You might also like
- ACS ATLS 1993 Test #1 9: 5/16/17, 4G38 PM Page 1 of 11Document11 pagesACS ATLS 1993 Test #1 9: 5/16/17, 4G38 PM Page 1 of 11Joshua Runtuwene100% (2)
- Highland Guidelines - LDK 2013-2-15Document3 pagesHighland Guidelines - LDK 2013-2-15andrew herringNo ratings yet
- Thoracotomy Through The Auscultatory Triangle - Ann Thorac Surg.1989Document2 pagesThoracotomy Through The Auscultatory Triangle - Ann Thorac Surg.1989Adriana PavelNo ratings yet
- Emergency Ultrasound Course-Textbook Update 23 Sept 2008-AdiDocument194 pagesEmergency Ultrasound Course-Textbook Update 23 Sept 2008-AdiHaswady Husaini100% (6)
- K Opiods For Pain BupDocument2 pagesK Opiods For Pain Bupandrew herringNo ratings yet
- Final SurgeryDocument35 pagesFinal SurgeryChinniah RamkumarNo ratings yet
- Chart Bodyblade Exercise Wall ChartDocument1 pageChart Bodyblade Exercise Wall ChartJ.w. Laster100% (1)
- Otolaryngology Mcqs & SBAs 2nd EditionDocument6 pagesOtolaryngology Mcqs & SBAs 2nd EditionJohn M. Hemsworth100% (1)
- FP Form ItrDocument2 pagesFP Form ItrAlibasher Macalnas100% (1)
- Raheel OSCE Notes January 2023Document453 pagesRaheel OSCE Notes January 2023KamleshKumar100% (1)
- Case Report ESPB AnakDocument11 pagesCase Report ESPB Anakmartindeng92_mdNo ratings yet
- Abat F. 2019. Comparison US Guided vs. Blind Interventions Supraspinatus TendinopathyDocument10 pagesAbat F. 2019. Comparison US Guided vs. Blind Interventions Supraspinatus TendinopathyJavier MartinNo ratings yet
- 6Document8 pages6Mihai PopescuNo ratings yet
- Transversus Abdominis Plane (Tap) BlockDocument6 pagesTransversus Abdominis Plane (Tap) BlockSuresh KumarNo ratings yet
- Brachial Plexus Injury in Adult: Comparative Effectiveness of Anterior and Posterior Approach For Shoulder FunctionDocument4 pagesBrachial Plexus Injury in Adult: Comparative Effectiveness of Anterior and Posterior Approach For Shoulder FunctionMedical JournalNo ratings yet
- Regional Anaesthesia: Case ReportDocument6 pagesRegional Anaesthesia: Case ReportChristian Adiputra WijayaNo ratings yet
- Real-Time Ultrasound-Guided Paramedian Epidural Access: Evaluation of A Novel In-Plane TechniqueDocument10 pagesReal-Time Ultrasound-Guided Paramedian Epidural Access: Evaluation of A Novel In-Plane TechniqueANGELICANo ratings yet
- Yoshida Proximal Obturator Nerve BlockDocument7 pagesYoshida Proximal Obturator Nerve BlockFACULTY FOLDERSNo ratings yet
- Ultrasound-Guided Block of TheDocument6 pagesUltrasound-Guided Block of Theandrew herringNo ratings yet
- Content ServerDocument8 pagesContent ServerKennie RamirezNo ratings yet
- Anatomy de NeckDocument17 pagesAnatomy de NeckAnonymous yv4iLzsKtgNo ratings yet
- Art3a10 10072fs00256-014-1842-5Document9 pagesArt3a10 10072fs00256-014-1842-5api-253958760No ratings yet
- Role of Conventional Radiology and Mri Defecography of Pelvic Floor HerniasDocument7 pagesRole of Conventional Radiology and Mri Defecography of Pelvic Floor HerniasNurul AprilianiNo ratings yet
- Echo 6Document10 pagesEcho 6Indera VyasNo ratings yet
- The Erector Spinae Plane Block: A Review of Current EvidenceDocument11 pagesThe Erector Spinae Plane Block: A Review of Current Evidencetnim.dsNo ratings yet
- Fleischmann - PS03 - Thoracic Paravertebral Blocks PDFDocument8 pagesFleischmann - PS03 - Thoracic Paravertebral Blocks PDFapippasaNo ratings yet
- 1996-Thoracic Paravertebral Space LocationDocument3 pages1996-Thoracic Paravertebral Space LocationRubén Darío HerediaNo ratings yet
- Comparative Anatomical Analysis of The Transcallosal-Transchoroidal and Transcallosal-Transforniceal-Transchoroidal Approaches To The Third VentricleDocument10 pagesComparative Anatomical Analysis of The Transcallosal-Transchoroidal and Transcallosal-Transforniceal-Transchoroidal Approaches To The Third VentricleZeptalanNo ratings yet
- Occipital Bi-Transtentorial-Falcine Approach For Falcotentorial MeningiomaDocument3 pagesOccipital Bi-Transtentorial-Falcine Approach For Falcotentorial MeningiomaMarcelo LambertiNo ratings yet
- Thoracic Ultrasound and Integrated ImagingFrom EverandThoracic Ultrasound and Integrated ImagingFrancesco FelettiNo ratings yet
- Transmission of Vertical Whole Body Vibration To The Human BodyDocument8 pagesTransmission of Vertical Whole Body Vibration To The Human BodyKutya kompNo ratings yet
- Thora CosDocument20 pagesThora CosDani VélezNo ratings yet
- Proximal Radial Compression Neuropathy: Brian Rinker, MD, Charles R. Effron, MD, and Robert W. Beasley, MDDocument7 pagesProximal Radial Compression Neuropathy: Brian Rinker, MD, Charles R. Effron, MD, and Robert W. Beasley, MDRod VRNo ratings yet
- Rib Fracture SerratusDocument3 pagesRib Fracture Serratusandrew herring100% (1)
- First Dorsal Metacarpal Artery Flap For Thumb Reconstruction: A Retrospective Clinical StudyDocument7 pagesFirst Dorsal Metacarpal Artery Flap For Thumb Reconstruction: A Retrospective Clinical StudyAry YounusNo ratings yet
- JurnalDocument16 pagesJurnalsamuelionardiNo ratings yet
- Beaulieu J. Y. 2006 Cerebral Plasticity in Crossed C7 Grafts of The Brachial Plexus An fMRI StudyDocument8 pagesBeaulieu J. Y. 2006 Cerebral Plasticity in Crossed C7 Grafts of The Brachial Plexus An fMRI StudyTatiane SantosNo ratings yet
- Randomiazdo-Fono Dexa CervicalDocument5 pagesRandomiazdo-Fono Dexa CervicalELONo ratings yet
- Neurosurg Focus Article Pe2Document16 pagesNeurosurg Focus Article Pe2mohammed isam al hajNo ratings yet
- Real-Time Ultrasound-Guided Percutaneous Dilatational Tracheostomy A Feasibility StudyDocument10 pagesReal-Time Ultrasound-Guided Percutaneous Dilatational Tracheostomy A Feasibility Studyroflova1908No ratings yet
- Ultrasound-Guided Continuous Erector Spinae Plane Block in Open Nephrectomy For Renal MalignancyDocument8 pagesUltrasound-Guided Continuous Erector Spinae Plane Block in Open Nephrectomy For Renal Malignancyindex PubNo ratings yet
- Research ArticleDocument7 pagesResearch Articlefm_askaNo ratings yet
- Brachial Plexus Anesthesia: A Review of The Relevant Anatomy, Complications, and Anatomical VariationsDocument12 pagesBrachial Plexus Anesthesia: A Review of The Relevant Anatomy, Complications, and Anatomical VariationsLucille IlaganNo ratings yet
- Hip Medial ApproachDocument10 pagesHip Medial ApproachFadliArifNo ratings yet
- MR IntracranIal menIngIomas!!! Vazno!!!Document5 pagesMR IntracranIal menIngIomas!!! Vazno!!!StefanNo ratings yet
- Ultrasound-Guided Injections in The Lumbar Spine: Continuing EducationDocument5 pagesUltrasound-Guided Injections in The Lumbar Spine: Continuing EducationdeslitaNo ratings yet
- Anaesthesia For Shoulder Surgery 5: Alain Borgeat Georgios EkatodramisDocument15 pagesAnaesthesia For Shoulder Surgery 5: Alain Borgeat Georgios EkatodramisMathew MattNo ratings yet
- TAP BlockDocument5 pagesTAP BlockclaucardemilNo ratings yet
- US For Epidural. Anesth Analg 2017Document6 pagesUS For Epidural. Anesth Analg 2017tarekabdelkarem927No ratings yet
- Ultrasound Therapy For Calcific Tendinitis of The ShoulderDocument6 pagesUltrasound Therapy For Calcific Tendinitis of The ShoulderPedro LomaNo ratings yet
- Burst Fracture FinDocument11 pagesBurst Fracture Finbosnia agusNo ratings yet
- J.Surgical Approaches To Pineal Region Tumors.2001Document13 pagesJ.Surgical Approaches To Pineal Region Tumors.2001Kysy CodonNo ratings yet
- MCQ Ortho 1Document9 pagesMCQ Ortho 1Joanne NgimNo ratings yet
- Thoracoscopic Sympathectomy Techniques and OutcomesDocument15 pagesThoracoscopic Sympathectomy Techniques and OutcomesBeshoy KhelaNo ratings yet
- Superior Labrum Anterior-Posterior (SLAP) Tears: Evaluation of Three MR Signs On T2-Weighted ImagesDocument5 pagesSuperior Labrum Anterior-Posterior (SLAP) Tears: Evaluation of Three MR Signs On T2-Weighted ImagesdrsmithaNo ratings yet
- SD MiofascialDocument5 pagesSD MiofascialMarGarciaNo ratings yet
- Rapm Agosto 2010 Anatomia Del Canal Espinal Toraxico Por RMNDocument6 pagesRapm Agosto 2010 Anatomia Del Canal Espinal Toraxico Por RMNIvette M. Carroll D.No ratings yet
- Trans Versus Abdominis Plane BlockDocument7 pagesTrans Versus Abdominis Plane BlockIvette M. Carroll D.No ratings yet
- Results of Surgical TreatmentDocument4 pagesResults of Surgical TreatmentChristine Yohana SianturiNo ratings yet
- Gravity FAIRERDocument7 pagesGravity FAIRERJosh GreerNo ratings yet
- Abordaje Cigomato TransmandibularDocument14 pagesAbordaje Cigomato TransmandibularRafael LópezNo ratings yet
- Br. J. Anaesth.-2010-Meira-746-50Document5 pagesBr. J. Anaesth.-2010-Meira-746-50Retno SawitriNo ratings yet
- Guide To USDocument11 pagesGuide To USAdel HamadaNo ratings yet
- Pi Is 0022522319367212Document8 pagesPi Is 0022522319367212Robert ChristevenNo ratings yet
- Usmle MSKDocument12 pagesUsmle MSKstruzzNo ratings yet
- The Thoracic Anterior Spinal Cord Adhesion SyndromeDocument7 pagesThe Thoracic Anterior Spinal Cord Adhesion Syndromepaulina_810100% (1)
- Endoscopic Endonasal and Transorbital Routes To The Petrous Apex: Anatomic Comparative Study of Two PathwaysDocument13 pagesEndoscopic Endonasal and Transorbital Routes To The Petrous Apex: Anatomic Comparative Study of Two Pathwaysgabriele1977No ratings yet
- Roux 2013Document7 pagesRoux 2013andrew herringNo ratings yet
- Buprenorphine 2016-7-18Document1 pageBuprenorphine 2016-7-18andrew herringNo ratings yet
- Rib Fracture SerratusDocument3 pagesRib Fracture Serratusandrew herring100% (1)
- Intravenous Lidocaine To Treat Postoperative Pain : Lidocaína Intravenosa No Tratamento Da Dor Pós-OperatóriaDocument6 pagesIntravenous Lidocaine To Treat Postoperative Pain : Lidocaína Intravenosa No Tratamento Da Dor Pós-Operatóriaandrew herringNo ratings yet
- Rib Fracture W: PecsDocument8 pagesRib Fracture W: Pecsandrew herring100% (1)
- Ultrasound-Guided Block of TheDocument6 pagesUltrasound-Guided Block of Theandrew herringNo ratings yet
- Herring ED Intractable Abdominal pain-N+VDocument1 pageHerring ED Intractable Abdominal pain-N+Vandrew herringNo ratings yet
- 3.2.16.highland Emergency Medicine Journal Club Methods.2Document2 pages3.2.16.highland Emergency Medicine Journal Club Methods.2andrew herringNo ratings yet
- Ketamine As Rescue Treatment FDocument8 pagesKetamine As Rescue Treatment Fandrew herringNo ratings yet
- Dex For Dental Pain & SwellingDocument7 pagesDex For Dental Pain & Swellingandrew herring100% (1)
- Nej MR A 1511480Document9 pagesNej MR A 1511480Tohari Masidi AminNo ratings yet
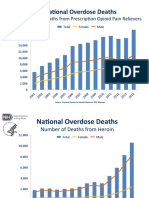
- OPR - Heroin DeathsDocument2 pagesOPR - Heroin Deathsandrew herringNo ratings yet
- CVS Action Plan v2Document1 pageCVS Action Plan v2andrew herringNo ratings yet
- Ultrasound Guided Interventional Procedures In.13Document14 pagesUltrasound Guided Interventional Procedures In.13andrew herring100% (1)
- Ultrasound Guided Interventional Procedures In.4Document13 pagesUltrasound Guided Interventional Procedures In.4andrew herringNo ratings yet
- Biomechanics of Side Impact: Injury Criteria, Aging Occupants, and Airbag TechnologyDocument17 pagesBiomechanics of Side Impact: Injury Criteria, Aging Occupants, and Airbag TechnologyStefanita CiunelNo ratings yet
- Physical Ass 2Document5 pagesPhysical Ass 2andreabreeNo ratings yet
- Medical MalalignmentDocument20 pagesMedical MalalignmentMihaela Tulbure100% (1)
- Evs 2nd STD FinalDocument29 pagesEvs 2nd STD FinalJay senthilNo ratings yet
- Bones of The Axial SkeletonDocument4 pagesBones of The Axial SkeletonJasminKate SutacioNo ratings yet
- EsseneHealingBreath PDFDocument13 pagesEsseneHealingBreath PDFJeremy100% (1)
- Active Cycle Breathing Technique-Easy DemoDocument3 pagesActive Cycle Breathing Technique-Easy DemoSenthilkumar ThiyagarajanNo ratings yet
- Care Plan Caesarian SectionDocument16 pagesCare Plan Caesarian Sectionpriyanka100% (1)
- Allen S Clinical Hints (Seror)Document479 pagesAllen S Clinical Hints (Seror)aldodiasNo ratings yet
- Blunt Chest TraumaDocument7 pagesBlunt Chest TraumaCatherine MorrisNo ratings yet
- Basic Trauma Life SupportDocument40 pagesBasic Trauma Life Supportyunita murfhiNo ratings yet
- Lec Activity15 Respiratory System 185522379Document17 pagesLec Activity15 Respiratory System 185522379Mariz GarganeraNo ratings yet
- Exercises (Basic Human Anatomy and Medical Terminologies)Document7 pagesExercises (Basic Human Anatomy and Medical Terminologies)tomaNo ratings yet
- Jason Wolfe's ATLS Trauma Moulage Page: (Thoughts On The Management of The Multiply Injured Patient)Document18 pagesJason Wolfe's ATLS Trauma Moulage Page: (Thoughts On The Management of The Multiply Injured Patient)gogopal100% (6)
- Medicare Rates January 2018Document679 pagesMedicare Rates January 2018Anna Wolfe0% (1)
- 5B Surgery 1st-2nd SE #28-32 #17-18Document3 pages5B Surgery 1st-2nd SE #28-32 #17-18Liza SoberkaayoNo ratings yet
- Chest Pain / Discomfort: DR (Brig) YD Singh Prof & Head Unit of MedicineDocument36 pagesChest Pain / Discomfort: DR (Brig) YD Singh Prof & Head Unit of MedicinenarmaNo ratings yet
- Anatomy 1linerDocument10 pagesAnatomy 1linersujsamNo ratings yet
- Chiropractic Adjusting TechniqueDocument111 pagesChiropractic Adjusting TechniqueDavid CristanchoNo ratings yet
- VAERS Adverse Events After Covid Vaccine MetallicDocument164 pagesVAERS Adverse Events After Covid Vaccine MetallicisNo ratings yet
- Newborn Resuscitation (Newborn CPR) BSN 12C: Madeline N. Gerzon, RN, MM Clinical Instructor Davao Doctors CollegeDocument59 pagesNewborn Resuscitation (Newborn CPR) BSN 12C: Madeline N. Gerzon, RN, MM Clinical Instructor Davao Doctors CollegemgerzonNo ratings yet
- NephrectomyDocument30 pagesNephrectomyIkhwan MusaNo ratings yet
- Combining Form SummaryDocument24 pagesCombining Form Summaryapi-57828209No ratings yet
- PA (Revised)Document16 pagesPA (Revised)Daryl Jake FornollesNo ratings yet