You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- National ALS Instructor ManualDocument38 pagesNational ALS Instructor ManualRIDZWAN ABDUL RAZAKNo ratings yet
- REST Booklet 2012 PDFDocument258 pagesREST Booklet 2012 PDFiahtesham100% (4)
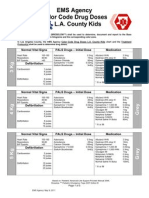
- EMS Agency Color Code Drug Doses L. L.A. County Kids: Normal Vital Signs PALS Drugs - Initial Dose MedicationDocument5 pagesEMS Agency Color Code Drug Doses L. L.A. County Kids: Normal Vital Signs PALS Drugs - Initial Dose MedicationCruz VerdeNo ratings yet
- RJPDocument38 pagesRJPjoyfullNo ratings yet
- Opito Medical Emergency Response Requirements Valid From 432016Document20 pagesOpito Medical Emergency Response Requirements Valid From 432016Joseph Soebroto100% (1)
- Advanced Life Support EMS ScenariosDocument147 pagesAdvanced Life Support EMS Scenariosfidelurtecho4881No ratings yet
- Word ERC Section 3. S0300-9572 (15) 00328-7 - MainDocument48 pagesWord ERC Section 3. S0300-9572 (15) 00328-7 - MainImam Hakim SuryonoNo ratings yet
- CV of Mark ErasmusDocument6 pagesCV of Mark Erasmusmarkyboy75No ratings yet
- Lifepak 20e: Defibrillator/MonitorDocument12 pagesLifepak 20e: Defibrillator/MonitorGabriel MudlongNo ratings yet
- A Geographic Information System Simulation Model of EMS: Reducing Ambulance Response TimeDocument7 pagesA Geographic Information System Simulation Model of EMS: Reducing Ambulance Response TimeCharmaine ColetaNo ratings yet
- Test 1 EMTDocument28 pagesTest 1 EMTCourtney McBrideNo ratings yet
- 2009 Laerdal CatalogDocument176 pages2009 Laerdal CatalogEnerspect Medical Solutions100% (2)
- Advanced Life Support Algorithm: Learning OutcomesDocument8 pagesAdvanced Life Support Algorithm: Learning OutcomesParvathy R NairNo ratings yet
- Als Protocol Dec 2023 FinalDocument84 pagesAls Protocol Dec 2023 FinalRobert MccallumNo ratings yet
- Ebook KoasDocument4 pagesEbook KoasGusti Ari SetyawanNo ratings yet
- FDNY Strategic Plan 2009 2010 FinalDocument29 pagesFDNY Strategic Plan 2009 2010 Finalبيدرو اسبينوزا مات بيدروNo ratings yet
- 7mosby's EMT-Basic Textbook - Revised Reprint, 2nd EditionDocument22 pages7mosby's EMT-Basic Textbook - Revised Reprint, 2nd EditionKathrina AlfonsoNo ratings yet
- ALS Recertification CourseDocument64 pagesALS Recertification CoursePanagiotis Iliopoulos100% (1)
- Warren More Emergency Medical Services Personnel and Increased Survival After OHCADocument9 pagesWarren More Emergency Medical Services Personnel and Increased Survival After OHCAJamison ParfittNo ratings yet
- Crew Size Simulation Cardiac Arrest TapiaiDocument12 pagesCrew Size Simulation Cardiac Arrest TapiaiJamison ParfittNo ratings yet
- Advanced Life Support Training Manual Final 2017Document87 pagesAdvanced Life Support Training Manual Final 2017Azhar MohamedNo ratings yet
- A Systematic Approach To EMS Cardiac Arrest Management Improves Survival For Out of Hospital Cardiac ArrestDocument29 pagesA Systematic Approach To EMS Cardiac Arrest Management Improves Survival For Out of Hospital Cardiac ArrestMELLYNDA ANASTASYANo ratings yet
- Advanced Life Support Training and Assessment PDFDocument6 pagesAdvanced Life Support Training and Assessment PDFwilmaNo ratings yet
- Pediatric Cardiac Arrest AlgorithmDocument27 pagesPediatric Cardiac Arrest AlgorithmLinna AndrianiNo ratings yet
- Pediatric Medical Emergencies Rev Oct 2016Document27 pagesPediatric Medical Emergencies Rev Oct 2016ElvisNo ratings yet
- Als Protocol Hpcsa PDFDocument21 pagesAls Protocol Hpcsa PDFPrince MojakiNo ratings yet
- Resuscitation Training 2016 - KKMDocument60 pagesResuscitation Training 2016 - KKMSiti NabilaNo ratings yet
- Resuscitation Highlights in 2018Document8 pagesResuscitation Highlights in 2018hermesNo ratings yet
- RJP Aha 2020Document29 pagesRJP Aha 2020byeukid_224862614No ratings yet
- Part 1 - Clinical Manual - January 2018 - Version 8.0Document260 pagesPart 1 - Clinical Manual - January 2018 - Version 8.0AbhishekNo ratings yet