You might also like
- An Assignment ON: Bronchial HygieneDocument12 pagesAn Assignment ON: Bronchial Hygienesoniya joseph100% (1)
- Pulmonary Rehabilitation: Nyimas FatimahDocument61 pagesPulmonary Rehabilitation: Nyimas FatimahNur akilaNo ratings yet
- Noncardiogenic Pulmonary EdemaDocument12 pagesNoncardiogenic Pulmonary EdemaIrina DuceacNo ratings yet
- Recent TB Treatment GuidelinesDocument28 pagesRecent TB Treatment GuidelinesDr venkatesh jalluNo ratings yet
- Arterial Line Arterial LineDocument13 pagesArterial Line Arterial LineLinamaria Lozano100% (1)
- B M W M: IO Edical Aste AnagementDocument23 pagesB M W M: IO Edical Aste AnagementJishnu JohnNo ratings yet
- Icu Initial Ventilator SettingsDocument40 pagesIcu Initial Ventilator SettingsantreaspetsasNo ratings yet
- Abdominal Aortic Aneurysmn FINAL WORDDocument16 pagesAbdominal Aortic Aneurysmn FINAL WORDErica P. ManlunasNo ratings yet
- Epid COPDDocument9 pagesEpid COPDAgung WistaraNo ratings yet
- Health Care EconomicsDocument30 pagesHealth Care EconomicsGopika SNo ratings yet
- Critically Ill PatientDocument31 pagesCritically Ill PatientSameh Aziz100% (1)
- Spinal TuberculosisDocument46 pagesSpinal TuberculosisAbby Austero100% (1)
- Care of Patient With TPM Slide PresentationDocument16 pagesCare of Patient With TPM Slide PresentationirzehronNo ratings yet
- Intercostal DrainageDocument39 pagesIntercostal DrainagePutri AdiratnaNo ratings yet
- Mechanical VentilationDocument40 pagesMechanical VentilationPratik SahooNo ratings yet
- Thoracic SurgeryDocument16 pagesThoracic SurgeryNicole Shannon CariñoNo ratings yet
- Cardiovascular and Thoracic NursingDocument4 pagesCardiovascular and Thoracic NursingShreyas Walvekar100% (1)
- Suctioning Artificial Airways - AdultsDocument27 pagesSuctioning Artificial Airways - AdultssdaNo ratings yet
- Jabalpur (M.P.) : Subject - Management Nursing Assignment ONDocument9 pagesJabalpur (M.P.) : Subject - Management Nursing Assignment ONNikkiNo ratings yet
- 2 5 17 991Document6 pages2 5 17 991Science JournalNo ratings yet
- Cabg Case Study FormDocument9 pagesCabg Case Study FormVlad ConstantinNo ratings yet
- Reference Writing Styles: Mrs. Monika Sharma Lecturer, DMCH, CON, Ludhiana. PunjabDocument82 pagesReference Writing Styles: Mrs. Monika Sharma Lecturer, DMCH, CON, Ludhiana. PunjabNavpreet KaurNo ratings yet
- 02 AmputationDocument23 pages02 AmputationJuanitoCabatañaLimIIINo ratings yet
- Ards PDFDocument2 pagesArds PDFgireeshsachinNo ratings yet
- Prognosis MGDocument7 pagesPrognosis MGPutri Cindy Claudia PandoyoNo ratings yet
- Critical Care Update PDFDocument25 pagesCritical Care Update PDFHugo PozoNo ratings yet
- Lung AuscultationDocument62 pagesLung AuscultationOlea CroitorNo ratings yet
- Respiratory Arrest and InsufficiencyDocument6 pagesRespiratory Arrest and InsufficiencyGetom Ngukir100% (1)
- Research Synopsis FormatDocument13 pagesResearch Synopsis Formatmaya vermaNo ratings yet
- Deep Vein Thrombosis & Its ProphylaxisDocument90 pagesDeep Vein Thrombosis & Its ProphylaxisPratik KumarNo ratings yet
- Management Acute StrokeDocument108 pagesManagement Acute StrokeratuhamimNo ratings yet
- Intermittent Positive Pressure BreathingDocument12 pagesIntermittent Positive Pressure BreathingHitesh RohitNo ratings yet
- Ventricular Septal DefectsDocument7 pagesVentricular Septal DefectsMuhammadAldoGiansyahNo ratings yet
- 13.knowledge and Practices of Universal Precautions Among Basic B. Sc. Nursing StudentsDocument10 pages13.knowledge and Practices of Universal Precautions Among Basic B. Sc. Nursing StudentsPutri Alin Kende RiaralyNo ratings yet
- Rajiv Gandhi University of Health Sciences, Bangalore, KarnatakaDocument34 pagesRajiv Gandhi University of Health Sciences, Bangalore, KarnatakaYayu AlawiiahNo ratings yet
- Assignment ON: S.G.R.D Institute of Nursing, Pandger, (Asr)Document4 pagesAssignment ON: S.G.R.D Institute of Nursing, Pandger, (Asr)Charan0% (1)
- IntroductionDocument13 pagesIntroductionSiyara AntonyNo ratings yet
- AARC Clinical Practice Guideline: Incentive SpirometryDocument10 pagesAARC Clinical Practice Guideline: Incentive SpirometrytruptimptNo ratings yet
- Empyema 171013100219Document23 pagesEmpyema 171013100219Mahmoud Abdel MoneimNo ratings yet
- Scope of Critical Care Practice: Study GuideDocument6 pagesScope of Critical Care Practice: Study GuideDan Dan ManaoisNo ratings yet
- Rhemuatoid Arthritis: Post RN BSN 1 Semester JCON Pushpa Kumari Abdul Hafeez Raza Muhammad Ghulam Murtaza 20/11/2020Document19 pagesRhemuatoid Arthritis: Post RN BSN 1 Semester JCON Pushpa Kumari Abdul Hafeez Raza Muhammad Ghulam Murtaza 20/11/2020shewo.pirtamNo ratings yet
- Thyroid CrisisDocument11 pagesThyroid CrisisKoka KolaNo ratings yet
- What Is ICU PsychosisDocument6 pagesWhat Is ICU PsychosisAngelicaMarieRafananNo ratings yet
- Code of EthicsDocument5 pagesCode of EthicspvlreyesNo ratings yet
- Diagnostic Thoracoscopy (VATS) in Lung CancerDocument18 pagesDiagnostic Thoracoscopy (VATS) in Lung CancerlmdarlongNo ratings yet
- Innovations in Nursing: Name: InstructorDocument5 pagesInnovations in Nursing: Name: InstructorAlex MunyaoNo ratings yet
- Research Proposal Outline (PHD)Document3 pagesResearch Proposal Outline (PHD)nadia azriNo ratings yet
- Cerebral Venous ThrombosisDocument15 pagesCerebral Venous ThrombosisValentina RobuNo ratings yet
- Treadmill Test: Khairul Nizam Abdul Rahman 4262143008Document12 pagesTreadmill Test: Khairul Nizam Abdul Rahman 4262143008Dea Amelia YolandaNo ratings yet
- Assignment ON: Writing The Reference and BibliographyDocument8 pagesAssignment ON: Writing The Reference and BibliographyAru VermaNo ratings yet
- A Pre Experimental Study To Assess The EDocument6 pagesA Pre Experimental Study To Assess The ERAMKESH DIWAKARNo ratings yet
- Icu PsychosisDocument23 pagesIcu PsychosisJisha JanardhanNo ratings yet
- Coronary Artery Bypass Grafting (Cabg) :: Case Study ReportDocument83 pagesCoronary Artery Bypass Grafting (Cabg) :: Case Study ReportSherena NicolasNo ratings yet
- ACLS II Sept 25 StudentsDocument60 pagesACLS II Sept 25 StudentsLex CatNo ratings yet
- EmpyemaDocument107 pagesEmpyemaNITHA KNo ratings yet
- Modes of Mechanical VentilationDocument4 pagesModes of Mechanical Ventilationsgod34100% (1)
- Disorders of AortaDocument25 pagesDisorders of Aortavani reddyNo ratings yet
- Warning Signs of Various DiseasesDocument44 pagesWarning Signs of Various DiseasesamsabavanNo ratings yet
- Small Pox (CHN)Document13 pagesSmall Pox (CHN)Getom NgukirNo ratings yet
- Management of Tuberculosis: A guide for clinicians (eBook edition)From EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)No ratings yet
- Name of DrugDocument6 pagesName of Drug私 シャーロット100% (1)
- This Refers To The Manner in Which Nursing Care Is Organized and ProvidedDocument3 pagesThis Refers To The Manner in Which Nursing Care Is Organized and Provided私 シャーロットNo ratings yet
- Tic Doulourex Nursing ManagementDocument1 pageTic Doulourex Nursing Management私 シャーロットNo ratings yet
- Tic DoulourexDocument6 pagesTic Doulourex私 シャーロットNo ratings yet
- Arterial Lines Mark Hammerschmidt, RN FromDocument9 pagesArterial Lines Mark Hammerschmidt, RN FromMark Hammerschmidt100% (3)
- Pulmonary Arterial Pressure TestingDocument22 pagesPulmonary Arterial Pressure Testingeven24No ratings yet
- Ccu First Quiz FinalDocument4 pagesCcu First Quiz FinalEggy PascualNo ratings yet
- Physics of Blood FlowDocument15 pagesPhysics of Blood FlowNahidNo ratings yet
- Compare The Pulmonary and Systemic Circuits of The Cardiovascular SystemDocument6 pagesCompare The Pulmonary and Systemic Circuits of The Cardiovascular Systememanuel coatesNo ratings yet
- Circulatory WksDocument6 pagesCirculatory WksPak RisNo ratings yet
- Pre-Board Papers With MS ScienceDocument323 pagesPre-Board Papers With MS Scienceayishasamath08No ratings yet
- MCQ HemodynamicsDocument2 pagesMCQ HemodynamicsKehkashan Khan80% (5)
- Corazón DerechoDocument326 pagesCorazón DerechoCristianAltunaSotomayorNo ratings yet
- Atherosclerosis: Wen Wen, Rong Luo, Xiaojing Tang, Lan Tang, Hunter X. Huang, Xiaoyan Wen, Shan Hu, Bin PengDocument6 pagesAtherosclerosis: Wen Wen, Rong Luo, Xiaojing Tang, Lan Tang, Hunter X. Huang, Xiaoyan Wen, Shan Hu, Bin PengmerawatidyahsepitaNo ratings yet
- CARDIOVASCULAR - SYSTEM Group No.3 MODULEDocument12 pagesCARDIOVASCULAR - SYSTEM Group No.3 MODULEDavid Paul LanuzaNo ratings yet
- EAWS AviationDocument72 pagesEAWS AviationcameldiverNo ratings yet
- Arterial Line Analysis PresentationDocument35 pagesArterial Line Analysis PresentationLisa GilbertNo ratings yet
- Nephrolithotomy To Nephrectomy: A Rare Case in The Field of Philippine-Based SurgeriesDocument58 pagesNephrolithotomy To Nephrectomy: A Rare Case in The Field of Philippine-Based SurgeriesGiuseppe Carlo LaranangNo ratings yet
- Stroke PreventionDocument3 pagesStroke Preventionapi-27015740100% (2)
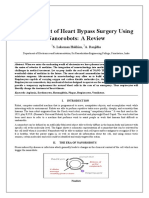
- Nanorobots The Heart SurgeonDocument7 pagesNanorobots The Heart SurgeonPoonguzhali MadhavanNo ratings yet
- Science 9Document3 pagesScience 9maria weleen largoNo ratings yet
- Sijil Tinggi Persekolahan Malaysia EditDocument75 pagesSijil Tinggi Persekolahan Malaysia EditDiana Ana0% (2)
- Medical Terminology 2 Cardiovascular System Lesson 1Document3 pagesMedical Terminology 2 Cardiovascular System Lesson 1sotman58No ratings yet
- Case StudyDocument41 pagesCase StudychaSeph292784100% (6)
- Myocardial InfarctionDocument15 pagesMyocardial Infarctionanon_877280340No ratings yet
- 6 - BLS HandoutDocument18 pages6 - BLS HandoutEastern SamarNo ratings yet
- L. A. Geddes ME, PHD Auth. Handbook of Blood Pressure MeasurementDocument171 pagesL. A. Geddes ME, PHD Auth. Handbook of Blood Pressure MeasurementYashNo ratings yet
- Physical Education Teacher 634 C 491 Set ADocument24 pagesPhysical Education Teacher 634 C 491 Set AManjit singhNo ratings yet
- Biology TermsDocument17 pagesBiology TermsSaidatul Atyah Mohd ApendaiNo ratings yet
- Ticket 1Document12 pagesTicket 1malihah qaziNo ratings yet
- Heart MurmursDocument7 pagesHeart MurmursOffvb MednuNo ratings yet
- B. Pathophysiology A) Schematic Diagram (Book - Based) : Wasting Blood Glucose LevelDocument2 pagesB. Pathophysiology A) Schematic Diagram (Book - Based) : Wasting Blood Glucose LevelCarl Elexer Cuyugan Ano50% (2)
- 10th Biology Term-01 Chapter Life Process e NotesDocument16 pages10th Biology Term-01 Chapter Life Process e NotesMichael LewisNo ratings yet
- Global Atlas About CV Disease by WHODocument164 pagesGlobal Atlas About CV Disease by WHOLouisette AgapeNo ratings yet