You might also like
- Descartes' Logarithmic Spiral ExplainedDocument8 pagesDescartes' Logarithmic Spiral Explainedcyberboy_875584No ratings yet
- Pinochle Rules GuideDocument2 pagesPinochle Rules GuidepatrickNo ratings yet
- Economics of Money Banking and Financial Markets 12th Edition Mishkin Solutions ManualDocument3 pagesEconomics of Money Banking and Financial Markets 12th Edition Mishkin Solutions Manualalexanderyanggftesimjac100% (15)
- Organizational Transformations: Population Ecology TheoryDocument25 pagesOrganizational Transformations: Population Ecology TheoryTurki Jarallah100% (2)
- Case StudyDocument21 pagesCase StudyLuige AvilaNo ratings yet
- Schneider Electric Strategy PresentationDocument10 pagesSchneider Electric Strategy PresentationDeepie KaurNo ratings yet
- Dave Jay S. Manriquez RN. Acute CholecystitisDocument11 pagesDave Jay S. Manriquez RN. Acute CholecystitisChilleMaeNo ratings yet
- Renal Calculi (NS Presentation)Document24 pagesRenal Calculi (NS Presentation)Norsyakira NawirNo ratings yet
- 1888 Speth Ars Quatuor Coronatorum v1Document280 pages1888 Speth Ars Quatuor Coronatorum v1Paulo Sequeira Rebelo100% (2)
- HydrocephalusDocument28 pagesHydrocephalusQurrataini Ibanez100% (1)
- Best Practices in Implementing A Secure Microservices ArchitectureDocument85 pagesBest Practices in Implementing A Secure Microservices Architecturewenapo100% (1)
- Nursing Care Plan (Bowel Elemination)Document8 pagesNursing Care Plan (Bowel Elemination)Rijane Tabonoc Omlang100% (1)
- PDFDocument72 pagesPDFGCMediaNo ratings yet
- Gallbladder Removal Recovery GuideDocument14 pagesGallbladder Removal Recovery GuideMarin HarabagiuNo ratings yet
- NCP - CapDocument4 pagesNCP - CapSherryNo ratings yet
- Test Initial Engleza A 8a Cu Matrice Si BaremDocument4 pagesTest Initial Engleza A 8a Cu Matrice Si BaremTatiana BeileșenNo ratings yet
- NCP Drug Study Group 1Document21 pagesNCP Drug Study Group 1Cassandra Grace Muerong Dela CruzNo ratings yet
- Pathophysiology AppendicitisDocument3 pagesPathophysiology AppendicitisIra Krystel ReyesNo ratings yet
- Intussusception: PathophysiologyDocument8 pagesIntussusception: PathophysiologyNaufal AndaluNo ratings yet
- Intussusception: DR Phillipo Leo ChalyaDocument19 pagesIntussusception: DR Phillipo Leo ChalyaSibabaong'ombe MasakaNo ratings yet
- H MoleDocument2 pagesH MoleJoanna Marie Datahan EstomoNo ratings yet
- Pathophysiology (Book-Based) : CystitisDocument9 pagesPathophysiology (Book-Based) : CystitisIrish EspinosaNo ratings yet
- Nursing Care Plan For Angina Pectoris NCPDocument2 pagesNursing Care Plan For Angina Pectoris NCPkarthi karthi100% (1)
- HYDROCELEDocument3 pagesHYDROCELESean Patrick Acoba100% (2)
- Case Study of Internal Hemorrhoids (IHDocument9 pagesCase Study of Internal Hemorrhoids (IHPearl Joy Diaz AnggotNo ratings yet
- Pathophysiology of Hyperemesis Gravidarum DiagramDocument1 pagePathophysiology of Hyperemesis Gravidarum DiagramQuintin MangaoangNo ratings yet
- Hydrocephalus 9Document9 pagesHydrocephalus 9Shesly PhilominaNo ratings yet
- Acute appendicitis symptoms and causesDocument20 pagesAcute appendicitis symptoms and causesAiyaz AliNo ratings yet
- Congenital HydrocephalusDocument11 pagesCongenital Hydrocephalusginafioravanti100% (6)
- Case Studies - Tetralogy of FallotDocument16 pagesCase Studies - Tetralogy of FallotKunwar Sidharth SaurabhNo ratings yet
- Schistosomiasis (From Anatomy To Pathophysiology)Document10 pagesSchistosomiasis (From Anatomy To Pathophysiology)Tiger Knee100% (1)
- Pathophysiology AbrasionDocument3 pagesPathophysiology AbrasionVito VitoNo ratings yet
- N. Bacalso Ave., Cebu City Philippines: Page 1 of 32Document32 pagesN. Bacalso Ave., Cebu City Philippines: Page 1 of 32Joule PeirreNo ratings yet
- Nursing Care Plan Placenta PreviaDocument2 pagesNursing Care Plan Placenta PreviaApril Ann HortilanoNo ratings yet
- Liver AbscessDocument3 pagesLiver AbscessStephanie Pe100% (1)
- Viii. Pathophysiology A. Overview of The Disease HypokalemiaDocument4 pagesViii. Pathophysiology A. Overview of The Disease HypokalemiaCleo Joyce C. CristalNo ratings yet
- HemorrhoidsDocument15 pagesHemorrhoidspologroNo ratings yet
- A Case Presentation On CholedocholithiasisDocument11 pagesA Case Presentation On CholedocholithiasisPaul Vincent EspereNo ratings yet
- DP Discharge Plan@@@@@@@@Document6 pagesDP Discharge Plan@@@@@@@@Maemae SumalinogNo ratings yet
- Pathophysiology of Rheumatic Heart Disease and FeverDocument3 pagesPathophysiology of Rheumatic Heart Disease and FeverDee SarajanNo ratings yet
- Hematologic (Blood) Diseases GuideDocument24 pagesHematologic (Blood) Diseases GuideMasha FloreaNo ratings yet
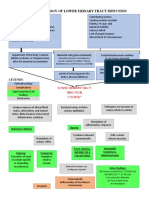
- Pathophysiology of Lower Urinary Tract InfectionDocument1 pagePathophysiology of Lower Urinary Tract InfectionSTORAGE FILENo ratings yet
- Drug StudyDocument5 pagesDrug StudyGAYOL BREEN IRAH A.No ratings yet
- Hirschsprung Disease Case Study: Maecy P. Tarinay BSN 4-1Document5 pagesHirschsprung Disease Case Study: Maecy P. Tarinay BSN 4-1Maecy OdegaardNo ratings yet
- 4 ConceptDocument1 page4 ConceptStacey GarciaNo ratings yet
- Intussuseption and Hirschprung's DiseaseDocument5 pagesIntussuseption and Hirschprung's DiseaseAris Magallanes100% (2)
- CataractDocument5 pagesCataractTriXie SorrillaNo ratings yet
- Nursing Care Plan for Hypertension ManagementDocument5 pagesNursing Care Plan for Hypertension Managementbhavana100% (1)
- Obstructive Lesions of the Urinary Tract: Causes and Pathophysiology of HydronephrosisDocument17 pagesObstructive Lesions of the Urinary Tract: Causes and Pathophysiology of HydronephrosisShradha Khurana100% (1)
- Hydronephrosis Fred LuceDocument69 pagesHydronephrosis Fred LuceKMNo ratings yet
- Assessment Nsg. Diagnosis Sci. Explanation Planning Intervention Rationale EvaluationDocument6 pagesAssessment Nsg. Diagnosis Sci. Explanation Planning Intervention Rationale EvaluationRoMarie AbainzaNo ratings yet
- UROLITHIASISDocument9 pagesUROLITHIASISmardsz100% (13)
- Acute Cholecystitis SeminarDocument42 pagesAcute Cholecystitis SeminarNatnaelNo ratings yet
- Ov Ov OvDocument15 pagesOv Ov OvHayyana Mae Taguba LadiaNo ratings yet
- Head To Toe Assessment of Infant CsepreDocument5 pagesHead To Toe Assessment of Infant CsepreteuuuuNo ratings yet
- Dysfunction at The First Stage of Labor: Prolonged Latent PhaseDocument5 pagesDysfunction at The First Stage of Labor: Prolonged Latent PhaseRam Dela PeñaNo ratings yet
- Case Presentation - CholelithiasisDocument35 pagesCase Presentation - Cholelithiasisarief2704900% (1)
- Tetralogy of FallotDocument5 pagesTetralogy of FallotCharity OaniaNo ratings yet
- Aklan State University Nursing Readings on Pyloric StenosisDocument5 pagesAklan State University Nursing Readings on Pyloric Stenosisensoooooooooo100% (1)
- Tetralogy of FallotDocument3 pagesTetralogy of FallotJohn Mark PocsidioNo ratings yet
- Anatomy and Physiology of The GallbladderDocument1 pageAnatomy and Physiology of The GallbladderRojanisa Baculi RomathoNo ratings yet
- CholelithiasisDocument6 pagesCholelithiasismarkzamNo ratings yet
- PP Insect Bite 2007 (Print)Document16 pagesPP Insect Bite 2007 (Print)Ali RumiNo ratings yet
- Nursing Care Plan 1: Diagnosis Goal Nursing Interventions RationaleDocument8 pagesNursing Care Plan 1: Diagnosis Goal Nursing Interventions RationaleTrysna Ayu SukardiNo ratings yet
- Cholelithiasis SneDocument12 pagesCholelithiasis SneSuhas IngaleNo ratings yet
- AmoebiasisDocument1 pageAmoebiasisYakumaNo ratings yet
- Cholecystitis With CholecystolithiasisDocument33 pagesCholecystitis With CholecystolithiasisDino V EscalonaNo ratings yet
- Right Hypochondrium Pain CausesDocument34 pagesRight Hypochondrium Pain CauseskhansamrNo ratings yet
- CHOLECYSTITIS With CHOLECYSTOLITHIASISDocument2 pagesCHOLECYSTITIS With CHOLECYSTOLITHIASISkennice_nereaNo ratings yet
- Chole ReportingDocument5 pagesChole ReportingMarcieNo ratings yet
- Cholecystitis Full With EditDocument43 pagesCholecystitis Full With Editmustafalotfy01No ratings yet
- VAP PresentationDocument17 pagesVAP PresentationSherryNo ratings yet
- Essential OET preparation strategiesDocument2 pagesEssential OET preparation strategiesSherryNo ratings yet
- Person Centered TherapyDocument13 pagesPerson Centered TherapySherryNo ratings yet
- Prostate DisturbancesDocument5 pagesProstate DisturbancesSherryNo ratings yet
- Understanding Seizures and EpilepsyDocument7 pagesUnderstanding Seizures and EpilepsySherryNo ratings yet
- Prostate DisturbancesDocument5 pagesProstate DisturbancesSherryNo ratings yet
- Phases of Wound HealingDocument7 pagesPhases of Wound HealingSherryNo ratings yet
- Bulimia NervosaDocument17 pagesBulimia NervosaSherryNo ratings yet
- The Pancreas: Functions, Inflammation, Diagnosis and TreatmentDocument4 pagesThe Pancreas: Functions, Inflammation, Diagnosis and TreatmentSherryNo ratings yet
- Suicidal Assessment (Sad Persons)Document18 pagesSuicidal Assessment (Sad Persons)SherryNo ratings yet
- Suicidal Assessment (Sad Persons)Document18 pagesSuicidal Assessment (Sad Persons)SherryNo ratings yet
- Registration Form: Advancement in I.C.Engine and Vehicle System"Document2 pagesRegistration Form: Advancement in I.C.Engine and Vehicle System"Weld TechNo ratings yet
- Year 7 Depth Study 2a 2020 5Document6 pagesYear 7 Depth Study 2a 2020 5api-508928238No ratings yet
- CAE-NUST College Aeronautical Engineering AssignmentDocument3 pagesCAE-NUST College Aeronautical Engineering AssignmentBahram TahirNo ratings yet
- Volleyball ReflectionDocument1 pageVolleyball ReflectionJake Santos100% (1)
- VET PREVENTIVE MEDICINE EXAMDocument8 pagesVET PREVENTIVE MEDICINE EXAMashish kumarNo ratings yet
- Labor DoctrinesDocument22 pagesLabor DoctrinesAngemeir Chloe FranciscoNo ratings yet
- Mock-B1 Writing ReadingDocument6 pagesMock-B1 Writing ReadingAnonymous 0uBSrduoNo ratings yet
- MS0800288 Angh enDocument5 pagesMS0800288 Angh enSeason AkhirNo ratings yet
- Facebook Use Case Diagram Activity Diagram Sequence DiagramDocument21 pagesFacebook Use Case Diagram Activity Diagram Sequence DiagramSaiNo ratings yet
- Urbanization As A Transformative Force: Quick FactsDocument20 pagesUrbanization As A Transformative Force: Quick FactsJulio CovarrubiasNo ratings yet
- NGOs Affiliated To SWCDocument2,555 pagesNGOs Affiliated To SWCMandip marasiniNo ratings yet
- Whole Brain Lesson Plan: 3 QuarterDocument5 pagesWhole Brain Lesson Plan: 3 QuarterNieve Marie Cerezo100% (1)
- Ariston Oven ManualDocument16 pagesAriston Oven ManualJoanne JoanneNo ratings yet
- Project Notes PackagingDocument4 pagesProject Notes PackagingAngrej Singh SohalNo ratings yet
- 6 Economics of International TradeDocument29 pages6 Economics of International TradeSenthil Kumar KNo ratings yet
- Integrating Force - Com With MicrosoftDocument11 pagesIntegrating Force - Com With MicrosoftSurajAluruNo ratings yet
- Oil Immersed TransformerDocument8 pagesOil Immersed TransformerAbdul JabbarNo ratings yet
- Slope StabilityDocument11 pagesSlope StabilityAhmed MohebNo ratings yet
- Art 1207-1257 CCDocument5 pagesArt 1207-1257 CCRubz JeanNo ratings yet
- Shah Wali Ullah Syed Haji Shariat Ullah Ahmad Barelvi (Notes)Document2 pagesShah Wali Ullah Syed Haji Shariat Ullah Ahmad Barelvi (Notes)Samreen KapasiNo ratings yet