You might also like
- Ebstein Anomaly, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandEbstein Anomaly, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Management of Tuberculosis: A guide for clinicians (eBook edition)From EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)No ratings yet
- Causes and Management of Syncope in DentistryDocument27 pagesCauses and Management of Syncope in DentistrySelvarathi KandhaswamyNo ratings yet
- ShockDocument64 pagesShockAnusha VergheseNo ratings yet
- Periodontitis As A Risk Factor For Systemic DiseaseDocument13 pagesPeriodontitis As A Risk Factor For Systemic DiseaseRussia Al ShboulNo ratings yet
- Thyroglossal CystsDocument4 pagesThyroglossal CystsCondurache Ilie-AndreiNo ratings yet
- Disorder of Oral CavityDocument4 pagesDisorder of Oral CavitySiva0726No ratings yet
- Bleeding Disorders FinalDocument35 pagesBleeding Disorders FinalsanthiyasandyNo ratings yet
- Epidemiology of Non-Communicable DiseasesDocument16 pagesEpidemiology of Non-Communicable DiseasesAparna AbyNo ratings yet
- Hemophilia Guide: Causes, Symptoms, TreatmentsDocument3 pagesHemophilia Guide: Causes, Symptoms, TreatmentsMuthoni NdongaNo ratings yet
- Nephrotic Syndrome: Ron Christian Neil T. Rodriguez, MD 1 Year Pedia ResidentDocument26 pagesNephrotic Syndrome: Ron Christian Neil T. Rodriguez, MD 1 Year Pedia ResidentRon Christian Neil RodriguezNo ratings yet
- Management of Hypoxia During AnaesthesiaDocument5 pagesManagement of Hypoxia During AnaesthesiaNurhafizahImfista100% (1)
- Haemophilia: DR Y S Vishnu Vardhan, PGDocument64 pagesHaemophilia: DR Y S Vishnu Vardhan, PGVishnu VardhanNo ratings yet
- Gingival Crevicular Fluid Composition and Clinical SignificanceDocument57 pagesGingival Crevicular Fluid Composition and Clinical SignificanceRiya KvNo ratings yet
- Hodgkins Lymphoma: DR Swathi R KrishnaDocument83 pagesHodgkins Lymphoma: DR Swathi R KrishnaSwathi R KrishnaNo ratings yet
- Approach To Septic ShockDocument16 pagesApproach To Septic ShockRaja EllysyaNo ratings yet
- Anatomy and Physiology of the Coronary CirculationDocument60 pagesAnatomy and Physiology of the Coronary CirculationNithya SekarNo ratings yet
- Holy Family College of Nursing Seminar On Tele-MedicineDocument22 pagesHoly Family College of Nursing Seminar On Tele-MedicineTanviNo ratings yet
- Seminar On Shock: IntroductionDocument22 pagesSeminar On Shock: Introductionmahendra singhNo ratings yet
- SyncopeDocument4 pagesSyncopeLakshay Chanana100% (1)
- Diseases of The Temporomandibular JointDocument27 pagesDiseases of The Temporomandibular JointJustDen090% (1)
- BSC Nursing: Medical Surgical Nursing Unit V - Disorders of The Cardio Vascular SystemDocument34 pagesBSC Nursing: Medical Surgical Nursing Unit V - Disorders of The Cardio Vascular SystemPoova Ragavan100% (1)
- SyncopeDocument25 pagesSyncopeRianiEffendiNo ratings yet
- Hyphema 2Document7 pagesHyphema 2heidyNo ratings yet
- Glomerulonephritis: Nameesha Natasha Naidu 20130105Document26 pagesGlomerulonephritis: Nameesha Natasha Naidu 20130105AliMalikNo ratings yet
- Malabsorption Syndrome: Dr. Gehan Mohamed Dr. Abdelaty ShawkyDocument25 pagesMalabsorption Syndrome: Dr. Gehan Mohamed Dr. Abdelaty ShawkyNikhil GuptaNo ratings yet
- Spleenomegaly & Hypersplenism Etiology Pathogenesis and Surgical ManagementDocument53 pagesSpleenomegaly & Hypersplenism Etiology Pathogenesis and Surgical ManagementMuhammad SaadNo ratings yet
- Cushing's SyndromeDocument68 pagesCushing's SyndromeKaye De Guzman, BSN - Level 3ANo ratings yet
- Pemphigus vulgarisPPTDocument23 pagesPemphigus vulgarisPPTSiti HanisaNo ratings yet
- Oral Complications of Cancer TreatmentDocument68 pagesOral Complications of Cancer TreatmentFarisha RasheedNo ratings yet
- Lichen Planus Guide: Causes, Symptoms and TreatmentDocument37 pagesLichen Planus Guide: Causes, Symptoms and TreatmentSaroash SadruddinNo ratings yet
- Antibiotic in OmfsDocument47 pagesAntibiotic in OmfsRajat GuptaNo ratings yet
- Morphologic Patterns of Acute InflammationDocument51 pagesMorphologic Patterns of Acute Inflammationحفصه حسينNo ratings yet
- ErythroplakiaDocument20 pagesErythroplakiaEshan VermaNo ratings yet
- Lip Cancer-Ablative and Reconstructive Surgery: ChapDocument52 pagesLip Cancer-Ablative and Reconstructive Surgery: ChapYang Lin Chen100% (1)
- Cranial Nerves Examination GuideDocument14 pagesCranial Nerves Examination GuideMoussa FarhatNo ratings yet
- Vitamin A and XerophthalmiaDocument29 pagesVitamin A and XerophthalmiaJayashree IyerNo ratings yet
- Management of Lymphomas: 2018 Indian Expert ConsensusDocument24 pagesManagement of Lymphomas: 2018 Indian Expert ConsensusAndi SusiloNo ratings yet
- Connective Tissue LesionsDocument285 pagesConnective Tissue LesionsRwskhans KhanNo ratings yet
- Cardiac Invasive Diagnostic Tests GuideDocument19 pagesCardiac Invasive Diagnostic Tests GuideSimran JosanNo ratings yet
- Cell Injury PathologyDocument40 pagesCell Injury Pathologysridhar100% (1)
- Systemic Lupus Erythematosus (SLE)Document39 pagesSystemic Lupus Erythematosus (SLE)Nadya SabrinaNo ratings yet
- SurgeryDocument12 pagesSurgeryManusheeNo ratings yet
- Gastro Intestinal Bleeding DR - muayAD ABASSDocument59 pagesGastro Intestinal Bleeding DR - muayAD ABASSMAFADHELNo ratings yet
- Cervical LymphadenopathyDocument42 pagesCervical LymphadenopathyQuranSunnatNo ratings yet
- IgA Nephropathy and IgA Vasculitis: Pathogenesis, Clinical Manifestations, and TreatmentDocument52 pagesIgA Nephropathy and IgA Vasculitis: Pathogenesis, Clinical Manifestations, and TreatmentDr Rida And Shoaib VideosNo ratings yet
- Postoperative Fever - UpToDate PDFDocument25 pagesPostoperative Fever - UpToDate PDFkatsuiaNo ratings yet
- Hospital: Ms .Neethu Vincent Asst Professor KVM College of NursingDocument29 pagesHospital: Ms .Neethu Vincent Asst Professor KVM College of NursingNeethu VincentNo ratings yet
- Case Presentation: by Michael ArmstrongDocument21 pagesCase Presentation: by Michael ArmstrongWirawan Amirul BahriNo ratings yet
- Thalassemia: Dr. Deep Shah Under Guidance of Dr. Krutika Ma'Am and Dr. Rahul SirDocument46 pagesThalassemia: Dr. Deep Shah Under Guidance of Dr. Krutika Ma'Am and Dr. Rahul SirDeep ShahNo ratings yet
- Pemphigus VulgarisDocument21 pagesPemphigus VulgarisGina Kissey100% (1)
- Acute Pancreatitis NOTESDocument17 pagesAcute Pancreatitis NOTESsameeha semiNo ratings yet
- Neuroblastoma: A Cancer of the Sympathetic Nervous SystemDocument153 pagesNeuroblastoma: A Cancer of the Sympathetic Nervous SystemWael ElsawyNo ratings yet
- A. Brief Definition of The Specific Disease Condition: Mechanism CauseDocument6 pagesA. Brief Definition of The Specific Disease Condition: Mechanism CauseEuniceNo ratings yet
- Understanding Toxic Epidermal NecrolysisDocument13 pagesUnderstanding Toxic Epidermal NecrolysisHend AbdallaNo ratings yet
- Critical Care Update PDFDocument25 pagesCritical Care Update PDFHugo PozoNo ratings yet
- Urolithiasis SeminarDocument50 pagesUrolithiasis SeminarSiddharth GuptaNo ratings yet
- Emergency DepartmentDocument9 pagesEmergency DepartmentSarah Mae SanchezNo ratings yet
- Embolism and InfarctionDocument34 pagesEmbolism and InfarctionDiviya ArikrishnanNo ratings yet
- Types and Causes of HemorrhageDocument26 pagesTypes and Causes of HemorrhagepriyagidhuNo ratings yet
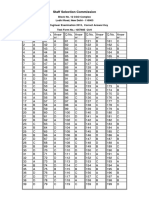
- SSC JE 2015 Exam Correct Answer Key for Test Form 1057685Document2 pagesSSC JE 2015 Exam Correct Answer Key for Test Form 1057685prashanthNo ratings yet
- Notice Result Extend - NursingOfficer - 2019Document1 pageNotice Result Extend - NursingOfficer - 2019prashanthNo ratings yet
- Advt of Nursing Officer For 4 AIIMS - 1Document10 pagesAdvt of Nursing Officer For 4 AIIMS - 1prashanthNo ratings yet
- Addendum For PWBD For Online RegDocument1 pageAddendum For PWBD For Online Regprashanth100% (1)
- Final Result - Nursing Officer Central Hospitals-2019-NETDocument17 pagesFinal Result - Nursing Officer Central Hospitals-2019-NETprashanthNo ratings yet
- Project ReportDocument2 pagesProject ReportprashanthNo ratings yet
- HMIS Kerala RevisedDocument34 pagesHMIS Kerala RevisedprashanthNo ratings yet
- Medical MalpracticeDocument41 pagesMedical MalpracticeprashanthNo ratings yet
- Cghs Nabh Application HospitalDocument27 pagesCghs Nabh Application HospitalGaurav SharmaNo ratings yet
- M.O.S.C.College of Nursing 3 Year BSC Nursing Pattern of ExaminationDocument1 pageM.O.S.C.College of Nursing 3 Year BSC Nursing Pattern of ExaminationprashanthNo ratings yet
- United India Insurance Recruitment for 300+ VacanciesDocument29 pagesUnited India Insurance Recruitment for 300+ VacanciesRavi SrivastavaNo ratings yet
- Your Bibliography VancouverDocument1 pageYour Bibliography VancouverprashanthNo ratings yet
- Post Basic BSC Admn PlanDocument2 pagesPost Basic BSC Admn PlanprashanthNo ratings yet
- M.O.S.C.College of Nursing, Kolenchery 3Rd Year B.Sc. Nursing Degree Course (2013-17 Batch) Clinical PlanDocument12 pagesM.O.S.C.College of Nursing, Kolenchery 3Rd Year B.Sc. Nursing Degree Course (2013-17 Batch) Clinical PlanprashanthNo ratings yet
- 8TIME TABLE - 2013 Batch Third YearDocument2 pages8TIME TABLE - 2013 Batch Third YearprashanthNo ratings yet
- 2TIME TABLE - 2013 Batch Third YearDocument2 pages2TIME TABLE - 2013 Batch Third YearprashanthNo ratings yet
- 2TIME TABLE - 2013 Batch Third YearDocument2 pages2TIME TABLE - 2013 Batch Third YearprashanthNo ratings yet
- M.O.S.C College of Nursing Kolenchery: Anecdotal RecordDocument5 pagesM.O.S.C College of Nursing Kolenchery: Anecdotal RecordprashanthNo ratings yet
- Martha RogerDocument10 pagesMartha RogerprashanthNo ratings yet
- Seminar On BUDGETDocument14 pagesSeminar On BUDGETprashanth60% (5)
- Physical ExaminationDocument39 pagesPhysical ExaminationprashanthNo ratings yet
- OremDocument12 pagesOremprashanthNo ratings yet
- Bowel IncontinenceDocument4 pagesBowel IncontinenceprashanthNo ratings yet
- Diabetic Foot Care OverviewDocument21 pagesDiabetic Foot Care Overviewprashanth100% (4)
- ANP Clinical Rotation 2015 SinuDocument4 pagesANP Clinical Rotation 2015 SinuprashanthNo ratings yet
- M.O.S.C College Psychiatric Nursing FormsDocument5 pagesM.O.S.C College Psychiatric Nursing FormsprashanthNo ratings yet
- Calculation of Clinical HoursDocument1 pageCalculation of Clinical HoursprashanthNo ratings yet
- Unit Plan Mental Health NursingDocument2 pagesUnit Plan Mental Health Nursingprashanth100% (2)
- Tuners SndromeDocument9 pagesTuners SndromeprashanthNo ratings yet
- Assessment Format Mental Health NursingDocument11 pagesAssessment Format Mental Health Nursingprashanth100% (1)
- Qad Quick StartDocument534 pagesQad Quick StartMahadev Subramani100% (1)
- Nagina Cotton Mills Annual Report 2007Document44 pagesNagina Cotton Mills Annual Report 2007Sonia MukhtarNo ratings yet
- Indian Journal of Natural Products and Resources Vol 1 No 4 Phytochemical pharmacological profile Cassia tora overviewDocument8 pagesIndian Journal of Natural Products and Resources Vol 1 No 4 Phytochemical pharmacological profile Cassia tora overviewPRINCIPAL BHILWARANo ratings yet
- Speed Reducer GearboxDocument14 pagesSpeed Reducer Gearboxعبد للهNo ratings yet
- Week 15 - Rams vs. VikingsDocument175 pagesWeek 15 - Rams vs. VikingsJMOTTUTNNo ratings yet
- PeopleSoft Security TablesDocument8 pagesPeopleSoft Security TablesChhavibhasinNo ratings yet
- EIRA v0.8.1 Beta OverviewDocument33 pagesEIRA v0.8.1 Beta OverviewAlexQuiñonesNietoNo ratings yet
- Ultra Slimpak G448-0002: Bridge Input Field Configurable IsolatorDocument4 pagesUltra Slimpak G448-0002: Bridge Input Field Configurable IsolatorVladimirNo ratings yet
- Methods to estimate stakeholder views of sustainabilityDocument7 pagesMethods to estimate stakeholder views of sustainabilityAlireza FatemiNo ratings yet
- Gabinete STS Activity1Document2 pagesGabinete STS Activity1Anthony GabineteNo ratings yet
- Paradigms of ManagementDocument2 pagesParadigms of ManagementLaura TicoiuNo ratings yet
- LEARNING ACTIVITY Sheet Math 7 q3 M 1Document4 pagesLEARNING ACTIVITY Sheet Math 7 q3 M 1Mariel PastoleroNo ratings yet
- MA1201 Calculus and Basic Linear Algebra II Solution of Problem Set 4Document10 pagesMA1201 Calculus and Basic Linear Algebra II Solution of Problem Set 4Sit LucasNo ratings yet
- I Will Be Here TABSDocument7 pagesI Will Be Here TABSEric JaoNo ratings yet
- Extrajudicial Settlement of Estate Rule 74, Section 1 ChecklistDocument8 pagesExtrajudicial Settlement of Estate Rule 74, Section 1 ChecklistMsyang Ann Corbo DiazNo ratings yet
- Form 709 United States Gift Tax ReturnDocument5 pagesForm 709 United States Gift Tax ReturnBogdan PraščevićNo ratings yet
- Key Fact Sheet (HBL FreedomAccount) - July 2019 PDFDocument1 pageKey Fact Sheet (HBL FreedomAccount) - July 2019 PDFBaD cHaUhDrYNo ratings yet
- Marshall Stability Test AnalysisDocument5 pagesMarshall Stability Test AnalysisZick Zickry50% (2)
- Combined Set12Document159 pagesCombined Set12Nguyễn Sơn LâmNo ratings yet
- Cover Letter PDFDocument1 pageCover Letter PDFAli EjazNo ratings yet
- 3d Control Sphere Edge and Face StudyDocument4 pages3d Control Sphere Edge and Face Studydjbroussard100% (2)
- OS LabDocument130 pagesOS LabSourav BadhanNo ratings yet
- AA ActivitiesDocument4 pagesAA ActivitiesSalim Amazir100% (1)
- Consumers ' Usage and Adoption of E-Pharmacy in India: Mallika SrivastavaDocument16 pagesConsumers ' Usage and Adoption of E-Pharmacy in India: Mallika SrivastavaSundaravel ElangovanNo ratings yet
- Unit 14 Ergonomics Design: AND ProductDocument24 pagesUnit 14 Ergonomics Design: AND ProductRämêşh KątúřiNo ratings yet
- Ratio Analysis of PIADocument16 pagesRatio Analysis of PIAMalik Saad Noman100% (5)
- Final Year Project (Product Recommendation)Document33 pagesFinal Year Project (Product Recommendation)Anurag ChakrabortyNo ratings yet
- Brochure en 2014 Web Canyon Bikes How ToDocument36 pagesBrochure en 2014 Web Canyon Bikes How ToRadivizija PortalNo ratings yet
- Laryngeal Diseases: Laryngitis, Vocal Cord Nodules / Polyps, Carcinoma LarynxDocument52 pagesLaryngeal Diseases: Laryngitis, Vocal Cord Nodules / Polyps, Carcinoma LarynxjialeongNo ratings yet
- List of Reactive Chemicals - Guardian Environmental TechnologiesDocument69 pagesList of Reactive Chemicals - Guardian Environmental TechnologiesGuardian Environmental TechnologiesNo ratings yet