You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
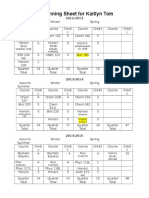
- 4 YearplanDocument3 pages4 Yearplanapi-314200814No ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Critical Incident EssayDocument2 pagesCritical Incident Essayapi-314200814No ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Honors 394 Music Presentation-2Document14 pagesHonors 394 Music Presentation-2api-314200814No ratings yet
- Henrietta Lacks PaperDocument7 pagesHenrietta Lacks Paperapi-314200814No ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Veterinary Nurses Practical Guide To Small Animal Anaesthesia Niamh Clancy All ChapterDocument67 pagesThe Veterinary Nurses Practical Guide To Small Animal Anaesthesia Niamh Clancy All Chapterlinda.mitchelle597100% (6)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Ebook Hadzics Textbook of Regional Anesthesia and Acute Pain Management Self Assessment and Review PDF Full Chapter PDFDocument68 pagesEbook Hadzics Textbook of Regional Anesthesia and Acute Pain Management Self Assessment and Review PDF Full Chapter PDFdonald.mortensen170100% (23)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Hadzic's Peripheral Nerve Blocks and Anatomy For Ultrasound Guided Regional Anesthesia (New York School of Regional Anesthesia) PDF DownloadDocument3 pagesHadzic's Peripheral Nerve Blocks and Anatomy For Ultrasound Guided Regional Anesthesia (New York School of Regional Anesthesia) PDF Downloadhellena buks33% (3)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Dissertation Chronic PainDocument4 pagesDissertation Chronic PainWriteMyCollegePaperForMeSingapore100% (1)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Hadzics Peripheral Nerve Blocks and Anatomy For Ultrasound Guided Regional Anesthesia 3Rd Edition Admir Hadzic Full ChapterDocument52 pagesHadzics Peripheral Nerve Blocks and Anatomy For Ultrasound Guided Regional Anesthesia 3Rd Edition Admir Hadzic Full Chaptercatherine.jonas226100% (7)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Bedah Buku InstrumenDocument12 pagesBedah Buku Instrumencoffe latteNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Incidence of Complications of Inferior Alveolar Nrve BlockDocument6 pagesIncidence of Complications of Inferior Alveolar Nrve Blockmatias112No ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Jinlei Li, Wei Jiang, Nalini Vadivelu - First Aid Perioperative Ultrasound - Acute Pain Manual For Surgical Procedures (2023, Springer)Document668 pagesJinlei Li, Wei Jiang, Nalini Vadivelu - First Aid Perioperative Ultrasound - Acute Pain Manual For Surgical Procedures (2023, Springer)Inês BatistaNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Peripheral NerveblockproductsbrochureDocument12 pagesPeripheral NerveblockproductsbrochureNS Biomendical Equipments service pvt ltdNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Local Anesthesia and Anxiolytic Techniques For Oculoplastic SurgeryDocument8 pagesLocal Anesthesia and Anxiolytic Techniques For Oculoplastic SurgeryFrancisco Javier Rodriguez MolinaNo ratings yet
- To Evaluate The Efficacy of Ultrasonography Guided Pectoral Nerve Block For Postoperative Analgesia in Breast SurgeriesDocument4 pagesTo Evaluate The Efficacy of Ultrasonography Guided Pectoral Nerve Block For Postoperative Analgesia in Breast SurgeriesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Anesthesia For Ophthalmic Surgery: An Educational ReviewDocument9 pagesAnesthesia For Ophthalmic Surgery: An Educational ReviewDAMIAN MERCADO BENTNo ratings yet
- Comparación Articaina y LidocainaDocument6 pagesComparación Articaina y LidocainaYonatan MorenoNo ratings yet
- Test 6 - Pharmacology & AnesthesiologyDocument5 pagesTest 6 - Pharmacology & Anesthesiologydr.jah9No ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Regional Anesthesia - FinalDocument46 pagesRegional Anesthesia - Finalvan016_bunnyNo ratings yet
- Ebook Hadzics Peripheral Nerve Blocks and Anatomy For Ultrasound Guided Regional Anesthesia PDF Full Chapter PDFDocument67 pagesEbook Hadzics Peripheral Nerve Blocks and Anatomy For Ultrasound Guided Regional Anesthesia PDF Full Chapter PDFdonald.mortensen170100% (26)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Gulf Pain School Webinar Series II - Program - 0Document5 pagesGulf Pain School Webinar Series II - Program - 0NIKOLAOS SYRMOSNo ratings yet
- Efficacy of Adductor Canal Block in Total Knee Arthroplasty: A Systematic ReviewDocument10 pagesEfficacy of Adductor Canal Block in Total Knee Arthroplasty: A Systematic ReviewHalim SudonoNo ratings yet
- Simple Anesthesia TechniqueDocument3 pagesSimple Anesthesia TechniqueBharathiNo ratings yet
- Ultrasound-Guided Nerve Blocks in The Head and Neck For Chronic Pain Management - The Anatomy, Sonoanatomy, and ProcedureDocument16 pagesUltrasound-Guided Nerve Blocks in The Head and Neck For Chronic Pain Management - The Anatomy, Sonoanatomy, and Proceduremarcus moraisNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Chapter 2 Anesthesia Services Current Procedural Terminology CPT Codes 00000 - 01999Document13 pagesChapter 2 Anesthesia Services Current Procedural Terminology CPT Codes 00000 - 01999shafilcr07No ratings yet
- 46686-Article Text-153299-1-10-20200420Document3 pages46686-Article Text-153299-1-10-20200420H.M. TouhidNo ratings yet
- 14Document10 pages14Juliana ObandoNo ratings yet
- Perioperative Concepts and Nursing Management: NCM 112-LecturerDocument98 pagesPerioperative Concepts and Nursing Management: NCM 112-LecturerJaylord Verazon100% (1)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- CircumcisionDocument38 pagesCircumcisionChalie MequanentNo ratings yet
- Genitofemoral Nerve Block: DurationDocument2 pagesGenitofemoral Nerve Block: DurationIshwar MeenaNo ratings yet
- Anesthesia Board Review Flashcards - QuizletDocument47 pagesAnesthesia Board Review Flashcards - QuizletDENTAL REVIEWER ONLYNo ratings yet
- Anesthetic Considerations in Dental SpecialtiesDocument10 pagesAnesthetic Considerations in Dental SpecialtiesOmar FawazNo ratings yet
- A Case of Occipital NeuralgiaDocument20 pagesA Case of Occipital NeuralgiaLakNo ratings yet
- A New Classification of Lip Zones To Customize Injectable Lip AugmentationDocument5 pagesA New Classification of Lip Zones To Customize Injectable Lip AugmentationClaudia Antonia Ortiz PeraltaNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)