You might also like
- Nursing Cheat LabValuesDocument4 pagesNursing Cheat LabValuessasukenoneko100% (5)
- Ineffective Airway Clearance Related To BronchospasmDocument2 pagesIneffective Airway Clearance Related To BronchospasmReylan Garcia100% (4)
- Oxygen TherapyDocument20 pagesOxygen TherapyPaul Gabriel CasquejoNo ratings yet
- Intravenous Flow Rate CalculationDocument7 pagesIntravenous Flow Rate CalculationCarmela Mabel Ansay PrincipeNo ratings yet
- Mbdqor345235235 PDFDocument482 pagesMbdqor345235235 PDFM HaidarNo ratings yet
- Mechanical Ventilator CareDocument9 pagesMechanical Ventilator CareAnusha Verghese100% (2)
- NCP For Community Acquired PnuemoniaDocument7 pagesNCP For Community Acquired PnuemoniaAshley Gaton Alindogan100% (1)
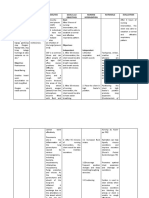
- Cues Nursing Diagnosis Analysis GOALS and Objectives Nursing Intervention Rationale Evaluation Subjective: GoalDocument4 pagesCues Nursing Diagnosis Analysis GOALS and Objectives Nursing Intervention Rationale Evaluation Subjective: GoalMonica Angelique SalayoNo ratings yet
- Gas GangreneDocument21 pagesGas GangreneSyaIra SamatNo ratings yet
- Nursing Care Plan:: Lopez, Maria Sofia B. 10/18/2020 3-BSN-B Prof. IsananDocument4 pagesNursing Care Plan:: Lopez, Maria Sofia B. 10/18/2020 3-BSN-B Prof. IsananSofia LopezNo ratings yet
- Nursing Care Plan for Community Acquired PneumoniaDocument2 pagesNursing Care Plan for Community Acquired PneumoniaEngely Mercader100% (1)
- NCP - Patient With Chest TubeDocument2 pagesNCP - Patient With Chest TubeSelwynVillamorPatente0% (1)
- NCP HemoDocument2 pagesNCP HemoJigs HechNo ratings yet
- Pleural EffusionDocument5 pagesPleural EffusionTerizla MobileNo ratings yet
- NCP For PneumoniaDocument3 pagesNCP For PneumoniaKahMallari100% (10)
- NCPDocument9 pagesNCPEjie Boy Isaga67% (3)
- NCP Ineffective Breathing ActualDocument3 pagesNCP Ineffective Breathing ActualArian May Marcos100% (1)
- Nebulization Therapy Guide for Respiratory ConditionsDocument5 pagesNebulization Therapy Guide for Respiratory ConditionsTamil Villardo100% (2)
- Drug Study FluimucilDocument2 pagesDrug Study FluimucilJemina Rafanan Racadio0% (1)
- NCPDocument4 pagesNCPAbegail Abaygar100% (1)
- BronchiectasisDocument40 pagesBronchiectasisyana jaeNo ratings yet
- Chapter 01 Introduction To Nursing PDFDocument7 pagesChapter 01 Introduction To Nursing PDFludwigs43100% (1)
- NCP PCAP CDocument4 pagesNCP PCAP CRio Bonifacio100% (2)
- Hemodialysis NCPDocument2 pagesHemodialysis NCPAfia Tawiah100% (1)
- Time Chart: Data Action ResponseDocument2 pagesTime Chart: Data Action ResponseAziil Liiza100% (2)
- NCP TBDocument6 pagesNCP TBGrhace Aquino100% (3)
- Asthma treatment steroid receptorDocument3 pagesAsthma treatment steroid receptorMuhammad Abubakar100% (1)
- Nursing Care Plan for Ineffective Airway ClearanceDocument2 pagesNursing Care Plan for Ineffective Airway ClearanceKenj Pereña100% (1)
- Effective airway clearance for pneumonia patientDocument5 pagesEffective airway clearance for pneumonia patientCamille Serrano100% (1)
- Goal:: Ineffective Airway Clearance Related To Cumulation of SecretionDocument4 pagesGoal:: Ineffective Airway Clearance Related To Cumulation of SecretionWyen CabatbatNo ratings yet
- Cap NCPDocument2 pagesCap NCPkyshb100% (2)
- St. Anthony's Nursing Care PlanDocument2 pagesSt. Anthony's Nursing Care PlanKristine Young100% (1)
- Risk For Infection Pneumonia Nursing Care PlanDocument1 pageRisk For Infection Pneumonia Nursing Care Planjustin_sane100% (1)
- History of SurgeryDocument35 pagesHistory of SurgeryImolaBakosNo ratings yet
- Nursing Care Plan Community Acquired PneumoniaDocument2 pagesNursing Care Plan Community Acquired Pneumoniaderic92% (50)
- DuaventDocument2 pagesDuaventKristine YoungNo ratings yet
- Community Acquired Pneumonia Nursing Care Plan: Demonstrate Pursed-Lip and Diaphragmatic Breathing To The PatientDocument4 pagesCommunity Acquired Pneumonia Nursing Care Plan: Demonstrate Pursed-Lip and Diaphragmatic Breathing To The PatientKrisianne Mae Lorenzo Francisco100% (1)
- Nursing Care Plan for Respiratory ConditionsDocument7 pagesNursing Care Plan for Respiratory ConditionsJonathan Delos ReyesNo ratings yet
- Cap NCPDocument6 pagesCap NCPMarlo Parayno100% (2)
- NCP For Ineffective Airway Clearance.Document2 pagesNCP For Ineffective Airway Clearance.Vanessa Joy Contreras100% (1)
- Impaired Gas Exchange PneumoniaDocument2 pagesImpaired Gas Exchange PneumoniaAngel Cabatingan100% (4)
- Nursing Care Plan For PcapDocument6 pagesNursing Care Plan For PcapMadsNo ratings yet
- ANOLIN, Marc Edriann T. Nursing Care Plan Assessmen T Diagnosis Rationale Planning Interventio N Rationale EvaluationDocument2 pagesANOLIN, Marc Edriann T. Nursing Care Plan Assessmen T Diagnosis Rationale Planning Interventio N Rationale EvaluationEdrianne Tui100% (2)
- NCP PneumoniaDocument2 pagesNCP Pneumonia_garonNo ratings yet
- NCP For Ineffective Airway ClearanceDocument3 pagesNCP For Ineffective Airway ClearanceJennelyn BayleNo ratings yet
- Nursing Care Plan - Ineffective Airway ClearanceDocument1 pageNursing Care Plan - Ineffective Airway ClearanceLei OrtegaNo ratings yet
- Ineffective Airway ClearanceDocument6 pagesIneffective Airway ClearanceBenly Grace Rebuyon MosquedaNo ratings yet
- Ineffective Airway ClearanceDocument1 pageIneffective Airway Clearancerozj0750% (2)
- NCP of MGH PatientDocument2 pagesNCP of MGH PatientMaverick LimNo ratings yet
- NCP DobDocument3 pagesNCP DobLester BuhayNo ratings yet
- Pneumonia Nursing Care Plans in 40 CharactersDocument1 pagePneumonia Nursing Care Plans in 40 Charactersjustin_saneNo ratings yet
- NCP Ineffective Airway ClearanceDocument4 pagesNCP Ineffective Airway ClearanceMary Joyce Limoico100% (1)
- Caring for an Elderly Patient with DepressionDocument2 pagesCaring for an Elderly Patient with DepressionSheryl Ann Barit PedinesNo ratings yet
- Nursing Care Plan Ineffective Airway Clearance Related To Tracheobronchial Secretions CAPDocument2 pagesNursing Care Plan Ineffective Airway Clearance Related To Tracheobronchial Secretions CAPLP Benoza100% (2)
- Ineffective Airway ClearanceDocument2 pagesIneffective Airway ClearancepsengsonNo ratings yet
- Respiratory Care: Ronald P. Mlcak, Oscar E. Suman, Linda E. Sousse, and David N. HerndonDocument12 pagesRespiratory Care: Ronald P. Mlcak, Oscar E. Suman, Linda E. Sousse, and David N. HerndonDavid ReyesNo ratings yet
- Abstrak 090014.id - enDocument1 pageAbstrak 090014.id - enIna OrengNo ratings yet
- Ineffective Airway ClearanceDocument10 pagesIneffective Airway ClearanceHannah VueltaNo ratings yet
- Nursing ManagementDocument16 pagesNursing ManagementNica Marie LumbaNo ratings yet
- Chest Physiotherapy and Other Pulmonary Treatment ModalitiesDocument9 pagesChest Physiotherapy and Other Pulmonary Treatment ModalitiesJayferson SalesNo ratings yet
- Nursing Management of Clients With COPD: - Initiate Infusion of Intravenous Antibiotic As PrescribedDocument3 pagesNursing Management of Clients With COPD: - Initiate Infusion of Intravenous Antibiotic As PrescribedNiña AngNo ratings yet
- 2 NCPDocument2 pages2 NCPJohn CenasNo ratings yet
- Demonstration On Chest Physiotherapy DefinitionDocument3 pagesDemonstration On Chest Physiotherapy Definitiondileep0% (1)
- Nursing Care Plan 2Document1 pageNursing Care Plan 2JOYCE ANNE SUERTE DAGDAGANNo ratings yet
- 11 Mechanical Ventilation & Endotracheal Intubation Nursing Care Plans and Management - NurseslabsDocument55 pages11 Mechanical Ventilation & Endotracheal Intubation Nursing Care Plans and Management - NurseslabsCarissa EstradaNo ratings yet
- Dyspnea and NebulizationDocument42 pagesDyspnea and NebulizationHema AnkamreddyNo ratings yet
- Wk2 NCP Edited2012Document6 pagesWk2 NCP Edited2012Jessely Caling SalasNo ratings yet
- Effective Airway Clearance Nursing DiagnosisDocument30 pagesEffective Airway Clearance Nursing DiagnosisReadcast EFNo ratings yet
- Laboratory ValuesDocument2 pagesLaboratory ValuesCarmela Mabel Ansay PrincipeNo ratings yet
- Laboratory ValuesDocument2 pagesLaboratory ValuesCarmela Mabel Ansay PrincipeNo ratings yet
- Essential Newborn CareDocument1 pageEssential Newborn CareCarmela Mabel Ansay PrincipeNo ratings yet
- Normal VSDocument1 pageNormal VSCarmela Mabel Ansay PrincipeNo ratings yet
- Procedure Sick Bay 2017Document6 pagesProcedure Sick Bay 2017Syed FareedNo ratings yet
- Chapter 39 - Assessment and Management of Patients With Hepatic DisordersDocument6 pagesChapter 39 - Assessment and Management of Patients With Hepatic DisordersMichael BoadoNo ratings yet
- Daftar PustakaDocument9 pagesDaftar Pustakaaajeng ftnyNo ratings yet
- Essay Ingles 2Document3 pagesEssay Ingles 2Javi LiuNo ratings yet
- 2021 Article 2922Document4 pages2021 Article 2922AnirisulNo ratings yet
- Ambulance ServiceDocument9 pagesAmbulance ServicedennymxNo ratings yet
- Notice To Kettle Falls SDDocument2 pagesNotice To Kettle Falls SDErin RobinsonNo ratings yet
- Katie's story of recovery from anorexiaDocument8 pagesKatie's story of recovery from anorexiaAinjhel CalaraNo ratings yet
- CPD Book and Patient PictureDocument6 pagesCPD Book and Patient PicturePriyaNo ratings yet
- Burn WoundsDocument14 pagesBurn WoundsRuxandra BadiuNo ratings yet
- Skeletal Muscle Relaxants and Neuromuscular Blocking AgentsDocument7 pagesSkeletal Muscle Relaxants and Neuromuscular Blocking AgentsYanyan PanesNo ratings yet
- SOP For Ground Crossing On Covid-19Document6 pagesSOP For Ground Crossing On Covid-19Bheru LalNo ratings yet
- Eric Thorhauer CVDocument7 pagesEric Thorhauer CVapi-251923314No ratings yet
- WSO Global Stroke Fact SheetDocument15 pagesWSO Global Stroke Fact SheetPentolNo ratings yet
- Diane Pills Drug StudyDocument4 pagesDiane Pills Drug StudyDawn EncarnacionNo ratings yet
- 1 Laporan Pengeluaran Obat Dan Alkes Depyan 28 SEPTEMBER 2019Document18 pages1 Laporan Pengeluaran Obat Dan Alkes Depyan 28 SEPTEMBER 2019Indah SetyowatiNo ratings yet
- Manual Surgical Safety Checklist 1st EditionDocument28 pagesManual Surgical Safety Checklist 1st EditionJuandri Pia TorocozzickNo ratings yet
- HIV 12 Stat Pak Dipstick Product Packet EnglishDocument6 pagesHIV 12 Stat Pak Dipstick Product Packet EnglishSagkyNo ratings yet
- 香港脊醫 Hong Kong Chiropractors May 2018Document18 pages香港脊醫 Hong Kong Chiropractors May 2018CDAHKNo ratings yet
- Health HistoryDocument4 pagesHealth Historyapi-454903860No ratings yet
- BANSUANRDRECORDDocument4 pagesBANSUANRDRECORDclint xavier odangoNo ratings yet
- 214 Dominican Republic Fact SheetDocument2 pages214 Dominican Republic Fact Sheetfedemoncada89No ratings yet
- 22 PciDocument19 pages22 PciSoham MAITYNo ratings yet
- Nurse'S Notes: Date-Shift Focus Data - Action - ResponseDocument5 pagesNurse'S Notes: Date-Shift Focus Data - Action - ResponseRenea Joy ArruejoNo ratings yet