings yet
- PhilHealth Circular No. 0035, s.2013 Annex11 PhilHealthClaimForm3 Frontpage (RevisedNovember2013)Document2 pagesPhilHealth Circular No. 0035, s.2013 Annex11 PhilHealthClaimForm3 Frontpage (RevisedNovember2013)Chrysanthus HerreraNo ratings yet
- PhilHealth Circular No. 0035, s.2013 Annex11 - PhilHealthClaimForm2 (Revisednovember2013)Document2 pagesPhilHealth Circular No. 0035, s.2013 Annex11 - PhilHealthClaimForm2 (Revisednovember2013)Chrysanthus HerreraNo ratings yet
- Philippine Health Insurance Corporation Circular No. 0035, S. 2013 - Implementing Guidelines On The Medical and Procedure Case RatesDocument17 pagesPhilippine Health Insurance Corporation Circular No. 0035, S. 2013 - Implementing Guidelines On The Medical and Procedure Case RatesChrysanthus HerreraNo ratings yet
- Tabata WorkoutDocument1 pageTabata WorkoutEmily HeadingsNo ratings yet
- Job Contract Agreement Letter PDFDocument4 pagesJob Contract Agreement Letter PDFQazi Yusuf100% (1)
- Situation Analysis: Children in Bangsamoro Autonomous Region in Muslim MindanaoDocument335 pagesSituation Analysis: Children in Bangsamoro Autonomous Region in Muslim MindanaoTerence YuNo ratings yet
- Bethesda Thyroid 2017Document6 pagesBethesda Thyroid 2017Ladipo Temitope AyodejiNo ratings yet
- Blood ConversationDocument300 pagesBlood ConversationMohsin NabeelNo ratings yet
- Blue Green Yellow Modern English Intrapersonal Communication Educational Presentation - 20231109 - FixDocument12 pagesBlue Green Yellow Modern English Intrapersonal Communication Educational Presentation - 20231109 - FixmhailvandalzNo ratings yet
- Toxoplasmosis Serologic Testing AlgorithmDocument1 pageToxoplasmosis Serologic Testing AlgorithmHanny Prasetiana YuriantiNo ratings yet
- Hyaluronic Acid Embolism Treated With Subcutaneous High and Low Hyaluronidase Doses: Efficacy and Surrounding Tissue EffectDocument8 pagesHyaluronic Acid Embolism Treated With Subcutaneous High and Low Hyaluronidase Doses: Efficacy and Surrounding Tissue Effectkalinca marizyNo ratings yet
- Closure MineDocument14 pagesClosure MineAmilton filhoNo ratings yet
- Was King Tut Murdered?Document4 pagesWas King Tut Murdered?mauricio760No ratings yet
- BT RA 01 WeldingDocument6 pagesBT RA 01 Weldingnandha gopalNo ratings yet
- S.N o Name of Drug Recommended Paediatrics Dose Strength 1.: CPM - 2 mg/5mlDocument3 pagesS.N o Name of Drug Recommended Paediatrics Dose Strength 1.: CPM - 2 mg/5mlmrs raamNo ratings yet
- A Review On Water Used in Pharma Industry: European Journal of Pharmaceutical and Medical ResearchDocument11 pagesA Review On Water Used in Pharma Industry: European Journal of Pharmaceutical and Medical ResearchDinesh babuNo ratings yet
- Brubaker 2001Document5 pagesBrubaker 2001Residencia OftalmologíaNo ratings yet
- AntiConvulsants Drugs in Brief PDFDocument28 pagesAntiConvulsants Drugs in Brief PDFSunilNo ratings yet
- K4health-The Mhealth Planning Guide Key Considerations For Integrating Mobile Technology Into Health Programs-2015!04!06Document49 pagesK4health-The Mhealth Planning Guide Key Considerations For Integrating Mobile Technology Into Health Programs-2015!04!06DitaMaryaniNo ratings yet
- Medical Examiner'S Confidential ReportDocument2 pagesMedical Examiner'S Confidential ReportParesh BorboruahNo ratings yet
- Employee Benefits India PDFDocument2 pagesEmployee Benefits India PDFshahidki31100% (1)
- Logic ModelDocument2 pagesLogic ModelstojannaNo ratings yet
- Vawc Final ResearchDocument17 pagesVawc Final ResearchWilliam Vincent Soria100% (1)
- EMResource - NEDOCS Definitions and Tracking LogDocument2 pagesEMResource - NEDOCS Definitions and Tracking LogkingdonNo ratings yet
- Air PollutionDocument3 pagesAir PollutionGaurav Singh JantwalNo ratings yet
- Aspiracion Destornillador Implanto Roa-V1-Id1018Document3 pagesAspiracion Destornillador Implanto Roa-V1-Id1018CesarAmorotoNo ratings yet
- Alexander 2023 My Left KidneyDocument87 pagesAlexander 2023 My Left KidneyStamnumNo ratings yet
- 6 - Tamplate For Incident - Accident - Near Miss ReportDocument4 pages6 - Tamplate For Incident - Accident - Near Miss ReportImran razaNo ratings yet
- Nghe 4Document13 pagesNghe 4ToánNo ratings yet
- Jurnal Maternitas InggrisDocument20 pagesJurnal Maternitas InggrisTiffanie ClarkNo ratings yet
- Cancer - 2011 - Hajdu - A Note From History Landmarks in History of Cancer Part 2Document10 pagesCancer - 2011 - Hajdu - A Note From History Landmarks in History of Cancer Part 2Pilar AufrastoNo ratings yet
- Hun Yuan Qigong - All NotesDocument19 pagesHun Yuan Qigong - All Notespilillo50% (2)
- Human Condition Before Common EraDocument2 pagesHuman Condition Before Common EraACM23No ratings yet
- Swab Contact MethodDocument7 pagesSwab Contact Methodaca suki. haiNo ratings yet