You might also like
- NCLFNP - Mr. Robert McClelland CaseDocument4 pagesNCLFNP - Mr. Robert McClelland CaseAiresh Lamao50% (2)
- Orif Case StudyDocument17 pagesOrif Case Studykreny1078% (9)
- SP CSDocument4 pagesSP CSKhan HansNo ratings yet
- Laryngeal Obstruction: Narciso A. CañibanDocument54 pagesLaryngeal Obstruction: Narciso A. Cañibanalexandrajane200767% (3)
- Blood TransfusionDocument63 pagesBlood TransfusionMary Joy F. Ching100% (3)
- Curative and Rehabilitative Nursing Care Management of Clients in Acute Biologic CrisisDocument44 pagesCurative and Rehabilitative Nursing Care Management of Clients in Acute Biologic CrisisArgee AlonsabeNo ratings yet
- Transfusion ReactionsDocument11 pagesTransfusion ReactionsBungas Arisudana50% (2)
- 300+ TOP Digestive System MCQs and Answers PDF Quiz ExamDocument11 pages300+ TOP Digestive System MCQs and Answers PDF Quiz ExamMuhammad AliNo ratings yet
- Rationale: This Will Assess Pain LevelDocument7 pagesRationale: This Will Assess Pain LevelCoreyNo ratings yet
- Oxygen Terapi Dan PrinsipelDocument16 pagesOxygen Terapi Dan PrinsipelAmrita KaurNo ratings yet
- Nursing Care PlanDocument20 pagesNursing Care PlanZamranosNo ratings yet
- NCP Fever 1Document11 pagesNCP Fever 1Deepak VermaNo ratings yet
- Drug Presentation On AminophyllineDocument10 pagesDrug Presentation On Aminophyllineelisha immanuelNo ratings yet
- Osteomalacia Care Plan/OthersDocument11 pagesOsteomalacia Care Plan/OthersJill Jackson, RNNo ratings yet
- Effectiveness of Planned Teaching Programme On Knowledge Regarding Needle Stick Injury Among The Staff NursesDocument3 pagesEffectiveness of Planned Teaching Programme On Knowledge Regarding Needle Stick Injury Among The Staff NursesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Spina Bifida NCPDocument3 pagesSpina Bifida NCPShahzad GulfamNo ratings yet
- PP Insect Bite 2007 (Print)Document16 pagesPP Insect Bite 2007 (Print)Ali RumiNo ratings yet
- Health-Perception-Health-Management PatternDocument3 pagesHealth-Perception-Health-Management PatternBela MillenaNo ratings yet
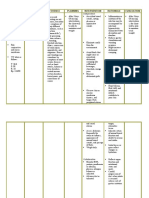
- Assesment Diagnosis Planning Intervention Rationale EvaluationDocument3 pagesAssesment Diagnosis Planning Intervention Rationale EvaluationTrisha Suazo100% (1)
- CholecystitisDocument1 pageCholecystitisDianne ParungaoNo ratings yet
- NCP For ConcussionDocument3 pagesNCP For Concussiontamtam_antonio100% (1)
- SIGNIFICANT SAQsDocument407 pagesSIGNIFICANT SAQsFarid Iqbal100% (2)
- FractureDocument1 pageFractureReechie TeasoonNo ratings yet
- CP Intestinal Obstruction Nursing Care PlanDocument7 pagesCP Intestinal Obstruction Nursing Care PlanShiella Heart MalanaNo ratings yet
- Hypertension Nursing Care PlanDocument2 pagesHypertension Nursing Care PlanCj LowryNo ratings yet
- Diphtheria SlideDocument11 pagesDiphtheria Slideandre andreNo ratings yet
- Discharge Plan Post SeizureDocument2 pagesDischarge Plan Post SeizureVecky TolentinoNo ratings yet
- LARYNGITISDocument13 pagesLARYNGITIStherese BNo ratings yet
- Lesson Plan On HyperlipidemiaDocument4 pagesLesson Plan On HyperlipidemiaBinita Shakya100% (1)
- Nicu Lesson PlanDocument11 pagesNicu Lesson PlanSAYMABANUNo ratings yet
- Nursing Care Plan: Assessment Diagnosis Inference Planning Intervention Rationale EvaluationDocument3 pagesNursing Care Plan: Assessment Diagnosis Inference Planning Intervention Rationale EvaluationAbdallah AlasalNo ratings yet
- Nursing Care PlanDocument4 pagesNursing Care PlanJobelyn TunayNo ratings yet
- Total Abdominal Hysterectomy Actual NCPDocument1 pageTotal Abdominal Hysterectomy Actual NCPDoreen ClaireNo ratings yet
- Drug Study - LevothyroxineDocument1 pageDrug Study - LevothyroxineCarla Tongson MaravillaNo ratings yet
- Cholecystectomy Nursing Care Plan: Risk For InfectionDocument1 pageCholecystectomy Nursing Care Plan: Risk For InfectionBesael BaccolNo ratings yet
- Nursing Care Plan: Change in Health Status As Evidence by Excessive Shaking After 1hour, The Patient Will Be Able ToDocument1 pageNursing Care Plan: Change in Health Status As Evidence by Excessive Shaking After 1hour, The Patient Will Be Able ToVoid LessNo ratings yet
- Artillo NCP Renal Cell CarcinomaDocument5 pagesArtillo NCP Renal Cell CarcinomaAl TheóNo ratings yet
- Word Ncp.......... TetanusDocument6 pagesWord Ncp.......... TetanusaianrNo ratings yet
- Assessment Diagnosis Planning Nursing Intervention Rationale EvaluationDocument2 pagesAssessment Diagnosis Planning Nursing Intervention Rationale Evaluationjennelyn losantaNo ratings yet
- Assessment Nursing Diagnosis Planning Interventions EvaluationsDocument4 pagesAssessment Nursing Diagnosis Planning Interventions EvaluationsAjay SupanNo ratings yet
- NCP Proper - Obstructive JaundiceDocument8 pagesNCP Proper - Obstructive JaundiceWyen Cabatbat100% (2)
- NCP Alcoholic NeuropathyDocument5 pagesNCP Alcoholic NeuropathyPeachy Marie Anca100% (1)
- Assessment Diagnosis Planning Intrvention Rationale EvaluationDocument1 pageAssessment Diagnosis Planning Intrvention Rationale EvaluationMar OrdanzaNo ratings yet
- PCNL Nursing Care Plan 2Document11 pagesPCNL Nursing Care Plan 2ISICLE GTNo ratings yet
- Terminology CHNDocument4 pagesTerminology CHNKailash NagarNo ratings yet
- Patient With Neutropenia Risk For Infection Related To Inadequate Secondary Defenses (Leukopenia, Neutropenia), Altered Response To MicrobialDocument2 pagesPatient With Neutropenia Risk For Infection Related To Inadequate Secondary Defenses (Leukopenia, Neutropenia), Altered Response To MicrobialICa MarlinaNo ratings yet
- NCP - Pediatrics Case Study (Pnuemonia With Down Syndrome)Document4 pagesNCP - Pediatrics Case Study (Pnuemonia With Down Syndrome)Charley DegamoNo ratings yet
- Fistula NCPDocument1 pageFistula NCPHasna LisnaNo ratings yet
- Care of The Client With Pulmonary Tuberculosis Utilizing Orem's TheoryDocument13 pagesCare of The Client With Pulmonary Tuberculosis Utilizing Orem's TheoryRazel Kinette AzotesNo ratings yet
- NCP SeratroDocument2 pagesNCP SeratroKristine YoungNo ratings yet
- Schizophrenia Nursing ManagementDocument56 pagesSchizophrenia Nursing ManagementHumphreyNo ratings yet
- Actual NCPDocument2 pagesActual NCPbaki0146No ratings yet
- Case Presentation On Parkinsonism 4th YearDocument27 pagesCase Presentation On Parkinsonism 4th YearArchanaNo ratings yet
- Femur Fracture Health EducationDocument1 pageFemur Fracture Health EducationMadx VNo ratings yet
- Case Study On Left PCOM AneurysmDocument32 pagesCase Study On Left PCOM AneurysmGopal AcharyaNo ratings yet
- Recreational TherapyDocument22 pagesRecreational TherapyKishore RathoreNo ratings yet
- Dengue-WPS OfficeDocument20 pagesDengue-WPS OfficeAnnamalai MNo ratings yet
- NCP - PoliomyelitisDocument4 pagesNCP - PoliomyelitisCassey CuregNo ratings yet
- Case Report On Bipolar Affective Disorder: Mania With Psychotic SymptomsDocument2 pagesCase Report On Bipolar Affective Disorder: Mania With Psychotic SymptomskslhfwoiebvNo ratings yet
- Management of Tuberculosis: A guide for clinicians (eBook edition)From EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)No ratings yet
- Impaired SwallowingDocument2 pagesImpaired SwallowingfaizaNo ratings yet
- Nursing Care Plan Assessment Diagnosis Inference Planning Interventio N Rationale Evaluatio N SubjectiveDocument58 pagesNursing Care Plan Assessment Diagnosis Inference Planning Interventio N Rationale Evaluatio N SubjectiveJemina Rafanan RacadioNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale Evaluation Subjective Data: Short-Term Goal: Independent IndependentDocument3 pagesAssessment Diagnosis Planning Intervention Rationale Evaluation Subjective Data: Short-Term Goal: Independent IndependentWonie booNo ratings yet
- DiarrheaDocument3 pagesDiarrheaBert GasalNo ratings yet
- Subjective Short Term Independent: Patient Is Conscious and CooperativeDocument5 pagesSubjective Short Term Independent: Patient Is Conscious and Cooperativeraven riveraNo ratings yet
- Pda Case StudyDocument27 pagesPda Case Studykreny10100% (9)
- Delayed Growth and Development Assessment N.Diagnosis Inference Planning Intervention Rationale EvaluationDocument2 pagesDelayed Growth and Development Assessment N.Diagnosis Inference Planning Intervention Rationale Evaluationkreny10No ratings yet
- Drug StudyDocument5 pagesDrug Studykreny10No ratings yet
- Source: Operating Room Technique by Nancymarie PhillipsDocument1 pageSource: Operating Room Technique by Nancymarie Phillipsnoreen ellieNo ratings yet
- CATest PDFDocument1 pageCATest PDFAsrie Sukawatie PutrieNo ratings yet
- Definition and ClassificationDocument36 pagesDefinition and Classificationplogiojayr8340No ratings yet
- Environmental Emergencies Heat Exhaustion HeatstrokeDocument6 pagesEnvironmental Emergencies Heat Exhaustion HeatstrokepauchanmnlNo ratings yet
- Final Guidelines For Leishmaniasis - Print VersionDocument88 pagesFinal Guidelines For Leishmaniasis - Print VersiongaasheNo ratings yet
- Epidemiology, Clinical Presentation, and Diagnostic Evaluation of Parapneumonic Effusion and Empyema in Adults - UpToDateDocument40 pagesEpidemiology, Clinical Presentation, and Diagnostic Evaluation of Parapneumonic Effusion and Empyema in Adults - UpToDateAlejandra LopezNo ratings yet
- Wesleyan: College of Nursing and Allied Medical SciencesDocument2 pagesWesleyan: College of Nursing and Allied Medical SciencesShane Aileen AngelesNo ratings yet
- Complement C3Document8 pagesComplement C3Akbar RihansyahNo ratings yet
- 15 Causes of Burning in The FeetDocument6 pages15 Causes of Burning in The Feetfausto omioNo ratings yet
- Ap Psychology Unit 8 Overview 2015Document5 pagesAp Psychology Unit 8 Overview 2015api-262090199No ratings yet
- LSM RepairDocument4 pagesLSM RepairDanily Faith VillarNo ratings yet
- Nursing Responsibilities For Oxygen AdministrationDocument3 pagesNursing Responsibilities For Oxygen AdministrationJahseh WolfeNo ratings yet
- Ontario Fee CodesDocument4 pagesOntario Fee CodesCraig RaflaNo ratings yet
- Community Medicine Notes & Question Bank: MBBS para ClinicalDocument67 pagesCommunity Medicine Notes & Question Bank: MBBS para ClinicalAnish Nazar100% (2)
- PsychiatryDocument100 pagesPsychiatryDikshant DaswatNo ratings yet
- Gout and Hyperuricemia: PathophysiologyDocument1 pageGout and Hyperuricemia: Pathophysiologyسمرة طايبNo ratings yet
- F 360Document6 pagesF 360اسعد عبد الحميد50% (2)
- 3-3 Infections Main PoignetDocument52 pages3-3 Infections Main PoignetProfesseur Christian Dumontier100% (5)
- A Short History of OnchocerciasisDocument12 pagesA Short History of OnchocerciasisAldo Sánchez100% (1)
- Harish Kumar Adwani ReportsDocument3 pagesHarish Kumar Adwani ReportspriyushhospitallabNo ratings yet
- Objective Testing of Pelvic Floor FunctionDocument2 pagesObjective Testing of Pelvic Floor FunctionSteven ElvyNo ratings yet
- Physiotherapy and Occupational Therapy in Patients With StrokeDocument8 pagesPhysiotherapy and Occupational Therapy in Patients With Strokeilona ilincaNo ratings yet
- Covid-19 Mitigation PlanDocument8 pagesCovid-19 Mitigation PlanEkum EdunghuNo ratings yet
- Guilford Child & Adolescent Psychology Chapter SamplerDocument97 pagesGuilford Child & Adolescent Psychology Chapter SamplerAdelaKočanBahtoNo ratings yet
- Health in Your HandDocument6 pagesHealth in Your HandBhargav Mistry100% (2)
- DR - PARTHA - 2018 Clinical Microbiology II PDFDocument88 pagesDR - PARTHA - 2018 Clinical Microbiology II PDFNuzki YofandaNo ratings yet