You might also like
- Fixed Prosthodontics in Dental PracticeFrom EverandFixed Prosthodontics in Dental PracticeRating: 4 out of 5 stars4/5 (1)
- All - Ceramic Restorations: Composition of Ceramic Products Based On Feldspar, Kaolin and QuartzDocument9 pagesAll - Ceramic Restorations: Composition of Ceramic Products Based On Feldspar, Kaolin and QuartzVincent Ser100% (1)
- Guide Connector Design FPDsDocument41 pagesGuide Connector Design FPDsMrunal Doiphode83% (6)
- Classification of Failure of FPDDocument4 pagesClassification of Failure of FPDrayavarapu sunilNo ratings yet
- Occlusion in Complete DentureDocument64 pagesOcclusion in Complete Denturepuja singhNo ratings yet
- Attachments in Removable Pros Tho Don TicsDocument27 pagesAttachments in Removable Pros Tho Don TicsRajan Verma100% (4)
- Stresses Induced by Removoble Partial DentureDocument85 pagesStresses Induced by Removoble Partial DentureSimran Sahni100% (2)
- Indirect RetainersDocument52 pagesIndirect RetainerssarahNo ratings yet
- Ridge Preservation for Implant TreatmentDocument24 pagesRidge Preservation for Implant TreatmentFadly RasyidNo ratings yet
- Downs Analysis: SL Parameters Down's Mean Observed Values InferencesDocument9 pagesDowns Analysis: SL Parameters Down's Mean Observed Values Inferencesmebibeg50% (4)
- Principles of Tooth PreparationDocument43 pagesPrinciples of Tooth PreparationJyoti Raheja100% (3)
- Treatment Planning Single Maxillary Anterior Implants for DentistsFrom EverandTreatment Planning Single Maxillary Anterior Implants for DentistsNo ratings yet
- Clinical Cases in Restorative and Reconstructive DentistryFrom EverandClinical Cases in Restorative and Reconstructive DentistryRating: 5 out of 5 stars5/5 (1)
- Evaluation Abutment Tooth:: Prof. Adel Farhan IbraheemDocument12 pagesEvaluation Abutment Tooth:: Prof. Adel Farhan IbraheemMohammad ANo ratings yet
- RPD Diagnosis, TX PlanningDocument10 pagesRPD Diagnosis, TX Planningapi-3710948No ratings yet
- Rest and Rest Seats: An OverviewDocument20 pagesRest and Rest Seats: An OverviewCharmiNo ratings yet
- Alloys For FPDDocument101 pagesAlloys For FPDsapnaNo ratings yet
- The Cantilever Fixed Partial Denture-A Literature ReviewDocument20 pagesThe Cantilever Fixed Partial Denture-A Literature ReviewJittin JamesNo ratings yet
- OVERDENTURESDocument15 pagesOVERDENTURESAditya SavirmathNo ratings yet
- Swing Lock Partial DentureDocument22 pagesSwing Lock Partial DentureSanNo ratings yet
- Philosophies of RPD DesigningDocument8 pagesPhilosophies of RPD DesigningThenmozhiNo ratings yet
- Connector Design PrinciplesDocument24 pagesConnector Design PrinciplesVikas Aggarwal100% (1)
- Precision Attachments Applications and LimitationsDocument9 pagesPrecision Attachments Applications and LimitationsVivek ShankarNo ratings yet
- Selection of Teeth and Esthetics in Complete DentureDocument49 pagesSelection of Teeth and Esthetics in Complete DentureSawsan Z. Jwaied100% (1)
- Prostho Lec - OverdenturesDocument14 pagesProstho Lec - Overdenturesdrgayen6042No ratings yet
- Fixed ProsthodonticsDocument5 pagesFixed ProsthodonticsSnehal UpadhyayNo ratings yet
- 1 FP2 FPD Lecture 2011pdfDocument15 pages1 FP2 FPD Lecture 2011pdfIndrani DasNo ratings yet
- Removable Partial Denture ComponentsDocument128 pagesRemovable Partial Denture ComponentsVikas Aggarwal50% (2)
- Partial Retainer in FPD DR VikasDocument99 pagesPartial Retainer in FPD DR VikasVikas AggarwalNo ratings yet
- Provisionals in Dentistry - From Past To Recent Advances: Rohitraghavan, Shajahan P A, NeenakunjumonDocument6 pagesProvisionals in Dentistry - From Past To Recent Advances: Rohitraghavan, Shajahan P A, Neenakunjumonnavdeep100% (1)
- Esthetic in Complete DentureDocument14 pagesEsthetic in Complete DentureNidhi KatochNo ratings yet
- Fabrication of Record BaseDocument38 pagesFabrication of Record BaseSuvasish SuvasishNo ratings yet
- Finish Line of The Preparation Is The End of Tooth PreparationDocument36 pagesFinish Line of The Preparation Is The End of Tooth PreparationAnureet MehrokNo ratings yet
- Clinical Failures in FPDDocument57 pagesClinical Failures in FPDdrreba100% (3)
- Orientation Jaw Relation ProsthoDocument24 pagesOrientation Jaw Relation ProsthoFourthMolar.comNo ratings yet
- Overdenture Presentation PDFDocument19 pagesOverdenture Presentation PDFAjay Mehta100% (1)
- Complete Denture Guide - Functions, Parts, Fabrication StepsDocument19 pagesComplete Denture Guide - Functions, Parts, Fabrication StepsSajeeb HossainNo ratings yet
- Major Connector in RDPDocument73 pagesMajor Connector in RDPmujtabaNo ratings yet
- Principles of Designing RPD Copy Copy 160211154113Document38 pagesPrinciples of Designing RPD Copy Copy 160211154113Abdelreheem ElgendyNo ratings yet
- Finish LinesDocument17 pagesFinish LinesWaseem AhmedNo ratings yet
- Retainers in FPDDocument32 pagesRetainers in FPDPriyanthi A50% (2)
- Gingivally Approaching Clasp - PedagogyDocument35 pagesGingivally Approaching Clasp - PedagogyNiaz AhammedNo ratings yet
- Die Materials, Investment and Inlay WaxDocument167 pagesDie Materials, Investment and Inlay WaxBhargav KambhampatiNo ratings yet
- Effects of Aging Edentulous PatientDocument29 pagesEffects of Aging Edentulous PatientMaliha TahirNo ratings yet
- Retention in Maxillofacial Prosthesis: A Literature ReviewDocument9 pagesRetention in Maxillofacial Prosthesis: A Literature ReviewIJAR JOURNALNo ratings yet
- Radiographs in Prosthodontics / Orthodontic Courses by Indian Dental AcademyDocument38 pagesRadiographs in Prosthodontics / Orthodontic Courses by Indian Dental Academyindian dental academy100% (4)
- Journal Club 5Document74 pagesJournal Club 5Naveen Kumar100% (1)
- Dr. Omkar Shetty - ProsthoDocument7 pagesDr. Omkar Shetty - ProsthoSyed NooraniNo ratings yet
- Mandibular MovementsDocument110 pagesMandibular MovementsNeha Aggarwal100% (1)
- Laser Applications in ProsthodonticsDocument42 pagesLaser Applications in Prosthodonticsvarsha ammuNo ratings yet
- Relining & RebasingDocument86 pagesRelining & RebasingJASPREETKAUR0410100% (1)
- Checking and Verification of Crowns and Fixed ProsthesesDocument5 pagesChecking and Verification of Crowns and Fixed Prostheseskhaled alahmadNo ratings yet
- Library Dissertation On Nanotechnology in Prosthodontics: Sumayya.A. Nazar Junior Resident Department of ProsthodonticsDocument69 pagesLibrary Dissertation On Nanotechnology in Prosthodontics: Sumayya.A. Nazar Junior Resident Department of ProsthodonticsDr FarhatNo ratings yet
- Partial Coverage PPT FinalDocument83 pagesPartial Coverage PPT FinalTotta Ayman50% (2)
- Prosthodontic Care For Patients With Cleft PalateDocument6 pagesProsthodontic Care For Patients With Cleft PalateShraddha AgarwalNo ratings yet
- Occlusion in Fpd-13.08.10Document104 pagesOcclusion in Fpd-13.08.10Paridhi GargNo ratings yet
- Border Molding in Complete DentureDocument40 pagesBorder Molding in Complete DentureVishnu S Pattath0% (1)
- Retainer in Fixed Partial Denture'S: 1 Presented by - Dr. Amit Bhargav Post Graduate 3 Year Deptt. of ProsthodonticsDocument29 pagesRetainer in Fixed Partial Denture'S: 1 Presented by - Dr. Amit Bhargav Post Graduate 3 Year Deptt. of ProsthodonticsAmit BhargavNo ratings yet
- Color & Shade Matching PPT - UnlockedDocument70 pagesColor & Shade Matching PPT - UnlockedAmit Bhargav100% (1)
- Tilted Post Teeh II Biomech TherapyDocument7 pagesTilted Post Teeh II Biomech TherapyAmit BhargavNo ratings yet
- Biomaterials For Dental ImplantsDocument136 pagesBiomaterials For Dental ImplantsAmit Bhargav100% (1)
- OverdentureDocument97 pagesOverdentureAmit Bhargav100% (1)
- The Effect of Surface Treatment On Fiber ReinforcedDocument28 pagesThe Effect of Surface Treatment On Fiber ReinforcedAmit BhargavNo ratings yet
- Posterior Palatal Seal ProsthoDocument64 pagesPosterior Palatal Seal ProsthoAmit BhargavNo ratings yet
- Posterior Palatal SealDocument74 pagesPosterior Palatal SealAmit Bhargav50% (2)
- Complete Denture Prosthodontics in Children With Ectodermal DysplasiaDocument29 pagesComplete Denture Prosthodontics in Children With Ectodermal DysplasiaAmit BhargavNo ratings yet
- Hollow DenturesDocument31 pagesHollow DenturesAmit BhargavNo ratings yet
- Comparative Anatomy of Bone, Brain, Skull, Muskuloskeletal System, Gait and PostureDocument62 pagesComparative Anatomy of Bone, Brain, Skull, Muskuloskeletal System, Gait and PostureAmit BhargavNo ratings yet
- Cranial Nerves (7 12)Document87 pagesCranial Nerves (7 12)Amit BhargavNo ratings yet
- Anatomy of Head and Neck Nerve Supply and Lymphatic DrainageDocument168 pagesAnatomy of Head and Neck Nerve Supply and Lymphatic DrainageAmit Bhargav100% (3)
- Prosthodontics: Dental Assistant Diploma ProgramDocument33 pagesProsthodontics: Dental Assistant Diploma ProgrambeyNo ratings yet
- Maxillary First PremolarDocument6 pagesMaxillary First PremolarHayley Welsh100% (1)
- Efficacy of Transpalatal Arch As An Anchorage Rein PDFDocument7 pagesEfficacy of Transpalatal Arch As An Anchorage Rein PDFOana CostanNo ratings yet
- Maxillary Expansion in The Mixed Dentition: Rapid or Semi-Rapid?Document8 pagesMaxillary Expansion in The Mixed Dentition: Rapid or Semi-Rapid?Shriya MurarkaNo ratings yet
- 12trauma de Oclusion PDFDocument6 pages12trauma de Oclusion PDFManuel Tovar ZevallosNo ratings yet
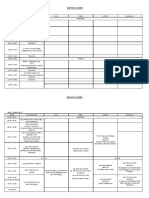
- Jadwal AcaraDocument2 pagesJadwal AcaraElok Faiqotul UmmaNo ratings yet
- Sajb 33263 266Document4 pagesSajb 33263 266Ezza RiezaNo ratings yet
- Clasificacion de Angle Se Usa Realmente - Morton, Katz PDFDocument7 pagesClasificacion de Angle Se Usa Realmente - Morton, Katz PDFLisset MaritzaNo ratings yet
- Manipulation of AmalgamDocument5 pagesManipulation of AmalgamELAINE DE OCAMPONo ratings yet
- Giuseppe Marchetti Deep Margin Elevation Indirect and Direct Composite Restorations A Clinical Case ViaDocument24 pagesGiuseppe Marchetti Deep Margin Elevation Indirect and Direct Composite Restorations A Clinical Case Viajuan luis100% (1)
- CEE Restorative Focus Catalog 2018 Complete PDFDocument36 pagesCEE Restorative Focus Catalog 2018 Complete PDFudirmusaNo ratings yet
- Rehabilitation of A Patient With An Immediate Complete Denture: A Case ReportDocument4 pagesRehabilitation of A Patient With An Immediate Complete Denture: A Case ReportghinaNo ratings yet
- Coahman Galip Gurel Et Al 2012Document12 pagesCoahman Galip Gurel Et Al 2012Jorge RojasNo ratings yet
- Development of OcclusionDocument49 pagesDevelopment of OcclusionSardarni Ramandeep KaurNo ratings yet
- Fixed ProsthodonticsDocument16 pagesFixed ProsthodonticsMagnet ShotNo ratings yet
- Anchorage in OrthodonticsDocument127 pagesAnchorage in Orthodonticsmustafa_tambawala75% (4)
- Download Atlas Of Oral Histology 2Nd Edition Harikrishnan Prasad full chapterDocument67 pagesDownload Atlas Of Oral Histology 2Nd Edition Harikrishnan Prasad full chaptervicki.jackson553100% (5)
- Chapter 48Document40 pagesChapter 48serhunaNo ratings yet
- Iotn Ruler Made EasyDocument7 pagesIotn Ruler Made EasyZahid Ahmad100% (1)
- AE Instrumentenkunde 2022 GBDocument23 pagesAE Instrumentenkunde 2022 GBGeorgi GugicevNo ratings yet
- Essentials of Dentistry Quick Review and PDFDocument327 pagesEssentials of Dentistry Quick Review and PDFIonela Madalina100% (1)
- Gummy Smile017Document55 pagesGummy Smile017Shathra'a HamzaNo ratings yet
- Case Report: Management of Dental Trauma in ChildrenDocument5 pagesCase Report: Management of Dental Trauma in ChildrenIfadahNo ratings yet
- Guidelines For Placing Attachments: Your ChoiceDocument2 pagesGuidelines For Placing Attachments: Your ChoiceMark Saul Pérez TorresNo ratings yet
- Growth RotationDocument19 pagesGrowth RotationSyed Bazli AlwiNo ratings yet
- Andrew 1994Document15 pagesAndrew 1994Néia CostaNo ratings yet
- Journal ClubDocument25 pagesJournal ClubAnonymous Val05Blj100% (1)
- Pulp TherapyDocument42 pagesPulp TherapyruchikaNo ratings yet