You might also like
- EKG and ECG Interpretation: Learn EKG Interpretation, Rhythms, and Arrhythmia Fast!From EverandEKG and ECG Interpretation: Learn EKG Interpretation, Rhythms, and Arrhythmia Fast!No ratings yet
- ECG & EKG Interpretation: How to interpret ECG & EKG, including rhythms, arrhythmias, and more!From EverandECG & EKG Interpretation: How to interpret ECG & EKG, including rhythms, arrhythmias, and more!No ratings yet
- The 12-Lead Electrocardiogram for Nurses and Allied ProfessionalsFrom EverandThe 12-Lead Electrocardiogram for Nurses and Allied ProfessionalsNo ratings yet
- ECG/EKG Interpretation: An Easy Approach to Read a 12-Lead ECG and How to Diagnose and Treat ArrhythmiasFrom EverandECG/EKG Interpretation: An Easy Approach to Read a 12-Lead ECG and How to Diagnose and Treat ArrhythmiasRating: 5 out of 5 stars5/5 (2)
- EKG | ECG: An Ultimate Step-By-Step Guide to 12-Lead EKG | ECG Interpretation, Rhythms & Arrhythmias Including Basic Cardiac DysrhythmiasFrom EverandEKG | ECG: An Ultimate Step-By-Step Guide to 12-Lead EKG | ECG Interpretation, Rhythms & Arrhythmias Including Basic Cardiac DysrhythmiasRating: 3 out of 5 stars3/5 (5)
- EKG | ECG Interpretation. Everything You Need to Know about 12-Lead ECG/EKG InterpretationFrom EverandEKG | ECG Interpretation. Everything You Need to Know about 12-Lead ECG/EKG InterpretationRating: 3 out of 5 stars3/5 (1)
- Torsade De Pointes, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandTorsade De Pointes, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- EKG Interpretation Basics Guide: Electrocardiogram Heart Rate Determination, Arrhythmia, Cardiac Dysrhythmia, Heart Block Causes, Symptoms, Identification and Medical Treatment Nursing HandbookFrom EverandEKG Interpretation Basics Guide: Electrocardiogram Heart Rate Determination, Arrhythmia, Cardiac Dysrhythmia, Heart Block Causes, Symptoms, Identification and Medical Treatment Nursing HandbookNo ratings yet
- A Simple Guide to the Heart beats, Related Diseases And Use in Disease DiagnosisFrom EverandA Simple Guide to the Heart beats, Related Diseases And Use in Disease DiagnosisRating: 5 out of 5 stars5/5 (1)
- Basic Arrhythmia RulesDocument3 pagesBasic Arrhythmia Rulesgreenflames0997% (30)
- Cardiac DysrhythmiasDocument3 pagesCardiac DysrhythmiasKatherine Santiago92% (62)
- A Simplified ECG GuideDocument4 pagesA Simplified ECG Guidejalan_z96% (27)
- EKG ExamplesDocument9 pagesEKG ExamplesMayer Rosenberg99% (235)
- May/No P: Inverted/B/ A Qrs P (Befor e QRS) - 0.12Document3 pagesMay/No P: Inverted/B/ A Qrs P (Befor e QRS) - 0.12is_aradanas0% (1)
- Cardiac Dysrhythmia Chart Med-Surg NUR4Document3 pagesCardiac Dysrhythmia Chart Med-Surg NUR4ktfosterfd2096% (97)
- Cardiac Study GuideDocument11 pagesCardiac Study Guidejenwiley318096% (73)
- Dysrhythmias ChartDocument6 pagesDysrhythmias Chartjkrix100% (1)
- EKG Flash CardsDocument5 pagesEKG Flash CardsRyann Sampino FreitasNo ratings yet
- Ecg Cheat Sheet 35Document2 pagesEcg Cheat Sheet 35jessjaylee80% (5)
- ECG Interpretation Cheat SheetDocument1 pageECG Interpretation Cheat Sheethirsi20051879% (24)
- EKG Cheat SheetDocument9 pagesEKG Cheat SheetAlert Twitter100% (5)
- Cardiac DrugsDocument10 pagesCardiac DrugsNursePoor98% (48)
- EKG Practice TestDocument16 pagesEKG Practice TestAbdul Rohim100% (1)
- Ekg Strip NotesDocument13 pagesEkg Strip NotesNick Loizzo100% (2)
- Reading A EKGDocument10 pagesReading A EKGMayer Rosenberg100% (15)
- Acid-Base WorksheetDocument2 pagesAcid-Base WorksheetMayer Rosenberg100% (18)
- Lab ValuesDocument3 pagesLab Valuessurviving nursing school100% (1)
- Basic EKG ECG Rhythms CheatsheetDocument1 pageBasic EKG ECG Rhythms CheatsheetAhmad83% (6)
- ACLS EKG Rhythms and InterpretationDocument10 pagesACLS EKG Rhythms and Interpretationdonheyzz_02No ratings yet
- Ekg PracticeDocument7 pagesEkg PracticeMichelle Cobb Matthews100% (1)
- Cardiac Meds ChartDocument1 pageCardiac Meds ChartCharlotte Louise75% (4)
- Basic EKG For DummiesDocument133 pagesBasic EKG For Dummieseduardocmoura86% (7)
- Quick Ekg ReferenceDocument23 pagesQuick Ekg Referencekowaikowar100% (2)
- Ekg Made EasyDocument7 pagesEkg Made Easystring44100% (3)
- Ecg Reading NotesDocument17 pagesEcg Reading NotesMarian FloresNo ratings yet
- Cardiac Dysrhythmia Chart Med Surg NUR4 PDFDocument3 pagesCardiac Dysrhythmia Chart Med Surg NUR4 PDFlml100% (1)
- EKG Pocket GuideDocument2 pagesEKG Pocket GuideFabian Ramirez HincapiéNo ratings yet
- Common Cardiac MedicationsDocument1 pageCommon Cardiac MedicationsPaige HardekopfNo ratings yet
- Jane Huff ECG Workout Exercises in Arrhythmia Interpretation 2011Document419 pagesJane Huff ECG Workout Exercises in Arrhythmia Interpretation 2011BiancaPancu90% (40)
- Inherent Rates: Cardiovascular System Alterations Module BDocument7 pagesInherent Rates: Cardiovascular System Alterations Module Bmp_329No ratings yet
- Wolff-Parkinson- White-Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandWolff-Parkinson- White-Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- EKG/ECG Interpretation Made Easy: A Practical Approach to Passing the ECG/EKG Portion of NCLEXFrom EverandEKG/ECG Interpretation Made Easy: A Practical Approach to Passing the ECG/EKG Portion of NCLEXRating: 5 out of 5 stars5/5 (2)
- Advance Cardiac Life Support: Short, Sweet and to the PointFrom EverandAdvance Cardiac Life Support: Short, Sweet and to the PointRating: 3 out of 5 stars3/5 (2)
- Bonehead Electrocardiography: The Easiest and Best Way to Learn How to Read Electrocardiograms—No Bones About It!From EverandBonehead Electrocardiography: The Easiest and Best Way to Learn How to Read Electrocardiograms—No Bones About It!Rating: 5 out of 5 stars5/5 (2)
- Haemodynamic Monitoring & Manipulation: an easy learning guideFrom EverandHaemodynamic Monitoring & Manipulation: an easy learning guideNo ratings yet
- Surviving the ICU: A Toolkit for the Critical Care NurseFrom EverandSurviving the ICU: A Toolkit for the Critical Care NurseNo ratings yet
- Ccrn Certification Examination Practice Questions and Answers with Rationale: First EditionFrom EverandCcrn Certification Examination Practice Questions and Answers with Rationale: First EditionRating: 5 out of 5 stars5/5 (1)
- Corazon - LecturioDocument33 pagesCorazon - LecturioFatima GiulianaNo ratings yet
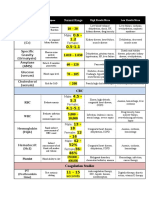
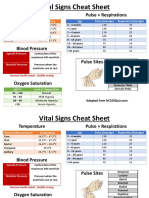
- Temperature Pulse + RespirationsDocument2 pagesTemperature Pulse + RespirationsMarshin Thea Celocia100% (1)
- Anatomy and Physiology AnswersDocument11 pagesAnatomy and Physiology AnswersKojo Yeboah EnchillNo ratings yet
- Ascites in Broiler ChickensDocument3 pagesAscites in Broiler ChickensDr.Kedar Karki ,M.V.Sc.Preventive Vet.Medicine CLSU Philippines100% (1)
- EmbolismDocument13 pagesEmbolismSandeep Bansal100% (1)
- Stroke Pathophysiology 1Document5 pagesStroke Pathophysiology 1Jeco ValdezNo ratings yet
- Electrocar Diogram: College of Nursing Madurai Medical College, Madurai-20 Procedure Demonstration OnDocument19 pagesElectrocar Diogram: College of Nursing Madurai Medical College, Madurai-20 Procedure Demonstration OnValarmathi100% (1)
- Cardiovascular SystemDocument40 pagesCardiovascular SystemMudasir Hussain TuriNo ratings yet
- Biology C - Lesson 1 - Circulatory SystemDocument47 pagesBiology C - Lesson 1 - Circulatory SystemMary Jewel0% (1)
- The Heart - Print - QuizizzDocument5 pagesThe Heart - Print - Quizizzosama100% (1)
- Cardiac Catheterization and MonitoringDocument40 pagesCardiac Catheterization and MonitoringMarissa Asim100% (1)
- Brosur Ecatalog Cosmo 2019 - V2Document19 pagesBrosur Ecatalog Cosmo 2019 - V2pku wonosoboNo ratings yet
- Lab 2jhghgdfgxzDocument47 pagesLab 2jhghgdfgxzanaNo ratings yet
- Coronary Artery DiseaseDocument3 pagesCoronary Artery DiseaseMarta Luquez RNo ratings yet
- VHD Guidelines Slide Set GL VHDDocument220 pagesVHD Guidelines Slide Set GL VHDNASERZALLOUMNo ratings yet
- The Intra-Aortic Balloon Pump (IABP) - An Essential Component of Modern Cardiac CareDocument1 pageThe Intra-Aortic Balloon Pump (IABP) - An Essential Component of Modern Cardiac CareNavojit ChowdhuryNo ratings yet
- Chapter 14. Patient Clinical EvaluationDocument13 pagesChapter 14. Patient Clinical Evaluationedwinp21No ratings yet
- ABSITE CH 16 Critical CareDocument11 pagesABSITE CH 16 Critical CareJames JosephNo ratings yet
- CASE PRESentationDocument30 pagesCASE PRESentationllanelli.graciaNo ratings yet
- The Easy R's EKG Interpretation FinalDocument9 pagesThe Easy R's EKG Interpretation FinalMatar PaneerNo ratings yet
- BplogDocument2 pagesBplogMonir AhamedNo ratings yet
- Fetal CirculationDocument15 pagesFetal CirculationPujani SenevirathnaNo ratings yet
- Immune SystemDocument21 pagesImmune SystemAbdullah KhanNo ratings yet
- 2012 EO2 Student HB v1.0Document78 pages2012 EO2 Student HB v1.0Ariane HoffmannNo ratings yet
- Nursing Care PlanDocument19 pagesNursing Care PlanChic Dian UsmanNo ratings yet
- 3D Transthoracic Echocardiography Provides Accurate Cross-Sectional Area of The RV Outflow Tract - 1Document3 pages3D Transthoracic Echocardiography Provides Accurate Cross-Sectional Area of The RV Outflow Tract - 1Thumper KatesNo ratings yet
- Conclusion Question 4Document2 pagesConclusion Question 4api-376088598No ratings yet
- Scientifically Proven Reading Comprehension StrategiesDocument12 pagesScientifically Proven Reading Comprehension StrategiesBrittney AnnNo ratings yet
- Tetralogy of FallotDocument31 pagesTetralogy of FallotDevipriya MajumderNo ratings yet
- 0610 s12 Ms 32 PDFDocument10 pages0610 s12 Ms 32 PDFNyantuy. MieNo ratings yet