You might also like
- Cardiac Arrythmias in The ED Menbeu Edited From AnaDocument106 pagesCardiac Arrythmias in The ED Menbeu Edited From AnaTemesgen Geleta100% (1)
- Assessing and Preventing Pressure UlcersDocument8 pagesAssessing and Preventing Pressure UlcersTamil VillardoNo ratings yet
- Risk-For-Fluid-And-Electrolyte-Imbalance Sample NCPDocument2 pagesRisk-For-Fluid-And-Electrolyte-Imbalance Sample NCPDuane Liloc67% (3)
- NCP-Deficient Fluid VolumeDocument1 pageNCP-Deficient Fluid Volumejanmichael8No ratings yet
- NonunionsDocument350 pagesNonunionsGreenIron9100% (2)
- Fluid Volume Excess (CRF)Document4 pagesFluid Volume Excess (CRF)NursesLabs.com100% (1)
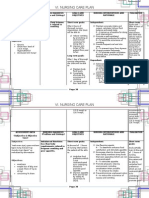
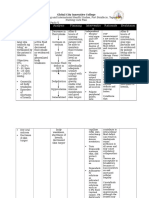
- Nursing Care Plan: Assessment Diagnosis Inference Planning Intervention Rationale EvaluationDocument3 pagesNursing Care Plan: Assessment Diagnosis Inference Planning Intervention Rationale EvaluationAbdallah AlasalNo ratings yet
- Nursing Care Plan for Skin IntegrityDocument3 pagesNursing Care Plan for Skin IntegrityCrystal Joy Misa100% (1)
- Nursing Care Plan For "Fluid and Electrolyte Imbalances"Document37 pagesNursing Care Plan For "Fluid and Electrolyte Imbalances"jhonroks90% (50)
- NCP On Electrolyte ImbalanceDocument4 pagesNCP On Electrolyte Imbalancefreyah_bc67% (3)
- NCP Fluid and Electrolyte ImbalanceDocument3 pagesNCP Fluid and Electrolyte ImbalanceVitha100% (1)
- NCP Electrolyte ImbalanceDocument2 pagesNCP Electrolyte ImbalanceSarah Benjamin100% (1)
- NCP DehydrationDocument4 pagesNCP DehydrationYnah Sayoc100% (2)
- NCP Altered ComfortDocument2 pagesNCP Altered ComfortColleen De la Rosa50% (2)
- Nursing Care Plan: Fluid Volume Deficit R/T Active Fluid Loss (Increased Urine Output)Document9 pagesNursing Care Plan: Fluid Volume Deficit R/T Active Fluid Loss (Increased Urine Output)Gayu Patel100% (2)
- Long Term: PT Will Demonstrate Increased Tolerance To Activity by DischargeDocument18 pagesLong Term: PT Will Demonstrate Increased Tolerance To Activity by DischargeMary Ann Ebol0% (1)
- NCP Fluid Volume DeficitDocument2 pagesNCP Fluid Volume DeficitRez Apego0% (1)
- NCP - Fluid and Electrolyte ImbalanceDocument3 pagesNCP - Fluid and Electrolyte ImbalancePaolo Belleza78% (9)
- NURSING CARE PLAN FOR GASTROESOPHAGEAL REFLUX DISEASEDocument1 pageNURSING CARE PLAN FOR GASTROESOPHAGEAL REFLUX DISEASEANGELICA JANE FLORENDONo ratings yet
- NCP For Deficient Fluid VolumeDocument2 pagesNCP For Deficient Fluid VolumeRedwing_Dc_854758% (12)
- ASSESSMENT OUTCOMES INTERVENTIONS RATIONALE EVALUATIONDocument4 pagesASSESSMENT OUTCOMES INTERVENTIONS RATIONALE EVALUATIONArian May Marcos100% (1)
- Benign Febrile ConvulsionDocument9 pagesBenign Febrile ConvulsionRoxanne Mae Marcelo BadongenNo ratings yet
- Impaired Physical MobilityDocument8 pagesImpaired Physical MobilityKM78% (9)
- English Grade 6 3RD QuarterDocument9 pagesEnglish Grade 6 3RD Quartersarah ubaNo ratings yet
- NCP - Deficient Fluid VolumeDocument2 pagesNCP - Deficient Fluid VolumerobbychuaNo ratings yet
- Nursing Care Plan Ineffective Tissue PerfusionDocument1 pageNursing Care Plan Ineffective Tissue Perfusionderic83% (29)
- NCP Deficient Fluid Volume Related To Fluid Loss DHNDocument2 pagesNCP Deficient Fluid Volume Related To Fluid Loss DHNMa. Elaine Carla Tating38% (8)
- Defient Fluid Volume Intake and Impaired Mobility NCPDocument6 pagesDefient Fluid Volume Intake and Impaired Mobility NCPjordan aguilarNo ratings yet
- NCP Impaiered Skin IntegrityDocument1 pageNCP Impaiered Skin Integrityeiram2264% (11)
- Nursing Care Plan Cues Diagnosis Justification: Sodium-132 Mmol/l (Low)Document3 pagesNursing Care Plan Cues Diagnosis Justification: Sodium-132 Mmol/l (Low)rei_alina75% (4)
- Nursing Care Plan Risk For Urinary RetentionDocument4 pagesNursing Care Plan Risk For Urinary RetentionReginald Julia100% (2)
- Imbalanced Nutrition Less Than Body Requirements Related To Altered Image, Inadequate Nutrient Intake, and Chronic Vomiting.Document2 pagesImbalanced Nutrition Less Than Body Requirements Related To Altered Image, Inadequate Nutrient Intake, and Chronic Vomiting.Senyorita KHaye100% (1)
- Infant BathingDocument5 pagesInfant BathingKYLE SABAYNo ratings yet
- Nursing Care Plan for Fluid Volume DeficitDocument2 pagesNursing Care Plan for Fluid Volume DeficitXtinego89% (9)
- NCP 3A Nutritional Imbalance Less ThanDocument3 pagesNCP 3A Nutritional Imbalance Less ThanCee Sanchez100% (3)
- Impaired Skin Integrity Related To Surgical Removal of SkinDocument3 pagesImpaired Skin Integrity Related To Surgical Removal of Skinnnaesor_10910% (2)
- Imbalanced Nutrition Less Than Body Requirements - Diabetes - NCPDocument5 pagesImbalanced Nutrition Less Than Body Requirements - Diabetes - NCPJulie Ann Jimenez Manlangit50% (4)
- NCP Risk For Fluid Volume DeficitDocument2 pagesNCP Risk For Fluid Volume DeficitJeanineReyes44% (9)
- NCP (Diarrhea)Document2 pagesNCP (Diarrhea)Rodj Bilang Jr.83% (30)
- Basic Life SupportDocument12 pagesBasic Life SupportFlorence De ChavezNo ratings yet
- NCP-Fluid Volume DeficitDocument2 pagesNCP-Fluid Volume Deficitanon_207994234100% (1)
- Fluid Volume Deficit Related To Loose Watery Stool Diarrhea)Document2 pagesFluid Volume Deficit Related To Loose Watery Stool Diarrhea)Jesse James Advincula Edjec100% (15)
- Activity Intolerance NCPDocument2 pagesActivity Intolerance NCPAlden MendozaNo ratings yet
- Knowledge Deficit - RegorDocument3 pagesKnowledge Deficit - RegorAdrian MallarNo ratings yet
- NCP - Nausea and VomitingDocument9 pagesNCP - Nausea and VomitingMikko Anthony Pingol Alarcon77% (13)
- Nursing Diagnosis # 1 Acute Pain Related To Abdominal Incision.Document10 pagesNursing Diagnosis # 1 Acute Pain Related To Abdominal Incision.jhunanax100% (3)
- NCPDocument3 pagesNCPDelaine Mae MierNo ratings yet
- Nursing Care PlanDocument23 pagesNursing Care PlanLorielle HernandezNo ratings yet
- Hypokalemia NCPDocument4 pagesHypokalemia NCPpauchanmnlNo ratings yet
- Nursing Care Plan for Electrolyte ImbalanceDocument8 pagesNursing Care Plan for Electrolyte ImbalanceManuel Jacob YradNo ratings yet
- Risk For Impaired Skin Integrity and Readiness For Enhanced PowerDocument3 pagesRisk For Impaired Skin Integrity and Readiness For Enhanced PowerdanaNo ratings yet
- Risk For Fluid and Electrolyte Imbalances Nursing Care PlanDocument1 pageRisk For Fluid and Electrolyte Imbalances Nursing Care PlanTrixia Dacles100% (1)
- n320 Peds NCP wk3Document2 pagesn320 Peds NCP wk3api-301826049No ratings yet
- Activity Intolerance Related To AmeniaDocument1 pageActivity Intolerance Related To AmeniaSiti Syazana Mohamad MogriNo ratings yet
- Hypertonic SolutionsDocument4 pagesHypertonic SolutionsVanessa PaguiriganNo ratings yet
- Daily NCPDocument5 pagesDaily NCPKuennie SabalNo ratings yet
- NCP 1Document1 pageNCP 1hsiriaNo ratings yet
- Fluid Volume DeficitDocument2 pagesFluid Volume DeficitRuby AnneNo ratings yet
- PDF NCP Electrolyte Imbalance - CompressDocument3 pagesPDF NCP Electrolyte Imbalance - Compressclaire yows100% (1)
- NCP FinalDocument7 pagesNCP FinalRuss RussNo ratings yet
- Hepatic EncephalopathyDocument3 pagesHepatic EncephalopathyJamaile GarciaNo ratings yet
- Nursing Problem PrioritizationDocument5 pagesNursing Problem PrioritizationJhen JhenNo ratings yet
- Nursing ProcessDocument40 pagesNursing ProcessRishiel Dimple BalonesNo ratings yet
- NCPDocument3 pagesNCPLuiji Amor TiamzonNo ratings yet
- Nursing Care Pla1Document1 pageNursing Care Pla1Btob meloNo ratings yet
- MedulloblastomaDocument67 pagesMedulloblastomaAmira YasmineNo ratings yet
- 3Document13 pages3Urologi Unpad Februari 2023No ratings yet
- ACNE VULGARIS 13 April 2020Document97 pagesACNE VULGARIS 13 April 2020afuw1605No ratings yet
- ALS Fact SheetDocument4 pagesALS Fact SheetGovar Miqdad GardiNo ratings yet
- Hep B PregnantDocument6 pagesHep B PregnantEman ShNo ratings yet
- Pulse OximetryDocument16 pagesPulse OximetryDineshkumarNo ratings yet
- Ethics On Consumers.Document7 pagesEthics On Consumers.Sujata KunduNo ratings yet
- NCP MaternalDocument21 pagesNCP MaternalDorothee GumisadNo ratings yet
- Cardiovascular Assessment: Assessment Uses of CVS AssessmentDocument8 pagesCardiovascular Assessment: Assessment Uses of CVS AssessmentKawaljit KaurNo ratings yet
- The Thromboelastogram (TEG®) : A Five-Minute Primer For The Emergency PhysicianDocument11 pagesThe Thromboelastogram (TEG®) : A Five-Minute Primer For The Emergency PhysicianMarcelliaNo ratings yet
- Urinary Tract Infections (UTI)Document32 pagesUrinary Tract Infections (UTI)Ruqaya HassanNo ratings yet
- 2 - Bedside Medicine 2 2019-2020Document32 pages2 - Bedside Medicine 2 2019-2020syed nomanshahNo ratings yet
- Faktor-Faktor Yang Berhubungan Dengan Kejadian Dermatitis Atopik Di Puskesmas Bangkinang KotaDocument10 pagesFaktor-Faktor Yang Berhubungan Dengan Kejadian Dermatitis Atopik Di Puskesmas Bangkinang KotaAsha NopatiNo ratings yet
- DSM-5 (R) Self-Exam Questions - Muskin, Philip R. (SRG) (Dragged)Document16 pagesDSM-5 (R) Self-Exam Questions - Muskin, Philip R. (SRG) (Dragged)Felipe HoraNo ratings yet
- Effectiveness of A Novel Topical Powder On The Treatment of Traumatic Oral PDFDocument8 pagesEffectiveness of A Novel Topical Powder On The Treatment of Traumatic Oral PDFpaolaNo ratings yet
- Tata Laksana Komprehensif Dermatitis Stasis Pada Geriatri: Ejournal Kedokteran Indonesia January 2022Document8 pagesTata Laksana Komprehensif Dermatitis Stasis Pada Geriatri: Ejournal Kedokteran Indonesia January 2022suci triana putriNo ratings yet
- Hyponatremia (Essay)Document3 pagesHyponatremia (Essay)Wan HafizNo ratings yet
- Helpful Questions For Oral RevalidaDocument6 pagesHelpful Questions For Oral RevalidaMomo CanNo ratings yet
- New MOU Format 2024Document15 pagesNew MOU Format 2024mohan kumarNo ratings yet
- Covid 19Document42 pagesCovid 19ok100% (3)
- PHP GUFo TLDocument2 pagesPHP GUFo TLARSLANNo ratings yet
- Hellp SyndromeDocument5 pagesHellp SyndromeJmarie Brillantes PopiocoNo ratings yet
- Venous InsufficiencyDocument32 pagesVenous InsufficiencyRalucaNo ratings yet
- Seaclean Plus 25 LTRDocument12 pagesSeaclean Plus 25 LTRspamalstublieft1832No ratings yet
- Vestibular Evoked Myogenic Potentials: Preliminary ReportDocument8 pagesVestibular Evoked Myogenic Potentials: Preliminary ReportHerminaElenaNo ratings yet