Professional Documents
Culture Documents
Demicheli Et Al - 2000 - Prevention and Early Treatment of Influenza in Healthy Adults
Uploaded by
Михаил РайцисOriginal Description:
Original Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Demicheli Et Al - 2000 - Prevention and Early Treatment of Influenza in Healthy Adults
Uploaded by
Михаил РайцисCopyright:
Available Formats
Vaccine 18 (2000) 9571030
www.elsevier.com/locate/vaccine
Review
Prevention and early treatment of inuenza in healthy adults
V. Demicheli a, T. Jeerson b,*, D. Rivetti c, J. Deeks d
b a Institute of Medical Statistics, University of Pavia, Pavia, Italy Cochrane Centre and Cochrane Vaccines Field, Summertown Pavillion, Middle Way, Oxford OX2 7LG, UK c Environmental Epidemiology Unit, ARPA, Alessandria, Italy d Systematic Reviews Unit, Institute of Health Sciences, Oxford, UK
Received 27 January 1999; received in revised form 20 June 1999; accepted 14 July 1999
Abstract Introduction: We present three systematic reviews carried out within the Cochrane Collaboration, focusing on a dierent inuenza intervention in healthy adults: Vaccines; Ion Channel Inhibitor antivirals and Neuraminidase Inhibitor (NIs) antivirals. The objectives were to identify, retrieve and assess all studies evaluating the eects of these interventions in prophylaxis and early treatments of inuenza and the frequency of adverse events. Additionally we present the results of the economic evaluation of eective alternatives in order to dene the most cost-eective intervention. The economic evaluation is set in the context of the British Army. Methods: Studies were identied using a standard Cochrane search strategy. Any randomised or quasi-randomised studies in healthy individuals aged 1460 years were considered for inclusion in the systematic review. Those which met inclusion criteria were assessed for quality and their data meta-analysed. The economic model was constructed using Cost-eectiveness and Costutility study designs. Results: Live aerosol vaccines reduced cases of clinical inuenza A with virological conrmation (by serology and/or viral isolation) by 48% (95%CI: 2464%), whilst recommended inactivated parenteral vaccines have an ecacy of 68% (95%CI: 49 79%). Vaccine eectiveness in reducing clinical inuenza cases (i.e. without virological conrmation) was lower, with ecacies of 13 and 24% respectively. Use of the vaccine signicantly reduced time o work, but only by 0.4 days (95%CI: 0.10.8 days). Analysis of vaccines matching the circulating strain gave higher estimates of ecacy, whilst inclusion of all other vaccines reduced the ecacy. When compared to placebo for the prevention of inuenza, oral amantadine was 61% (95%CI: 5169%) ecacious (RR 0.39 95%CI: 0.310.49), and oral rimantadine was 64% (95%CI: 4178%) ecacious (RR 0.36 95%CI: 0.220.59). When compared to placebo for the treatment of inuenza, oral amantadine signicantly shortened duration of fever (by 1.00 days 95%CI: 0.731.29), and oral rimantadine signicantly shortened duration of fever (by 1.27 days 95%CI: 0.771.77). When compared to placebo, NIs were 74% (95%CIs: 5087%) eective in preventing naturally occurring cases of clinically dened inuenza. In a treatment role, NIs shortened the duration of symptoms by one day (Weighted Mean Dierence 1.0; 95%CIs: 1.3 to 0.6) when a clinical case denition is used. The economic results show that in healthy adults, inactivated vaccines appear the best buy. Conclusions: If assessed from the point of view of eectiveness and eciency, vaccines are undoubtedly the best preventive means for clinical inuenza in healthy adults. However, when safety and quality of life considerations are included, parenteral vaccines have such low eectiveness and high incidence of trivial local adverse eects that the trade-o is unfavourable. This is so even when the incidence of inuenza is high and adverse eect quality of life preferences are rated low. We reached similar conclusions for antivirals and NIs even at high inuenza incidence levels. On current evidence we conclude in healthy adults aged 1460 the most cost-eective option is not to take any action. # 2000 Elsevier Science Ltd. All rights reserved.
* Corresponding author. Tel.: +44-1865-516300; fax: +44-1865516311. E-mail address: toj1@aol.com (T. Jeerson). 0264-410X/00/$ - see front matter # 2000 Elsevier Science Ltd. All rights reserved. PII: S 0 2 6 4 - 4 1 0 X ( 0 0 ) 0 0 3 3 2 - 1
958
V. Demicheli et al. / Vaccine 18 (2000) 9571030
Contents 1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1.1. Prevention and early treatment of inuenza . . . . . . . . . . . . . . . . . . . . . 1.1.1. Inuenza vaccines . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1.1.2. Ion channel inhibitor antivirals (Amantadine and Rimantadine) 1.1.3. Neuraminidase inhibitor antivirals (NIs) . . . . . . . . . . . . . . . . . 1.2. Rationale for the economic evaluation . . . . . . . . . . . . . . . . . . . . . . . . Methods . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2.1. Methods for the reviews. . . . . . . . . . . . . . . . . 2.1.1. Objectives. . . . . . . . . . . . . . . . . . . . . 2.1.2. Selection criteria . . . . . . . . . . . . . . . . 2.1.3. Search strategy . . . . . . . . . . . . . . . . . 2.1.4. Methods for the economic evaluation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 959 959 959 961 962 962 963 963 963 963 963 966 967 967 967 970 971 971 971 971 972 972 972 974 974 975 975 976 976 977 977 977 979 979 979 981 982 982 982
2.
3.
Results . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3.1. Results of the reviews . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3.1.1. Description of studies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3.1.2. Methodological quality of included studies . . . . . . . . . . . . . . . . . . . . . . . . . 3.2. Eects of inuenza vaccines . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3.2.1. Eect of vaccination on clinical cases of inuenza . . . . . . . . . . . . . . . . . . . . 3.2.2. Eect of vaccination on serologically conrmed cases of inuenza . . . . . . . . 3.2.3. Eect of vaccination on other outcomes . . . . . . . . . . . . . . . . . . . . . . . . . . . 3.2.4. Recommended vaccines . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3.2.5. Vaccine matching the circulating strain . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3.3. Eects of amantadine and rimantadine . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3.3.1. Comparison A oral amantadine compared to placebo in inuenza prevention . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3.3.2. Comparison B oral rimantadine compared to placebo in inuenza prevention . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3.3.3. Comparison C oral amantadine compared to oral rimantadine in inuenza prevention . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3.3.4. Comparison D oral amantadine compared to placebo in inuenza treatment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3.3.5. Comparison E oral rimantadine compared to placebo in inuenza treatment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3.3.6. Comparison F oral amantadine compared to oral rimantadine in inuenza treatment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3.3.7. Comparison G oral amantadine compared to oral aspirin in inuenza treatment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3.3.8. Comparison H inhaled amantadine compared to placebo in inuenza treatment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3.4. Eects of NIs . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3.5. Results of the economic evaluation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Discussion . . . . . . . . . . . . . . . . . . . 4.1. Inuenza vaccines . . . . . . . . . 4.2. Amantadine and rimantadine . 4.3. Neuraminidase inhibitors . . . . 4.4. Overall comments . . . . . . . . . 4.5. Economic evaluation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
4.
Acknowledgements . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 983 Appendix A . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 984 Appendix B . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 985 Appendix C . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 986 References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1030
V. Demicheli et al. / Vaccine 18 (2000) 9571030
959
1. Introduction Inuenza is an acute respiratory infection caused by a virus, of which three serotypes are known (A, B and C). Inuenza causes an acute febrile illness with myalgia, headache and cough. Although the median duration of the acute illness is three days (duration can vary between serotypes and subtypes), cough and malaise can persist for weeks. Complications of inuenza include otitis media, pneumonia, secondary bacterial pneumonia, exacerbations of chronic respiratory disease and bronchiolitis in children. Additionally, inuenza can cause a range of non-respiratory complications including febrile convulsions, Reye's syndrome and myocarditis [1]. The inuenza virus is composed of a lipid membrane surrounding a protein shell and a core consisting of several RNA complexes. On the lipid membrane are two viral glycoproteins which act as powerful antigens: neuraminidase (N antigen) and hemagglutinin (H antigen). Hemagglutinin facilitates the entry of the virus into cells of the respiratory epithelium, while neuraminidase facilitates the release of newly produced viral particles (so-called virions) from infected cells. The inuenza virus has a marked propensity to mutate its external antigenic composition to escape the hosts' immune defences. Given this extreme mutability, the World Health Organisation (WHO) has introduced a classication of each viral subtype based on H and N typing. Additionally, strains are classied on the basis of antigenic type of the nucleoprotein core (A, B or C), geographical location of rst isolation, strain serial number and year of isolation. Every item is separated by a slash mark (e.g. A/Wuhan/359/95 [H3N2]). In this century there have been four pandemics caused by so-called antigenic shift (a major change in H conguration with or without a concomitant change in N and perhaps viral alteration of tissue tropism) leading to the appearance of a new subtype against which there is little circulating natural immunity. Pandemics are thought to originate in Southern China where ducks (the animal reservoir and breeding ground for new strains), pigs (which are thought to be the biological intermediate host or `mixing vessel') and humans live in very close proximity [2]. Minor changes in viral antigenic congurations, known as `drift', cause local or more circumscribed epidemics. The recently isolated Hong Kong avian inuenza (A/HK/156/97 [H5N1] virus appears to be an example of a zoonotic infection with direct spread of the avian virus to humans [35]. Pandemics by denition cause a very high morbidity and mortality burden [6]. The
191819 pandemic is estimated to have caused up to 40 million deaths world-wide. 1.1. Prevention and early treatment of inuenza Eorts to prevent or treat inuenza have had their mainstay in two separate approaches: vaccines and antivirals (ion channel inhibitors and neuraminidase inhibitors). 1.1.1. Inuenza vaccines Current inuenza vaccines are of four types: 1. whole virion vaccines which consist of complete viruses which have been `killed'; or inactivated, so that they are not infectious but retain their strainspecic antigenic properties. 2. subunit virion vaccines which are made of surface antigens (H and N) only. 3. split virion vaccines in which the viral structure is broken up by a disrupting agent. 4. live vaccines (as yet unlicensed). The rst three types of vaccines contain the two surface antigens; whole virion and split vaccines also contain antigens which are thought to contribute to a higher rate of vaccine reactions compared to subunit vaccines. Appendix A shows a list of inuenza vaccine producers and products world-wide, compiled by WHO in 1996 [7]. Periodic antigenic drifts and shifts pose problems for vaccine production and procurement, as a new vaccine closely matching circulating antigenic conguration must be produced and procured for the beginning of each new inuenza `season'. To achieve this, WHO has established a world-wide surveillance system allowing identication and isolation of viral strains circulating in the dierent parts of the globe. Sentinel practices recover viral particles from the naso-pharynx of patients with inuenza-like symptoms and the samples are swiftly sent to the laboratories of the national inuenza centres (110 laboratories in 79 countries). When new strains are detected the samples are sent to one of the four WHO reference centres (London, Atlanta, Tokyo and Melbourne) for antigenic analysis. Information on circulating strains is then sent to WHO, who in February of each year recommends, through a committee, the strains to be included in the vaccine for the forthcoming `season'. Individual governments may or may not follow WHO recommendations. Australia, New Zealand and more recently South Africa follow their own recommendations for vaccine content. Surveillance and early identication thus play a cen-
960
V. Demicheli et al. / Vaccine 18 (2000) 9571030
tral part in the composition of the vaccine. Traditionally, inuenza vaccines have been targeted to the elderly and those at serious risk of complications. Despite clear theoretical advantages in the use of vaccines, their uptake has been patchy. Studies in family practices suggest that 20% is a reasonable estimate of inuenza vaccine utilisation in the Canadian population [810]. The current low level of inuenza vaccine uptake in targeted populations may reect uncertainty on the part of primary care and public health practitioners and health policy decision-makers regarding vaccine eectiveness. One possible reason may be the diversity of regulations for the nancing and reimbursement of the vaccines. Other reasons may include perceived low ecacy due to the mutable viral conguration, the perceived commonality of the disease, which may breed contempt and, strangely, a misperception of the burden imposed by the disease on society. Nowhere is this more marked than in the case of healthy adults in employment, a population which would most benet from protection against inuenza. Epidemics in settings such as schools, barracks, prisons, oces, hospitals and industrial complexes cause great losses, but are seldom prevented by vaccination of sta. Despite the publication over a period of more than ve decades of a large number of reports of controlled clinical trials, there remains substantial uncertainty about the clinical eectiveness of inuenza vaccine. This uncertainty is manifested in widely varying estimates of vaccine eectiveness in the current health care literature. For example MMWR states: `The eectiveness of inuenza vaccine in preventing or attenuating illness varies, depending primarily on the age and immunocompetence of the vaccine recipient and the degree of similarity between the virus strains included in the vaccine and those that circulate during the inuenza season. When a good match exists between vaccine and circulating viruses, inuenza vaccine has been shown to prevent illness in approximately 7090% of healthy persons aged <65 years' [11]. To our knowledge there are no systematic reviews of the eects of vaccination on healthy adults, although there are several examples of reviews in the elderly such as the studies by Gross and Strassburg [12,13]. For example, Strassburg meta-analysed 17 controlled studies of inuenza vaccine eectiveness among elderly subjects. However all but two of the primary studies included in his analysis were non-experimental [13]. The only attempt at a comprehensive review of the inuenza vaccine eectiveness literature was conducted by Couch for the US Oce of
Technology Assessment. Couch reviewed 68 trials `reporting eectiveness against naturally occurring inuenza' (56 type A inuenza, 12 type B) [14]. His sources for identication of primary studies were: CG Lossli, International Bibliography of Inuenza 1930 59; Medlars Service of NLM; and Cumulative Index Medicus. His ndings included the following: . The range of eectiveness for each virus type was 0 96% . The majority of trials reported eectiveness greater than 60% for homologous virus challenge, but protection against heterologous virus was more variable [14] . The commonly quoted gure of 70% protection against illness (`clinical inuenza') in these circumstances (`if the epidemic virus is antigenically similar to the vaccine virus and if vaccine is given in the immediate few months preceding exposure') seems reasonable' [14] The wide variation in protection observed in controlled trials may be related to features of the inuenza virus, the vaccine, the target population or the study design. The most salient of these are discussed below. 1.1.1.1. The virus. The phenomenon of antigenic drift/ shift among inuenza viruses can result in a less than perfect and at times non-existent match between vaccine strain(s) and prevalent strain(s). The protective eect of vaccination would be expected to vary with the closeness of the antigenic match. There are two clinically important types of inuenza virus A and B. 1.1.1.2. The vaccine. Vaccines may vary in antigenic potency, composition (e.g. monovalent, bivalent, trivalent or polyvalent) or method of preparation (e.g. live or inactivated; whole virus, split virus or subunit vaccines, aqueous or oil adjuvant). Inuenza vaccines may act to modify as well as prevent illness. 1.1.1.3. The target population. Study populations vary in age, health status and type of living arrangements (e.g. institutional, communal or independent household). Some of these characteristics may aect immune responsiveness to vaccination or likelihood of contracting inuenza (which in turn aects statistical power and the play of chance on observed eect size). 1.1.1.4. The study design. Protective eect in clinical trials might be substantially inuenced by the outcome measure used. Inuenza cannot be satisfactorily distinguished on clinical grounds from respiratory infections caused by other chiey viral organisms. As a consequence, dilution of any eect of intervention can
V. Demicheli et al. / Vaccine 18 (2000) 9571030
961
be expected when purely clinical outcome measures are used. This is particularly true when the incidence of inuenza is low, when the period of observation extends beyond the usual four to 12 week annual period of inuenza activity, or when the denition of illness is imprecise (e.g. respiratory illness). To the extent that inuenza vaccine modies illness which it does not prevent, protection might be greater for outcomes which reect complications of inuenza (e.g. hospitalisation with respiratory illness) rather than primary infection (e.g. acute respiratory illness). Conventionally, serological diagnosis is based on a fourfold or greater increase in antibody titre to one or more virus antigens. There is evidence that vaccinated individuals are less likely than non-vaccinated persons to mount an antibody rise following infection with an inuenza virus antigenically related to strains contained in the vaccine. This phenomenon is thought to be based, at least in part, on higher pre-infection antibody titres which result from vaccination. Serological methods will therefore `miss' cases of inuenza among vaccinated subjects and could be expected to produce a spuriously high observed protective eect. Hobson has suggested (without citing supportive evidence) that virus isolation results may be similarly biased. He proposes that vaccines which fail to protect against clinical illness may reduce the amount and duration of virus shedding [15]. Other study design features which might inuence observed vaccine eectiveness include method of allocation, extent of blinding and type of virus challenge (natural or articial). Variability would be expected to be greater in studies with small sample sizes. The deciencies of most current and past reviews of inuenza vaccine eectiveness can be summarised as follows: 1. lack of comprehensiveness in the identication of primary studies 2. lack of methodological assessment of primary studies 3. failure to satisfactorily account for (or in some cases, to acknowledge) the marked variability in vaccine eectiveness among controlled studies 4. failure to provide estimates of vaccine eectiveness under conditions of imperfect antigenic matching between vaccines and prevalent viruses (that is, when vaccines contain either a dierent strain or a dierent subtype of inuenza virus than the prevalent virus) 5. lack of credible estimates of vaccine eectiveness in specic populations currently targeted for inuenza vaccination (for example, institutionalised elderly, community-dwelling elderly and persons with under-
lying medical conditions associated with a high risk of complications [16,17]. These deciencies help to explain discrepancies in reported vaccine eectiveness in the existing literature. Moreover, they can be expected to give rise to uncertainty among clinicians and policy-makers regarding the expected eectiveness of inuenza vaccine in the population groups for which annual inuenza vaccination is currently recommended. In this scenario a systematic review of the eects of vaccines against naturally occurring inuenza is necessary to enable decision-makers to devise strategies to deal with inuenza based on evidence. 1.1.2. Ion channel inhibitor antivirals (Amantadine and Rimantadine) The main antiviral compounds used against inuenza are amantadine hydrochloride and rimantadine hydrochloride (amantadine and rimantadine for short). Amantadine (an anti-Parkinsonism) was introduced in the 1950s and found to have antiviral activity in 1965. In the USA, amantadine was licensed for the treatment and prophylaxis of inuenza A/ H2N2 infections by the FDA in 1966 and for prophylaxis and treatment of all inuenza A infections in 1976. Rimantadine was licenced in 1993 [18]. In the USA, while amantadine is licensed for treatment and prophylaxis of adults and children over the age of one, rimantadine is licensed only for prophylaxis in children as well as for treatment and prophylaxis in adults [18]. In the UK amantadine only is licensed and is administered orally at a recommended does of 100 mg a day in healthy adults for ve days (treatment role) or 100 mg a day as long as the risk of infection lasts (prophylaxis role). Both compounds interfere with the replication cycle of type A (but not type B) viruses [19] and are thought to be ecacious and, given their virus-specic action, relatively free of adverse eect. Drug resistant H3N2 subtype inuenza A viruses have been isolated during treatment with amantadine and rimantadine, especially in institutions, but their clinical signicance is unclear [20]. Given both drugs' apparent ecacy in both prophylactic and therapeutic roles (if administration is started in time), their relatively scarce use is surprising [1]. Explanations for this nding include lack of awareness of the drugs and their properties by medical practitioners, lack of a rapid diagnostic capability and concern over their adverse eects, which include epilepsy. Even more surprising is the list of indications for use of both drugs. While subjects at high risk (i.e. subjects with underlying debilitating pathologies and the elderly) are included, healthy adults, es-
962
V. Demicheli et al. / Vaccine 18 (2000) 9571030
pecially those working in institutions (such as healthcare workers, nursing home attendants and the military) are not. These groups are likely to greatly benet from the use of the drugs, which could have a direct impact on length of sickness absence and diminish considerably the burden of inuenza epidemics to society. Additionally a non-systematic review of the evidence of the ecacy of rimantadine identied ve small double-blind placebo-controlled trials of both drugs in a prophylaxis role and nine trials in a treatment role [21]. The largest study contained 378 individuals, indicating the need to attempt pooling data to derive more precise estimates of eect and safety for the compounds. This systematic review of the eects of amantadine and rimantadine in healthy adults excludes children, the elderly and individuals with pre-existing pathologies. However, given the impact of inuenza in these populations, systematic reviews of the eects of amantadine and rimantadine in children, elderly and at-risk groups should also be carried out in the future. 1.1.3. Neuraminidase inhibitor antivirals (NIs) In recent years a new generation of antiviral compounds has been developed and is currently in preregistration phase III trials. These compounds, known collectively as neuraminidase inhibitors (NIs), are: . Nebulised Zanamivir developed by GlaxoWellcome PLC (UK). . Oral Oseltamivir (formerly known as Ro 64-0796 or GS 4104) co-developed by Gilead Sciences Inc. (Foster City, CA, USA) and Homann-La Roche Ltd (Basle, CH). Gilead Sciences Inc. still retains the intellectual property rights to Oseltamivir. Zanamivir is a so-called second-generation NI, whereas Oseltamivir represents the third generation of such compounds [22]. NIs act by inhibiting the entry of viral particles into the target cell and subsequent release of virions from the infected cell, neuraminidase being essential for both functions. Both Oseltamivir and Zanamivir appear to be eective against Inuenza A and B, while amantadine is eective only against inuenza A. NIs could be used in both a preventive role and to diminish the severity of the illness [23], to: . treat infected individuals . supplement protection against infection in individuals not fully protected by vaccination . provide protection for individuals unable to receive vaccine (e.g. individuals allergic to eggs) . provide short term prophylaxis in family settings . supplement vaccination during pandemics when vaccine stocks may be limited
. control outbreaks in institutions such as nursing homes or prisons . control outbreaks in settings such as factories, oces or the military . generally interrupt viral transmission. Homann-La Roche and GlaxoWellcome are targeting the registration and marketing of their compounds to the year 2000 inuenza season [24]. As NIs are likely, if proved eective and safe, to become a major form of prophylaxis and treatment of inuenza, reviewing and updating the available evidence is necessary to provide an accurate assessment of their eects.
1.2. Rationale for the economic evaluation J95, the British Army's ICD-based surveillance system, indicated that in soldiers respiratory disease is the second highest cause of morbidity and sixth highest cause of productivity losses (measured in working days lost, or WDL) both on world-wide military operations and when in barracks [25]. Further work carried out by the Department of Public Health of the University of Glasgow [26] shows that within the `respiratory disease' code block approximately 40% of the morbidity in the 19961997 season was caused by clinical inuenza. In some Army subpopulations (such as recruits undergoing training) the burden of respiratory disease is much higher (37 attendances per 1000 personnel per month in Training Establishment compared to 13 attendances per 1000 personnel per month in the rest of the Army). Inuenza, then, is an important recurring public health problem for the British Army, as it threatens the health and hence eciency of its workforce, the most important resource that any organisation has at its disposal. Before embarking in a major expenditure programme to purchase large quantities of these interventions (given that clinical inuenza is a disease of such high incidence among the military) the Ministry of Defence of the United Kingdom wanted to make sure that resources used in the prevention programme would be recouped by its benets. This provided the rationale for an economic evaluation comparing the costs and eects of each course of action. However, preliminary work prior to undertaking the evaluation indicated that there were considerable uncertainties as to the eectiveness and safety of vaccines, antivirals and NIs. This provided the main reason for the commissioning of three Cochrane reviews [2729] prior to carrying out the economic evaluation. The evaluation has been conducted and reported according to the BMJ guidelines for economic submissions [30].
V. Demicheli et al. / Vaccine 18 (2000) 9571030
963
2. Methods 2.1. Methods for the reviews 2.1.1. Objectives In comparisons between groups intended for the interventions and control/placebo groups the following hypotheses were tested: 2.1.1.1. Cases. There is no dierence in the number of cases of inuenza and their severity. 2.1.1.2. Adverse eects. There is no dierence in the number and severity of adverse eects (both systemic and localised). 2.1.2. Selection criteria See Table 1. 2.1.3. Search strategy . A MEDLINE search was carried out using the extended search strategy of the Cochrane Acute Respiratory Infections (ARI) Group [31] with the following search terms or combined sets from 1966 to the end of 1997 in any language: inuenza; route (oral) OR route (parenteral); vaccine; amantadine; rimantadine; neuraminidase inhibitors; Oseltamivir ; GS 4104; Ro 64-0796; Zanamivir . The bibliography of retrieved articles was examined in order to identify further trials . A search was carried out of the Cochrane Controlled Trials Register (CCTR) and of EMBASE (199097 for Inuenza Vaccines and for NIs; 1985 to 1997 for Amantadine and Rimantadine) . The journal Vaccine was handsearched from its rst issue to the end of 1997 [32,33] . The manufacturers, rst or corresponding authors of evaluated studies and researchers active in the eld were contacted in order to locate unpublished trials.
2. measure(s) taken to conceal treatment allocation (dened as methods to prevent selection bias, i.e. to ensure that all participants have the same chance of being assigned to one of the arms of the trial. This protects the allocation sequence before and during allocation) 3. number of drop-outs of allocated healthcare worker participants from the analysis of the trial (dened as the exclusion of any participants for whatever reason deviation from protocol, loss to followup, withdrawal, discovery of ineligibility; while the unbiased approach analyses all randomised participants in the originally assigned groups regardless of compliance with protocol, known as intention to treat analysis) 4. measures taken to implement double blinding (a double-blind study is one in which observer(s) and/ or subjects are kept ignorant of the group to which the subjects are assigned, as in an experiment, or of the population from which the subjects come, as in a non-experimental situation. Unlike allocation concealment, double blinding seeks to prevent ascertainment bias and protects the sequence after allocation) For criteria 2, 3 and 4 there is empirical evidence that low quality in their implementation is associated with exaggerated trial results [34] and it is reasonable to infer a quality link between all four items. The four criteria were assessed by answering a questionnaire; see Appendix B. 2.1.3.2. Data collection. The following data were extracted, checked and recorded: . Characteristics of trials: date; location; setting; case denitions used (clinical, serological, virological); surveillance system; type and length of epidemic (denition used, characteristics of circulating virus); sponsor (specied, known or unknown); publication status . Characteristics of participants: number of participants; age; gender; ethnic group; risk category; occupation . Characteristics of interventions: type of intervention; type of placebo; dose; treatment or prophylaxis schedule; length of follow-up (in days); route of administration . Characteristics of outcome measures: * Numbers and seriousness of inuenza cases (however dened) occurring in vaccine and placebo groups. Other outcome measures used to assess eects included cases of inuenza clinically dened; cases of inuenza clinically dened on the basis of a specic list of symptoms and/or signs; cases of inuenza conrmed by laboratory
2.1.3.1. Trial quality assessment. Two reviewers read all trials retrieved in the search and applied inclusion criteria. Trials fullling these criteria were assessed for quality and results analysed by the same authors. Disagreements on trial quality were arbitrated by a third author. Assessment of trial quality were made according to the following criteria: 1. generation of allocation schedule (dened as the methods of generation of the sequence which ensures random allocation).
964
Table 1 Selection criteria applied to retrieved studies to determine inclusion in systematic review Participants Apparently healthy, r75% aged 14 to 60 Intervention irrespective of viral antigenic conguration Numbers and/or severity of inuenza cases (however dened) occurring in intervention and placebo groups No other specic criteria Interventions Clinical outcomes Adverse eects Number and seriousness of adverse eects
Review
Study criteria
Selection criteria common to all
Inuenza vaccines
Randomised/quasirandomiseda studies in humans compared to placebo, controls, no intervention; or comparing types, doses/schedules of intervention Protective eect of inuenza vaccine from exposure to naturally occurring inuenza Inuenza immune status irrelevant Attenuated, killed or live vaccines or fractions thereof administered by any route
V. Demicheli et al. / Vaccine 18 (2000) 9571030
Amantadine and rimantadine for inuenza
Protection or treatment of amantadine and/or rimantadine from exposure to naturally occurring inuenza
No other specic criteria
Amantadine and/or rimantadine as prophylaxis and/or treatment for inuenza
No other specic criteria
NIs for inuenza
Protective/ treatment eect of oral Oseltamivir and/or Zanamivir in naturally or articially occurring inuenza
No other specic criteria
Oseltamivir and/or Zanamivir as prophylaxis and/or treatment for inuenza
Also temporal distribution of cases, and other outcomes e.g. distribution of symptoms under the curve; time to improvement
Systemic eects include of malaise, nausea, fever, arthralgias, rash, headache and more generalised and serious signs. Local eects include induration, soreness and redness at inoculation site (injected vaccines) and rhinitis and sore throat (inhaled vaccines) GI (diarrhoea, vomiting, dyspepsia, nausea, constipation); increased CNS activity (light-headedness, concentration problems, insomnia, restlessness, nervousness); decreased CNS activity (malaise, depression, fatigue, vertigo, feeling drunk); skin (urticaria and rash) Local and systemic adverse eects
a A study is randomised when it appears that the individuals (or other experimental units) followed in the study were denitely or possibly assigned prospectively to one of two (or more) alternative forms of health care using random allocation. A study is quasi-randomised when it appears that the individuals (or other experimental units) followed in the study were denitely or possibly assigned prospectively to one of two (or more) alternative forms of health care using some quasi-random method of allocation (such as alternation, date of birth or case record number).
V. Demicheli et al. / Vaccine 18 (2000) 9571030
965
tests; hospital admissions; complications; working day lost in episodes of sickness absence regardless of cause Adverse eects: presence and type, with local symptoms presented in the analysis separately from systemic symptoms; number of withdrawals due to adverse eects. Individual adverse eects have been considered in the analysis, as well as a combined endpoint (any or highest symptom).
Hospital admission rates. Hospital admission rates were calculated as the proportion of cases hospitalised for respiratory causes. Complications. Complications were considered as the proportion of cases complicated by bronchitis, pneumonia or otitis. 2.1.3.4. Data synthesis. The relative risks of events (cases of inuenza, deaths, and adverse eects) comparing treatment and placebo/control groups from the individual trials were combined using MantelHaenszel meta-analytical techniques. We did not combine estimates from treatment and prophylactic trials as these were conducted to answer dierent study questions. Between-trial variability in results was examined and incorporated into the estimates of uncertainty of treatment eect using random eects models where appropriate. In treatment trials the choice of methods for combining the estimates of severity of inuenza depended on the format in which the data was presented. Where possible, comparisons were made between the mean duration of symptoms in the two groups, and methods for combining dierences in means were used. Specically, where the data were presented as the number of subjects with duration of symptoms beyond a cut-o time period these were presented as `Cases with fever at 48 h'. The bewildering array of outcomes used in the treatment trials (see Results section) prevented us from using more than the `cases with fever' outcome. Included trials did not contain sucient information to enable us to assess the number of cases with no documented fever at entry into the trial. For the vaccine trials, separate analyses were performed for live aerosol vaccines, inactivated parenteral vaccines and inactivated aerosol vaccines. Clinical inuenza outcomes were specied according to whether specic criteria were or were not used, for which estimates were produced separately, and combined (where trials reported both denitions, only the wider denition was retained for analysis). Vaccine ecacy was estimated by calculating the common relative risk, using the Mantel-Haenszel method (xed eect model) when the trial results were consistent, or the DerSimonian and Laird method (random eects model) when signicant heterogeneity was evident between the study results. Between-study heterogeneity is to be expected in vaccine trials as there are unpredictable systematic dierences between trials in circulating strains and levels of local immunity. Once the relative risk (RR) had been obtained, vaccine ecacy (VE) was calculated as VE=1-RR. Similar analyses were also undertaken for other events, such as complications, hospital admissions and adverse eects.
2.1.3.3. Denitions Epidemic period. Four dierent denitions of `epidemic period' were found: . the interval between the rst and the last virus isolation in the community . the interval during which inuenza virus was recovered from more than a stated percentage of ill subjects . the period during which an increase of respiratory illness more than a stated percentage was recorded . the winter period taken as a proxy for epidemic period. The data were included regardless of the denition of epidemic period used in the primary study. When data were presented for the epidemic period and the entire follow-up period, those occurring during the former were considered. Clinically dened case. A clinically dened case was assumed as any case denition based on symptoms without further specication. The specic denition was assumed as: . `u-like illness' according to a predened list of symptoms (including the CDC case denition for surveillance) . `upper respiratory illness' according to a predened list of symptoms. When more than one denition was given for the same trial, data related to the more specic denition were included. Laboratory conrmation of cases. The laboratory conrmation of cases found were: . virus isolation from culture . four-fold antibody increase (HI) in acute or convalescent phase sera . four-fold antibody increase (HI) in post-vaccination or post-epidemic phase sera. When more than one denition was given for the same trial, data related to the more sensitive denition (seroconversion) were included.
966
V. Demicheli et al. / Vaccine 18 (2000) 9571030
In addition to the traditional estimate of vaccine ecacy, the eect of vaccination on the number of clinical cases was estimated by averaging the risk dierences (inuenza rate in vaccinated group minus inuenza rate in control group). Where the total number of clinical inuenza cases depends more on the number of other inuenza-like illnesses than true inuenza A illnesses, it is more likely that an intervention will appear to reduce the total number of cases by an absolute amount (i.e. a constant risk dierence) than by a relative amount (i.e. a constant relative eect). As the data on average time o work was reported as a continuous measurement, these results were expressed as dierences in means, and combined using the weighted mean dierence method. Caution should be exercised in interpreting these results as the data are very skewed. Several trials included more than one active vaccine arm. Where several active arms from the same trial were included in the same analysis, the placebo group was split equally between the dierent arms, so that the total number of subjects in any one analysis did not exceed the actual number in the trials. 2.1.4. Methods for the economic evaluation 2.1.4.1. Evidence-based alternative interventions to minimise the burden of inuenza. While the three Cochrane reviews were underway, we assumed a hypothetical scenario in which all available means had a preventive and treatment impact on inuenza. We also considered it likely that such means would produce adverse eects and have clinical outcomes not homogeneous for quality of life. In this case, the alternatives to be explored would be: . which is the best single alternative . which is the best combination of alternatives . which is the best combination of alternatives depending on the outcome measure considered (avoided cases, quality weighted avoided cases, severity of avoided cases, hospital admissions avoided and working days lost (WDL)). We aimed to compare these alternatives with the current Army policy on inuenza prevention (do-nothing). Once the reviews had been completed, the results led us to introduce considerable changes to our comparators. The changes (with the reasons in brackets) are summarised in Table 2. For our evaluation we chose the viewpoint of the funder, the MOD (UK). We thus focused on the eects of preventing inuenza in MOD/Army personnel although we believe that our methods are equally applicable to populations of employed healthy adults,
especially in an epidemic situation. These would include emergency services and employees of companies producing essential goods and services. We were able to test the eect of this assumption by setting our results in the context of a distribution of similar variables derived from our widely known and recently updated systematic review of the economics of inuenza [6,35,36]. We attempted to incorporate into our evaluation individual soldier preferences for the possible preventive means. One of the eects of adopting the viewpoint and decision-making perspective of the MOD/ Army was the possibility of incorporating the inuenza preventive campaign into existing immunisation and routine procedures at no incremental administrative cost. However, in the sensitivity analysis we have used administration costs derived from the ratio `vaccine cost/total administration cost' calculated from our systematic review of the economics of inuenza [6,35,36]. Final selection of alternatives. Our nal criteria for the choice of alternatives were: . evidence of ecacy; . evidence of safety; . practicality of organisational implementation in the setting of the British Army. On the basis of the rst criterion all remaining alternatives in the third column of Table 2 are practicable and acceptable. However applying the other two criteria and assuming an average inuenza epidemic period of 46 days (as in the trials included in the reviews) the alternatives of oral amantadine, oral rimantadine and oral Oseltamivir are no longer practicable. It is very unlikely that whole bodies of soldiers would comply with the requirement of protracted daily oral drug schedules. This assumption was further conrmed by the nding of our preference time trade-o exercise (Table 4) in which soldiers preferred the risk of contracting inuenza to that of experiencing adverse eects such as nausea or gastrointestinal disturbances. Two other factors contribute to making the prevention of inuenza with antimicrobials and NIs problematic. Firstly it is doubtful whether the protracted logistical eort involved in maintaining the chemoprophylaxis campaign for 46 days is feasible. Secondly the level and timeliness of the information required to determine with any certainty the `beginning' and the `end' of the inuenza epidemic is unlikely to be available, especially when the Army is deployed in dierent areas of the UK and abroad. Description of alternatives. Whereas before the Cochrane review results our provisional decision tree was very complicated, comprising preventive and treat-
V. Demicheli et al. / Vaccine 18 (2000) 9571030 Table 2 Possible alternatives to prevent and treat inuenza, before and after reviews of the evidence Items Which is the best single alternative for prevention Before Cochrane reviews Oral vaccines Aerosol vaccines Parenteral vaccines Oral Amantadine Oral Rimantadine After Cochrane reviews Parenteral vaccines Oral Amantadine Oral Rimantadine Oral Oseltamivir (aerosol/oral vaccines are less eective, or dierences are minimal and do not currently represent a real alternative. Zanamivir trials only apparently included laboratory conrmed outcomes)
967
Inhaled Zanamivir Oral Oseltamivir Which is the best single alternative for treatment Oral Amantadine Oral Rimantadine Inhaled Zanamivir Oral Oseltamivir Prevention only Treatment only Prevention treatment Laboratory cases Clinical cases WDL Hospital admissions Deaths Complications 84 days (SD=33.6) according to Communicable Disease Reports `Inuenza Surveillance England and Wales' (199197)
None (all compounds shortened duration of illness by 0.5 days)
Which is the best combination of alternatives
Prevention only
Outcome measure
Laboratory cases Clinical cases (the prevention of clinical cases is the only public health target. Not enough outcome data were presented in the trials to include any other outcomes)
Length of epidemics (i.e. required duration of antiviral & NI preventive treatment)
62 days (SD=27) (according to inuenza vaccines trials included in the Cochrane review [27])
ment alternatives, the nal tree consists only of the three preventive arms each with inuenza cases with or without adverse eects. Form of the economic model. On the basis of the above considerations we dened an economic model based on the cost per avoided case to dene the best preventive strategy, and the cost per avoided case weighted by individual preference to dene the choice of the best combination of interventions. The cost per avoided case was calculated by dividing the total costs of the interventions by the number of cases avoided. Data collection and assumptions made. We based our model on a set of assumptions, which are summarised in Table 3. The variables and the ranges across which we carried out our sensitivity analysis together with the rationale are summarised in Table 4.
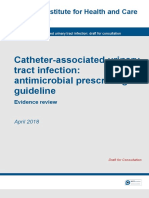
3. Results 3.1. Results of the reviews 3.1.1. Description of studies Identied trials are listed and described in the table of included studies using the name of the rst author and the publication year; see Appendix C. A list and description of excluded studies (with reason for exclusion) is available from the authors. 3.1.1.1. Inuenza vaccines. The tables of comparisons were constructed according to the following criteria (Fig. 1): 1. Inuenza vaccine versus placebo * All studies comparing any inuenza vaccine against a placebo (inert substances or non
968 Table 3 Basic assumptions of the model Variable Population Gender and age dierences Incidence of inuenza Eectiveness Adverse eects Individual preferences Preventive intervention costs
V. Demicheli et al. / Vaccine 18 (2000) 9571030
Assumption Army eectives as at 1 August 1998 Only incidence dierences will be tested in sensitivity analysis Sickness rates for inuenza in 1997 Meta-analysis estimate of RCTs using inuenza clinical outcomes Frequent symptom reported in RCTs included in Cochrane reviews comparable across range of preventive interventions Mean score of preferences expressed as combination of category rating and time-tradeo Acquisition costs
Source/Rationale Defense Analytical Services Agency (DASA) DASA DASA Cochrane Reviews [2729] Cochrane Reviews [2729] Study on a sample of 40 soldiers Defense Medical Supply Agency and authors' assumption (NI) Cochrane Review [27] Interviews with medical commanders Preventive interventions do not have dierent eects under this perspective Diculties in valuation
Duration of treatment for antivirals and NIs Mean duration of inuenza epidemics from vaccines RCTs Preventive intervention administration costs Nil Productivity losses due to inuenza Nil Productivity loss from adverse intervention events Nil
inuenza vaccines) were included in this group Subgroup analysis were carried out for live aerosol vaccine, inactivated parenteral vaccine, and inactivated aerosol vaccine The parenteral route comprised both intramuscular and subcutaneous route Dierent dosages and schedules of the vaccine and the presence of dierent adjuvants were not compared; and data from arms of trials comparing only vaccine composition or dosage were pooled in the analysis.
cebo in the control arm which may generate confusion The compliance of the study vaccine with the ocial recommendations was checked by reviewing WHO records when possible. In case of ambiguity (in the oldest trials), the opinion stated by authors was taken into account The compliance of a live attenuated vaccine with the recommendation has been decided according to the antigenic comparability to the wild strains
2. At least one vaccine strain recommended for that year (as an indicator of goodness of serological t) versus placebo or other vaccines: * All trials in which the studied vaccine contained at least one of the A strains recommended for that year by WHO or single governments (WHO recommendations were published since 1973 only) were included, independently from substances used in the control arm * Subgroup analysis was carried out according to control group for the recommended vaccine against placebo, against inuenza B vaccine, and against other non recommended A strains * Vaccines containing only a B recommended strain were excluded from this comparison since a number of authors used monovalent B vaccine as pla-
3. Vaccine matching circulating strain versus placebo or other vaccines: * All trials in which the studied vaccine contained the strain matching the circulating virus (or at least one of several circulating viruses) were included in this group of comparison, independently from substances used in the control arm * Subgroup analysis was carried out according to the control group; matching vaccine against placebo, against inuenza B vaccine, and against other non recommended A strains * In cases of an incomplete match or ambiguity of wording, the opinion stated by authors was also taken into account. Minor viral drift clearly stated was assumed as non-matching. Twenty papers describing 39 trials of sub-trials were identied. Some of them had more than two arms, comparing dierent vaccines, routes of administration,
V. Demicheli et al. / Vaccine 18 (2000) 9571030 Table 4 Assumptions tested in the sensitivity analysis Variable Incidence of inuenza Assumption Source/Rationale
969
Range of values from basic Army rate to training regiment rate Eectiveness Range of estimate from meta-analysis of RCTs using inuenza clinical outcomes case denition and from meta-analysis of RCTs using laboratory-based inuenza case denition Eectiveness Range of 95% Condence intervals around eect on outcome (clinical case denition) Adverse eects Range of incidence estimates with arbitrary variation Individual preferences 25th and 75th percentiles scores of preferences expressed as a combination of category rating and time-trade-o Duration of treatment for antivirals and Minimum and maximum duration of inuenza NIs epidemics from vaccines RCTs Vaccines administration costs Ratio of administration to vaccine costs derived from economic studies on vaccines Antivirals and NIs administration costs Arbitrary ratio of administration to drug costs
DASA, J97 & Glasgow University study [25,26] Cochrane Reviews [2729]
Cochrane Reviews [2729] Authors' assumption Study on a sample of 40 soldiers Distribution of duration is symmetrical. Cochrane Review [27] Systematic review of economic studies [6,36] Authors' assumptions
schedules or dosages. These trials were split into substudies. Some trials took in account the history of previous vaccine immunisations. Included trials assessed three kinds of vaccine: live attenuated aerosol, inactivated aerosol and inactivated parenteral. Four trials of live attenuated vaccine were included, all placebo controlled. These involved 26,369 subjects. The mean treatment size was 2028 individuals (median 999, 25th percentile 508, 75th percentile 1071), and the mean placebo arm size was 1739 (median 508,
25th percentile 289, 75th percentile 547 individuals). Two studies which assessed inactivated vaccine aerosol were included. Both were placebo controlled and involved 1506 subjects. The mean treatment size was 335 individuals (median 333, 25th percentile 195, 75th percentile 473), and the mean placebo arm size was 42 (median 42, 25th percentile 24, 75th percentile 59 individuals). Most studies assessed ecacy of inactivated parenteral vaccines against placebo or other inuenza vac-
Fig. 1. Summary of inuenza vaccines in healthy adults (95%CI=95% Condence intervals).
970
V. Demicheli et al. / Vaccine 18 (2000) 9571030
cines (some of them used a monovalent inuenza B vaccine as placebo). They involved 23,628 subjects. The mean treatment size was 550 individuals (median 432, 25th percentile 161, 75th percentile 920), and the mean placebo arm size was 358 (median 311, 25th percentile 66, 75th percentile 518 individuals). Surveillance methods were prospective or retrospective, active (by phone interview or questionnaire compilation) or passive (ill subjects spontaneously presenting). Mean length of follow up was 87 days (median 79 days, 25th percentile 61 days, 75th percentile 119 days). The duration of the epidemic was specied by 17 trials. Mean length of the epidemic period was 62 days (median 63 days, 25th percentile 42 days, 75th percentile 77 days). 3.1.1.2. Amantadine and Rimantadine Preventive trials. Seventeen preventive trials met the inclusion criteria. No unpublished trials were identied, despite receiving nine letters and three electronic communications from manufacturers, authors and researchers. The mean amantadine arm size was 494 individuals (median 151, 25th percentile 97, 75th percentile 348), the mean rimantadine arm size was 107 (median 108, 25th percentile 92, 75th percentile 122 individuals) and the mean placebo arm size was 373 individuals (median 140, 25th percentile 99, 75th percentile 269). The mean total population was 596 individuals (median 308, 25th percentile 225, 75th percentile 536). The mean length of follow up was 28 days (median 30 days, 25th percentile 18 days, 75th percentile 42 days). Treatment trials. Ten published treatment trials were identied. No unpublished trials were identied. The mean amantadine arm size was 91 individuals (median 72, 25th percentile 15, 75th percentile 110), the mean rimantadine arm size was 61 (median 56, 25th percentile 15, 75th percentile 104 individuals) and the mean placebo arm size was 77 individuals (median 76, 25th percentile 14, 75th percentile 99). The mean total population was 161 individuals (median 153, 25th percentile 30, 75th percentile 225). Mean length of follow up was 25 days (median 25.5 days, 25th percentile 16 days, 75th percentile 33 days). 3.1.1.3. Neuraminidase inhibitors Preventive trials. As at 1 January 1999 four accessible preventive trials met our inclusion criteria. A further two preventive trials of Zanamivir in abstract format were identied (Calfee H68 and Monto ). Further data was requested from the manufacturers, GlaxoWellcome, to allow the inclusion of data from the trials in the review. GlaxoWellcome provided the data as requested. The mean Zanamivir arm size was
136 individuals (median 34, 25th percentile 25, 75th percentile 61), the mean Oseltamivir arm size was 1040 (median, 25th percentile and 75th percentile 1040 individuals) and the mean placebo arm size was 189 individuals (median 21, 25th percentile 9, 75th percentile 397). The mean total population was 475 individuals (median 68, 25th percentile 36, 75th percentile 853). Mean length of follow up was 11 days. Treatment trials. As at 1 January 1999 three accessible treatment trials were identied which fullled the inclusion criteria. A further two treatment trials of Zanamivir in abstract format were also identied. Despite a request to the manufacturers, GlaxoWellcome did not release more detailed data in time for inclusion in the review. The mean Zanamivir arm size was 80 individuals (median 43, 25th percentile 25, 75th percentile 43), the mean Oseltamivir arm size was 920 (median 1040, 25th percentile 920, 75th percentile 1040 individuals) and the mean placebo arm size was 107 individuals (median 85, 25th percentile 22, 75th percentile 151). The mean total population was 315 individuals (median 243, 25th percentile 65, 75th percentile 449). Mean length of follow up was ve days. Preventive and treatment trials. Only one trial was identied containing both preventive and treatment interventions. 3.1.2. Methodological quality of included studies Two reviewers assessed allocation method, allocation concealment, blinding and completeness of follow-up. 3.1.2.1. Inuenza vaccines. There were 20 trials in all, 13 of which were placebo controlled. Three trials used an inuenza B vaccine in the control arm, considering it as a placebo. Four trials compared two or more inuenza vaccines but did not use a control arm. Thirteen trials reported data on adverse eects, but only seven were included in the analysis: one did not have sucient reporting and ve trials did not have a placebo arm. The overall quality of the trials was good. Assessed allocation concealment was adequate in 12 of the trials, inadequate in six and unclear in two. Fifteen trials were properly randomised, four stated that the allocation method was quasi-random, and one trial did not report information about randomisation. Assessment was double blinded in 14 trials. Two trials were single blinded and four did not mention blinding. Two studies were eld trials. 3.1.2.2. Amantadine and Rimantadine. There were 27 trials in all, 26 of which considered either amantadine and/or rimantadine ecacy and one which considered
V. Demicheli et al. / Vaccine 18 (2000) 9571030
971
adverse eects only. Eleven preventive trials and seven treatment trials reported sucient data on adverse eects. The quality of preventive and treatment trials is discussed separately. Preventive trials. The quality of the preventive trials was relatively good, considering the age of the trials. Among the 17 preventive trials, 15 stated that the allocation method was randomisation, although only four mentioned a particular method and two did not mention random allocation at all. These two trials have therefore been classied as controlled clinical trials (CCTs) rather than RCTs. All preventive trials were stated to be double blind with the exception of Payler which was open and had no placebo group (the comparison group was no intervention other than inuenza vaccine at the beginning of the season). Treatment trials. Among the 10 treatment trials, nine stated that the allocation method was randomisation; no trials mentioned a particular method; and one (Hornick) did not mention random allocation at all. Major aws in the reporting of trials lay in the following: . Lack of information on the completeness of followup. In many trials there was a large dierence between the number randomised and the number who actually participated . Lack of detailed description of methods to conceal allocation, with many trials just describing a `double blind' procedure . Frequent inconsistencies in the reporting of numerators and denominators in various arms of trials . In the treatment trials, the use of a bewildering variety of outcomes, such as severity scores, of which none are alike. This makes the task of meta-analysis impossible and leads to a great loss of information. 3.1.2.3. Neuraminidase inhibitors. Overall methodological quality appeared good, in keeping with the mainly early report nature of the results of the clinical trials of such potentially important compounds. However, detailed descriptions of methods and steps taken to ensure allocation concealment were not specic, leading us to grade this aspect of the trials `unclear'. This is potentially a very important point when dealing with cases of self-limiting upper respiratory tract infections with or without systemic symptoms, in which the potential for a placebo eect is great. Additionally as some trials (the WV series for instance) relied on clinical case denitions the potential for bias (and overestimation of eect) is even greater.
3.2. Eects of inuenza vaccines 3.2.1. Eect of vaccination on clinical cases of inuenza Trial data for the two denitions of inuenza (no case denition and specic case denition) are presented separately for each of the three types of vaccine: live aerosol, inactivated parenteral and inactivated aerosol. Signicant heterogeneity was detected between trial results for most comparisons, and the gures quoted are estimated from random eects models. The live aerosol vaccines were not eective for cases of either denition. A combined analysis of data from the two trials estimated the vaccine ecacy to be 2% (95%CI: 58%). The inactivated vaccines did oer signicant protection. Taking the data from the 10 trials together, regardless of case denition, the parenteral vaccine reduced the number of cases by 29% (95%CI: 12 42%). The ecacy of the inactivated aerosol vaccine was higher for the unspecied case denition (VE=31%, 95%CI: 551%) but not the specic inuenza case denition (VE=26%, 95%CI: 145%). The estimates of ecacy were more consistent when the treatment eect was expressed as a risk dierence rather than a relative eect. Estimation as risk dierences suggest that 5% (95%CI: 28%) and 9% (95%CI: 316%) fewer participants experienced inuenza like illnesses who received inactivated parenteral vaccine and inactivated aerosol vaccine respectively. 3.2.2. Eect of vaccination on serologically conrmed cases of inuenza Data from two studies showed that aerosol live vaccines reduced the number of serologically conrmed cases of inuenza by 79% (95%CI: 4492%). Six studies provided data for inactivated parenteral vaccines, showing a similar ecacy of 65% (95%CI: 4479%). No studies of inactivated aerosol vaccine reported numbers of serological conrmed cases. 3.2.3. Eect of vaccination on other outcomes Three trials of parenteral inactivated vaccine evaluated time o work, estimating that vaccination saved on average around 0.4 working days. This result was nearly statistically signicant. Hospital admissions were also lower, but not statistically signicant. There was little dierence in complication rates between vaccinated and unvaccinated groups. 3.2.3.1. Adverse eects aerosol live vaccines. Whilst signicantly more recipients experienced sore throats after vaccine administration than placebo administration (relative rate=2.5, 95%CI: 1.54.2), the overall number of local adverse eects was not signicantly dierent between vaccine and placebo groups. There
972
V. Demicheli et al. / Vaccine 18 (2000) 9571030
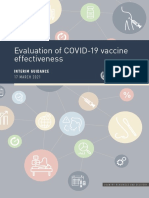
was also no signicant increase in systemic side eects, although rates of fever and myalgia were higher in vaccine than placebo groups. Overall 26% of vaccine recipients reported the combined endpoint for local reactions, whilst only 8% reported the combined endpoint for systemic eects. 3.2.3.2. Adverse eects inactivated vaccines. Local tenderness and soreness was more than twice as common among parenteral vaccine recipients than those in the placebo group (relative rate=2.1, 95%CI: 1.43.4). There were also increases in erythema (non-signicant), but not in duration of or arm stiness. The combined local eects endpoint was signicantly higher for those receiving the vaccine (relative rate=2.6, 95%CI: 1.6 4.2), with 69% reporting some eect. None of the systemic eects were individually more common in parenteral vaccine recipients than placebo recipients. However the combined endpoint was increased, and nearly statistically signicant, with 26% vaccine recipients reporting some side eect than placebo recipients (95%CI: 059%). Overall 30% of those receiving the vaccine reported possible systemic eects, although many of these equally could be attributed to inuenza-like illnesses. None of the trials on inactivated aerosol vaccines reported side-eects that could be included in the analysis. The two studies which evaluated these vaccines included parenteral components using an inuenza B control group so that the side-eects of the oral vaccine could not be estimated separately. 3.2.4. Recommended vaccines Sixteen trials evaluated the eect of the vaccines recommended (by WHO or single governments) on clinical cases of inuenza. Nine of these trials were placebo controlled, ve made comparisons with inuenza B vaccine, and two compared recommended inuenza A vaccines with non-recommended inuenza A and B vaccines. An additional trial (Tannock) only reported serologically conrmed cases. Live aerosol, inactivated parenteral and inactivated aerosol all had similar vaccine ecacies, although the estimate for inactivated aerosol vaccines was only based on the results of one trial. Live aerosols had a vaccine ecacy of 13% (95%CI: 520%), inactivated parenterals an ecacy of 24% (95%CI: 1532%), and inactivated aerosols an ecacy of 40% (95%CI: 13 59%). Combining the data from all three vaccine types from the placebo controlled trials, the overall estimate of vaccine ecacy was 24% (95%CI: 1433%). The estimate decreased to 22% when the non-placebo controlled trials were included (Fig. 2). Again, the individual study results were more consistent when expressed as risk dierences than relative
eects. Overall the percentage of participants experiencing clinical inuenza decreased by 5% (95%CI: 3 7%) using data from the placebo controlled trials. The reductions were 3%, 5% and 9% for the live aerosol, inactivated parenteral and inactivated aerosol vaccines respectively, the rst gure not being statistically signicant. There were signicant reductions in serologically conrmed cases of inuenza for live aerosol and inactivated parenteral preparations. There was no data for inactivated aerosol vaccines. Vaccine ecacy was estimated as 48% (95%CI: 2464%) for live aerosol vaccines, and 68% (95%CI: 4979%) for inactivated parenteral vaccines. 3.2.5. Vaccine matching the circulating strain The highest estimates of vaccine ecacy come from the analyses of vaccines which were shown to match the circulating vaccine strain. Twelve trials were included in these analyses, and seven were placebo controlled. Since several studies had more than two arms, the ecacy of the vaccines containing the matching strain was compared against non-matching A or B inuenza vaccines. None of the live aerosol vaccines used in the trials matched circulating strains. Estimates of the ecacy of both parenteral and aerosol inactivated vaccines in reducing cases of clinical inuenza were similar. Overall the vaccine ecacy based on results of the placebo controlled trials was 37% (95%CI: 1852%). The estimate declined to 31% when the non-placebo controlled trials were included. Expressing the ecacy as a risk dierence, on average 7% (95%CI: 410%) fewer participants who received matched vaccine suered inuenza like illnesses compared to placebo recipients. The eect of the matched vaccine on serologically conrmed cases was also larger than in any other analysis. Overall the results of seven trials reporting serologically conrmed cases estimated the vaccine ecacy to be 72% (95%CI: 5483%).
3.3. Eects of amantadine and rimantadine All trials tested the eects of amantadine and rimantadine on a wide variety of inuenza A viruses. None tested the eects on inuenza B, on which the molecules are known to be ineective. Also, no trial tested the role of the compounds on workplace outbreak control, which is a pity considering the trial settings (prisons, factories, schools, barracks). Some trials are likely to have included individuals who took aspirin to relive symptoms (especially in the
V. Demicheli et al. / Vaccine 18 (2000) 9571030
973
Fig. 2. At least one vaccine recommended for that year compared to placebo or other vaccine in inuenza cases clinically dened (Expt=experimental arm, ctrl=control arm; 95%CI=95% Condence intervals).
974
V. Demicheli et al. / Vaccine 18 (2000) 9571030
treatment trials). However the eects of this potential confounder should have been eliminated by the process of randomisation. All trials commenced administration of the compounds within a reasonable time lapse. When the results of surveillance made it reasonable to do so, treatment started at the latest 48 h after positive identication of the rst case in the population and prevention. Six main comparisons were carried out: 1. Comparison A oral amantadine compared placebo in inuenza prevention 2. Comparison B oral rimantadine compared placebo in inuenza prevention 3. Comparison C oral amantadine compared oral rimantadine in inuenza prevention 4. Comparison D oral amantadine compared placebo in inuenza treatment 5. Comparison E oral rimantadine compared placebo in inuenza treatment 6. Comparison F oral amantadine compared oral rimantadine in inuenza treatment to to to to to to
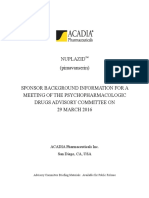
take place in the rimantadine or placebo arms. Overall both drugs appear to be eective and well tolerated, although the evaluation of the eects of rimantadine was carried out on a very small study population. In all comparisons duration of action and protection appeared directly related to duration of prophylaxis or treatment with amantadine and rimantadine. This nding is in keeping both with the half-life of the compounds which are excreted by the kidneys (at the rate of 6.4 ml/min/kg for amantadine and 1.2 ml/min/kg for rimantadine [37]) and the self-limiting duration of the illness. No trials assessed onset of resistance to the drugs although this is known to be of relatively short induction time (1027% of patients secrete drug-resistant virus within 45 days of commencing treatment [37]). 3.3.1. Comparison A oral amantadine compared to placebo in inuenza prevention 3.3.1.1. Ecacy. Amantadine: 61% (95%CI: 5169%) ecacious (RR 0.39 95%CI: 0.310.49) in preventing clinically and laboratory dened inuenza cases; 23% (95%CI: 1134%) ecacious (RR 0.77 95%CI: 0.660.89) in preventing clinically dened inuenza cases (Fig. 3). There was a signicant variation in the trial results for the second outcome. 3.3.1.2. Adverse events. All categories of adverse eects were signicantly more common in participants who received amantadine than placebo, except for dermatological changes. Nearly twice as many amantadine recipients experienced both increased or decreased CNS eects, and more than twice as many withdrew from the trials due to adverse eects (Table 5). 3.3.2. Comparison B oral rimantadine compared to placebo in inuenza prevention 3.3.2.1. Ecacy. Rimantadine: 72% (95%CI: 8 92%) ecacious (RR 0.28 95%CI: 0.081.08) in preventing clinically and laboratory dened inuenza cases; 35% (95%CI: 2065%) ecacious (RR 0.65 95%CI: 0.351.20) in preventing clinically inuenza cases (Fig. 4). The signicance of these ndings depends on whether a xed or random eect model is used. 3.3.2.2. Adverse events. Rimantadine recipients were also more likely to experience adverse eects than placebo recipients. However, there was no evidence of an increase in CNS-related eects with rimantadine and withdrawal rates were similar in both groups (Table 6).
Two minor comparisons, G and H, were also carried out, each based on the results of a single trial. For comparisons A, B and C the eects on `cases' were analysed, stratied either on the basis of clinicallaboratory criteria (a dened set of signs and symptoms backed up by serological conrmation and/or isolation of inuenza virus from nasal uids) or clinical criteria alone. The eects of amantadine/rimantadine administration on asymptomatic cases (dened only by serology or viral isolation) were not assessed, as these are of little public health interest. Comparisons were stratied on the basis of whether participants had received vaccination or not. Finally, the adverse eects in the comparisons were assessed. The `all adverse eects' category includes all types and was derived from those trials which either did not report sucient information to allow a more detailed classication or that presented aggregate data. Adverse eects incidence is reported in the meta-analysis as event per person, thus the incidence should not be added as more than one adverse event is likely to have taken place in the same individual during the trial. The dierence in incidence of adverse eects is of importance, rather than the estimated incidence itself, as the adverse eects reported with these drugs are very similar to the clinical manifestations of inuenza infection. Apart from these caveats the analysis shows that all types of adverse events were signicantly more likely to happen when individuals were given amantadine rather than placebo (with the exception of the `other' category) but none were signicantly more likely to
V. Demicheli et al. / Vaccine 18 (2000) 9571030
975
Fig. 3. Oral amantadine compared to placebo in inuenza prevention: inuenza cases clinically dened (Expt=experimental arm, ctrl=control arm; 95%CI=95% Condence intervals).
3.3.3. Comparison C oral amantadine compared to oral rimantadine in inuenza prevention 3.3.3.1. Ecacy. There was no evidence of a dierence in ecacy between amantadine and rimantadine, although the condence interval is quite wide (RR amantadine vs rimantadine 0.88. 95%CI: 0.481.63). In some cases (Plesnik) data on cases of inuenza have been included both under clinically and serologically dened, so the two outcomes should not be added. 3.3.3.2. Adverse events. CNS adverse eects and withdrawal from trials was more signicantly common among amantadine recipients than rimantadine recipients (CNS eects; RR 2.58, 95%CI: 1.544.33; withdrawals RR 2.30, 95%CI: 1.234.30).
Thus rimantadine appears no less ecacious but safer than amantadine in preventing cases of inuenza in healthy adults, although the study sizes of the safety trials of rimantadine are considerably smaller than those of amantadine.
3.3.4. Comparison D oral amantadine compared to placebo in inuenza treatment 3.3.4.1. Ecacy. Amantadine signicantly shortened duration of fever compared to placebo (by 1.00 days 95%CI: 0.731.29). The meta-analysis is based on 506 subjects (230 in the amantadine and 276 in the placebo arm). Where time to fever clearance data were not available (van Voris and Wingeld), a dichotomous outcome was used (cases with fever at 48 h).
Table 5 Comparison A: Incidence of adverse eects expressed as a percentage of participants Amantadine (%) All adverse eects GI eects Increased CNS activity (excitation) Decreased CNS activity (depression) Skin 14.7 5.1 7.5 8.6 1.1 Placebo (%) 10.4 2.4 4.7 7.1 6.8 No. of trials 6 5 9 6 4 N 4274 3336 5002 3782 918 Signicant Yes Yes Yes Yes No
976
V. Demicheli et al. / Vaccine 18 (2000) 9571030
Fig. 4. Oral rimantadine compared to placebo in inuenza prevention: inuenza cases clinically dened (Expt=experimental arm, ctrl=control arm; 95%CI=95% Condence intervals)
Amantadine was shown to be signicantly better than placebo (Peto relative risk 0.21 95%CI: 0.070.66). 3.3.4.2. Adverse events. In contrast to the increased adverse eect rates for prevention, there was no evidence that amantadine recipients had increased adverse eect rates to placebo recipients. The incidence of adverse eects by comparison expressed as a percentage of participants is shown in Table 7.
3.3.5.2. Adverse events. There were very little data available for the assessment of adverse eects of rimantadine for treatment (45 participants) (Table 8). 3.3.6. Comparison F oral amantadine compared to oral rimantadine in inuenza treatment 3.3.6.1. Ecacy. The little data available directly comparing amantadine and rimantadine for treatment showed that the ecacy of the two drugs was comparable, although condence intervals are very wide. 3.3.6.2. Adverse events. There were very little data available for the assessment of adverse eects of the direct comparison between amantadine and rimantadine (33 participants). A meta-analysis of the symptoms outcome data was considered to further inform the assessment of the eects of amantadine and rimantadine in a treatment
3.3.5. Comparison E oral rimantadine compared to placebo in inuenza treatment 3.3.5.1. Ecacy. Rimantadine also signicantly shortened duration of fever compared to placebo (by 1.27 days 95%CI: 0.771.77). There was a signicantly higher number of afebrile cases 48 h after commencing rimantadine treatment (RR=0.17; 95%CI: 0.040.74).
Table 6 Comparison B: Incidence of adverse eects expressed as a percentage of participants Rimantadine (%) All adverse eects GI eects Increased CNS activity (excitation) Decreased CNS activity (depression) Skin 18.6 9.0 6.5 9.6 0 Placebo (%) 10.8 2.2 4.3 1.0 0 No of trials 3 2 3 1 N 558 357 652 228 Signicant No Yes No No
V. Demicheli et al. / Vaccine 18 (2000) 9571030 Table 7 Comparison D: Incidence of adverse eects expressed as a percentage of participants Amantadine (%) GI eects Increased CNS activity (excitation) Decreased CNS activity (depression) Skin 13.8 3.5 56.4 0.9 Placebo (%) 13.4 5.0 65.2 0.4 No. of trials 3 2 3 2 N 494 475 491 465
977
Signicant No No Yes No
role. When the outcome typology was tabulated it was discovered that such a meta-analysis would be impossible (Table 9). We resorted to using duration of fever (dened as a temperature greater than 378C) as the only common outcome. One drawback of this approach is the possible confounding eect of the presence of fever for a variable length of time prior to and after entry to the study (and hence at the moment of commencement of treatment). However if random allocation had been properly carried out, this eect should disappear. 3.3.7. Comparison G oral amantadine compared to oral aspirin in inuenza treatment In Comparison G, based on Younkin, aspirin was signicantly more eective than amantadine in reducing the length of fever (by 0.47 days 95%CI: 0.17 0.76). This observation is based on 29 individuals. Aspirin is well known for being a very eective antipyretic and anti-inammatory drug, however it does not inhibit viral replication and as such remains a symptomatic remedy. 3.3.8. Comparison H inhaled amantadine compared to placebo in inuenza treatment In comparison H (based on Hayden's 1980 trial) inhaled amantadine was no more ecacious than placebo in bringing down the respiratory or constitutional symptom score (Weighted Mean Dierence 1.0 95%CI: 3.641.64 and 2.0 95%CI: 16.912.9 respectively). This comparison also is based on small numbers of participants (20). Not surprisingly, amantadine caused signicantly more nasal irritation (RR
6.11 95%CI: 0.8643.3). Inhaled amantadine does not appear to be particularly eective but has a high incidence of local adverse eects which would make compliance dicult. The interpretation of Comparisons G and H is made dicult by the small numbers involved and the presence of single trials. 3.4. Eects of NIs When compared to placebo, NIs are 55% (95%CIs: 2971%) eective in preventing naturally occurring cases of laboratory conrmed inuenza and 67% eective (95%CIs: 908%) in experimental inuenza when given intravenously. Overall NIs are 60% eective (95%CIs: 7633%) (Fig. 5). When the outcome is dened as cases of serologically conrmed inuenza, NIs are 74% eective (95%CIs: 5087%) in preventing naturally occurring inuenza and 86% eective (95%CIs: 1298%) in preventing experimentally induced inuenza. Overall they are 76% eective (95%CIs: 5587%) in preventing cases of laboratory conrmed inuenza. Both compounds appear safe, but as yet no direct comparisons have been carried out, so there can be no comment upon their relative eects. The adverse event prole (local nasal irritation) of Zanamivir appears little dierent to placebo (OR 1.19 95%CIs: 0.393.62). However this may be due to the relatively small denominator (112 individuals). Oseltamivir appears to have a signicantly higher incidence of systemic adverse eects than placebo (OR 1.68 95%CIs: 1.142.49).
Table 8 Comparison E: Incidence of adverse eects expressed as a percentage of participants Rimantadine (%) GI eects Increased CNS activity (excitation) Decreased CNS activity (depression) Skin 28.6 0 Placebo (%) 28.6 8.3 No of trials 0 1 1 0 N 0 14 31 0 Signicant No No
978 Table 9 Comparison F: Outcome typology by study Trial Galbraith 1971 Hayden 1980 Hayden 1986 Hornick Kitamoto 1968 Kitamoto 1971 Knight Togo Younkin Van Voris Wingeld
V. Demicheli et al. / Vaccine 18 (2000) 9571030
Symptom outcomes used Average time to clearance of symptoms Aggregate scores of systemic and respiratory symptoms Aggregate scores of systemic and respiratory symptoms Percentage of patients in three symptoms clearance time periods No symptoms No symptoms Between arms symptoms concordance. Aggregate data only Percentage of patients in three symptoms clearance time periods Signicance of the dierence of symptoms scores Percentage improvement of symptom scores at dierent time periods Signicance of dierence of proportions of patients in three symptoms clearance time periods
Each comparison should be read and interpreted separately from sub-comparisons because of the likelihood of double counting (when the same data appears more than once). When transforming the data for inclusion in the meta-analysis several assumptions were made. For instance in the case of Hayden, 1996b, the medians were transformed into means and SDs derived from ranges. To assess the safety prole of Oseltamivir (the NI compound for which the best detailed information was held) a comparison between amantadine, rimantadine and Oseltamivir was carried out (Table 10). The adverse eect `dyspepsia' in the amantadine and rimantadine trials includes nausea. The adverse eect `nausea' in the RO trials only includes nausea (Table 11). The comparison Rimantadine/Oseltamivir appears
sounder than Amantadine/ Oseltamivir because of the signicantly dierent incidence of adverse eects in the placebo arms. The likely explanation of the dierence in incidence in the placebo arms is due to dierences in denition and classication of adverse events within the original amantadine trials (which date back to the 1960s and 1970s). Consequent pooling of data and comparisons with Oseltamivir is unlikely to be methodologically acceptable. Compared with rimantadine in a preventive role, Oseltamivir (RO for short) has a signicantly lower incidence of adverse eects and signicantly higher incidence of nausea. In a treatment role, NIs shorten the duration of symptoms by one day (Weighted Mean Dierence WMD1 95%CIs: 1.3 to 0.6) for clinically dened inuenza cases, and by nine tenths of one day (WMD
Fig. 5. Neuraminidase inhibitors compared to placebo in inuenza prevention: inuenza cases laboratory dened (Expt=experimental arm, ctrl=control arm; 95%CI=95% Condence intervals).
V. Demicheli et al. / Vaccine 18 (2000) 9571030
979
Table 10 Percentage incidence of adverse eects in amantadine (ama), rimantadine (rima), Oseltamivir 75 mg (daily in prevention and twice daily in treatment) compared to placebo (pl) Comparison Amantadine (ama) Placebo (pl) P value Rimantadine (rima) Placebo P value Oseltamivir 75 mg Placebo P value Ama vs Oseltamivir P value Rima vs Ro P value Pl ama vs Pl Oseltamivir P value Pl rima vs Pl Oseltamivir P value Prevention All adverse eects 14.8% 9.9% 0.0001 32% 19.5% 0.03 23.8% 18.9% 0.05 0.0000 0.03 0.0000 0.9 Treatment Nausea/dyspepsia 3.4% 1.1% 0.0003 5.2% 2.6% 0.49 13.7% 7.3% 0.0008 0.0000 0.01 0.000 0.06 Treatment All adverse eects 14.5% 14.2 0.9 1.7% 5.7% 0.002 0.0000 0.0001
-0.9 95%CIs: 1.6 to 0.1) for laboratory dened inuenza cases. The time gained in returning to normal activities is a half day (WMD 0.5 95%CIs: -1.1 to 0.1) for laboratory conrmed inuenza cases. Thus in the latter comparison NIs fare no better than placebo. The adverse event prole shows that gastrointestinal symptoms are signicantly worse in NIs than placebo (Peto OR 2.32 95%CIs: 1.553.47) and overall 2.59 (Peto OR 2.59 95%CIs: 1.594.21). Upper respiratory tract and local nasal symptoms are no worse than placebo although these comparisons are based on small denominators. 3.5. Results of the economic evaluation Tables 12 and 13 present the basic values of the model, the ranges across which these have been varied and the results of our calculations. We did not adjust our results for time as inuenza is a yearly disease and both immunity to previous circulating strains and vaccine compositions vary from year to year. Our results
show that in healthy adults, vaccines appear the best buy, except in the most extreme scenario of high eectiveness, minimum adverse events and minimum duration of chemoprophylaxis (Table 12). In this case amantadine has the lowest incremental cost per case avoided (7). The weighted costs for vaccines are always negative (i.e. it is better to do nothing), while costs for chemoprophylaxis become positive only at the highest levels of incidence (150 per 1000 population for NIs and 200 per 1000 population for antivirals).
4. Discussion 4.1. Inuenza vaccines Parenterallyadministered inuenza vaccines appear signicantly better than their comparators, and can reduce the incidence of serologically conrmed inuenza by around 50%, if the WHO recommendations are adhered to. However, whilst the vaccines do prevent inuenza A, that is only one part of the spectrum of
Table 11 Summary of percentage incidence of adverse eects in amantadine, rimantadine, Oseltamivir 75 mg Incidence Amantadine Rimantadine Oseltamivir 75 mg Prevention All adverse eects (%) 14.8 32 23.8 Nausea/Dyspepsia (%) 3.4 5.2 13.7 Treatment All adverse eects (%) 14.5 1.7
980
V. Demicheli et al. / Vaccine 18 (2000) 9571030
Table 12 Values of variables used in the basic model and in the sensitivity analysis Variable Population Incidence of inuenza Eectiveness of parenteral inactivated vaccine (denominator size=6566) Eectiveness of amantadine Eectiveness of NI Adverse eects of vaccine (tenderness) Adverse eects of antiviral (GI) Adverse eects of NI (nausea) Individual preferences Nausea & inuenza=0.95 Preventive intervention: Vaccine unit cost Preventive intervention: Antiviral unit cost Preventive intervention: NI unit cost Duration of treatment for antivirals and NIs Preventive intervention administration costs for vaccine Preventive intervention administration costs for antiviral and NI Basic value 110,000 5.7 per 1000 0.21 0.23 0.74 0.57 0.05 0.11 Complete well being=1 25th and 75th percentiles scores of preferences expressed as a combination of category rating and time-trade-o 1997 3.36 1998 0.20 per 100 mg tablet 1998 6 62 days Nil Nil Values in the sensitivity analysis 110,000 5.7 per 1000400 per 1000 0.120.29 (95%CI: for clinical case denition) 0.48 0.79 for laboratory case denition) 0.110.34 (95%CI: for clinical case denition). From 0.420.76 (95%CI: for laboratory case denition) 0.500.87 (95%CI: for clinical case denition). From 0.370.65 (95%CI: for laboratory case denition) 0.100.57 0.020.05 0.050.11
Not tested Not tested Not tested 11 days122 days 2.9 times vaccine costs 2 times drug costs
`clinical inuenza', the parenterally administered vaccines only reducing total clinical inuenza rates by 24%. Live aerosol vaccines appear of little practical use given their relatively low eectiveness. Results regarding inactivated aerosol vaccine are based on analysis of two studies reporting only clinical outcomes and not directly comparable owing to non-
homogeneous denitions. Therefore conclusions have not been drawn from these data. Rates of complications caused by inuenza in these trials were very low, and analysis of the few trials which contained this outcome did not reveal a signicant reduction with inuenza vaccine. This result appears in contrast with the conclusions reported in
Table 13 Results of cost-eectiveness analysis (cost per avoided case in 1998 Pounds Sterling by assumption and intervention) Vaccine Basic assumptions Eectiveness high Eectiveness low Maximum duration of NIs and amantadine chemoprophylaxis Minimum duration of NIs and amantadine chemoprophylaxis Inclusion of administration costs Highest incidence Highest incidence and highest eectiveness Highest incidence and lowest eectiveness Highest incidence, highest eectiveness and minimum duration of chemoprophylaxis 2807 746 4912 2807 2807 8140 40 11 70 11 Amantadine 9458 2862 19,777 18,612 1678 18,917 135 41 282 7 NI 88,193 75,015 176,387 173,542 15,647 176,387 1257 1069 2514 190
V. Demicheli et al. / Vaccine 18 (2000) 9571030
981
the literature regarding elderly people, probably due to the general rarity of complications caused by respiratory infection in healthy adults. Hospitalisation was assessed only in one trial, and showed a signicant benet from vaccination. Working days lost in placebo recipients and vaccine recipients were signicantly reduced in the vaccinated group, but by less than half a day on average. Safety does not appear to be a particular problem with any of the vaccines, either for incidence or severity, although given the low eectiveness of the aerosol vaccines, the eects classied as adverse may be caused by inuenza. Either way, the public health safety prole of the vaccines is acceptable. The results of this review seem to discourage the utilisation of vaccination against inuenza in healthy adults as public health measure. Having healthy adults at low risk of complications due to respiratory disease, the use of the vaccine may be only advised as individual protection measure in very specic cases. The major dierences in eect size between outcomes highlight the need for careful consideration of the best study design to assess the eects of public health measures such as vaccines. Additionally more work needs to be carried out on the combined use of vaccines, antivirals and NIs when licensed. 4.2. Amantadine and rimantadine The results of the review show that both amantadine and rimantadine are ecacious and relatively safe in prevention and treatment of cases of inuenza A. The role of amantadine in prophylaxis (61% eective) and treatment (shortens duration of illness by one day) is beyond question and does not need to be investigated further compared to placebo. Rimantadine appears equally ecacious in prevention (72%), but in direct comparison with placebo, when a random eects model is applied the lower bound of the 95%, condence does not achieve statistical signicance. Two connected explanations for this nding may be given: the rst is that of insucient numbers (there are clinical data for approximately 700 rimantadine and 2500 amantadine recipients in the review). The second explanation is centred on the methods of statistical analysis used: the dierence between rimantadine and placebo for the prevention of clinically and serologically dened inuenza cases is highly signicant if a xed eect model is used (RR 0.36, 95%CI: 0.220.59). It is likely that with more clinical data available the eectiveness of rimantadine would be beyond doubt. Rimantadine is equally therapeutically ecacious, shortening duration of fever by just over one day. However, again, this observation is based on 54 patients
only. There do not appear to be signicant dierences in eectiveness in either roles between the two compounds, although again the comparisons are based on small numbers with large condence intervals. The safety prole of the two drugs appears however signicantly dierent; with rimantadine causing signicantly fewer CNS adverse eects than amantadine (being no dierent than placebo) and causing fewer withdrawals from the trials. Although these observations are based on smaller numbers of rimantadine recipients, amantadine denitely causes signs of signicantly increased and decreased CNS activity, an eect which is not easily acceptable by healthy adults, especially in employment which require concentration and mental tness. The conclusion may be drawn that from available evidence, rimantadine appears the better choice for prevention. Signicantly decreased CNS activity is caused by amantadine in a treatment role, but this appears to be the only signicant adverse eect of both compounds in a treatment role, although numbers of patients are again very low. Low numbers make the interpretation of the other two comparisons equally dicult. In future more attention should be paid to the assessment of adverse events of the two compounds, particularly those of rimantadine which at present are based on relatively small numbers. The quality of the trials was not good, with signicant numbers of studies failing to give adequate descriptions of methods and of results. This may be in part due to the number of older trials in the review. Both quality of trial conducting and reporting should be improved and adverse eects and case outcome denitions should be standardised. No trials assessed onset of resistance, but data from a review citing two studies demonstrated that 10 to 27% of patients treated with rimantadine secreted drug-resistant virus within four to ve days of commencing treatment [37]. Finally, carrying out subanalysis by dose was considered (100, 200, 300 mg daily), but decided against this given the small size of the resulting meta-analysis. This policy will be re-considered if any further data become available. Both drugs can be used eectively for the prevention and treatment of inuenza, both in vaccinated and unvaccinated populations. However, the higher incidence of CNS adverse eects of amantadine makes rimantadine the current antiviral of choice against inuenza. There is a requirement for better reported trials, particularly those assessing amantadine and rimantadine directly in both prevention and treatment roles. Attention should be paid to the assessment of adverse events of the two compounds, particularly those of
982
V. Demicheli et al. / Vaccine 18 (2000) 9571030
rimantadine which at present are based on relatively small numbers. Quality of trial conducting and reporting should be improved and adverse eects and case outcome denitions should be standardised. 4.3. Neuraminidase inhibitors As far as is known by the authors, this review provides the most comprehensive current evidence of the eects of NIs on humans exposed to inuenza either naturally or experimentally. The results of the metaanalysis show that NIs are eective in preventing inuenza A and B and shortening duration of illness. The safety prole of the compounds is good overall, although there is concern about the acceptability of Oseltamivir given the high incidence of nausea it causes. Further assessment of the safety of this compound is necessary. As increasing amounts of data become available (as can be seen by the number of studies awaiting assessment following publication) the review will be updated and further comparisons added. These are likely to include direct comparisons between compounds, and comparisons of dierent doses and schedules. Overall the quality of trials was dicult to assess as a proportion of trials were either in an unpublished or an abstract format. The quality of the two published studies was reasonable. As NIs have a clear eect, it is now time to concentrate on more pragmatic trials in individuals exposed to naturally acquired inuenza. 4.4. Overall comments Overall the evidence that we assembled in our Cochrane reviews was based on relatively small denominators. For instance, the parenteral inactivated vaccine trials meta-analysis is based on 16 studies with a total of 23,000 individuals. The trials were carried out worldwide over a 30-year time span during which, assuming a low incidence of ve per 1000, there would have been over eight million cases of inuenza in the UK alone. We do not know whether such trial size is sucient to properly evaluate an intervention (vaccines) which could be given yearly to large cohorts world-wide for a very common infectious disease, especially since the vaccine is eectively a new product each year. Many of the 17 antiviral trials did not report adverse events, thus our evaluation of the crucial safety prole of these was based on ve studies with a total of approximately 3000 individuals. Again the overall knowledge base may be insucient to reach rm conclusions in this most important aspect of quality. There is a notable dierence between eect size on clinically-dened outcomes and those based on a lab-
oratory-conrmed case denition. This is likely to be caused by a high intervention ecacy against the inuenza virus, which is equivalent to a low eectiveness in the context of an inuenza epidemic. This in turn raises the problem of whether RCTs are the best design to assess the eectiveness of public health measures such as vaccination. We are aware that the alternatives (context-specic non-randomised studies) are prone to confounders and hence problems of interpretation of results. 4.5. Economic evaluation By taking the perspectives of eectiveness, safety and eciency into account in the evaluation of the eects of prevention and treatment of inuenza, we were able to assess the relative importance of each perspective in answering the study question. By basing our economic model on systematically assembled and evaluated evidence we reached relatively rm conclusions. The rst eect of such a methodological approach was to prune our decision tree considerably; thus the treatment arms were deleted because of the small eect size. Our tree went from a `before' state of a prevention/treatment combination leading to 11 decision nodes and 165 terminal nodes to an `after' state of preventive alternatives only with one decision node and 12 terminal nodes. Although antivirals and NIs signicantly shortened the duration of illness when compared to placebo (0.5 to one day), this eect had little practical signicance. However, the use of systematic review methods to dene comparators had the drawbacks of discarding data because of inappropriate format and of reliance on what data were available. One of the consequences of the latter drawback is the impossibility of evaluating the use of NIs in local outbreak control situations. A consequence of the former was the exclusion from the decision-making process of all trials with inappropriate outcome measures. We were able to exclude inhaled or live attenuated vaccines from our evaluation because of little eect or little dierence in eect with parenteral vaccines. Of the remaining contenders, rimantadine is not licensed in the UK but has a better safety prole than amantadine (which is available in UK). As physicians we would not recommend the use of amantadine in healthy adults, given the high incidence of major CNS excitant and depressant adverse eects seen in our Cochrane meta-analysis [8]. Such adverse eects are likely to prove very dangerous in healthy adults, especially those undertaking emergency service duty during an inuenza outbreak. Despite this nding that ruled out the use of amantadine, we decided to keep amantadine in our model and
V. Demicheli et al. / Vaccine 18 (2000) 9571030
983
used its less frequent GI adverse eects, broadly comparable to those of NIs. From a GI point of view however, amantadine has a better safety prole that rimantadine. As rimantadine's eects on the CNS are no dierent than those of placebo, rimantadine would be considered a better candidate as a comparator were it registered in the UK. However when the likely duration of treatment is taken into consideration (62 days), the probable logistic burden and compliance problems of compounds to be administered daily (such as antivirals and NIs) make them an unpractical choice. The only remaining intervention, vaccines, should then become the solution to our study problem. Thus the economic evaluation was a posteriori made redundant by evidence of eects which ruled out all the alternatives. Had we built our economic model using an a priori conceptual framework and had we fed it estimates derived from single studies of the relevant interventions, it is likely that we would have retained a very complicated decision tree with many dierent alternatives and reached a dierent conclusion. If assessed from an eectiveness and eciency point of view, vaccines are undoubtedly the best preventive means for inuenza in healthy adults. However when safety and quality of life considerations are included, parenteral vaccines have such low eectiveness and high incidence of trivial local adverse eects that the trades-o are unfavourable. This is so even when the incidence of inuenza is high and adverse eect quality of life preferences are lowly rated. We reached similar conclusions for antivirals and NIs even at high inuenza incidence levels. We conclude that the most cost-eective option is not to take any action. We believe that our methods are applicable to other healthy adult population groups with several caveats. The costs of administration of a preventive programme and indirect costs of interventions (time spent being vaccinated or taking medication) would need to be carefully valued in a non-military population.
Individual preferences would have to be assessed in the reference population. The impact of inuenza diers on the basis of sickness certication patterns that are specic to employment groups. However problematical the economics of inuenza prevention are, these pale into insignicance when compared to the uncertainty still surrounding epidemiological knowledge of the disease and of its consequences and remedies. Acknowledgements This study was funded by the Ministry of Defence of the United Kingdom (MOD(UK)). Inuenza vaccines in healthy adults The authors gratefully acknowledge the help received by Drs Brian Hutchison, Alan Hampson, Andy Oxman and Donatella Tiberti for data extraction and Mrs Carol Hobbs for assistance with trial retrieval. Amantadine and Rimantadine for inuenza in healthy adults The authors would like to thank Drs Aoki, Couch, Hayden, and Monto for helpful comments on the draft protocol and Mrs Carol Hobbs for assistance with trial retrieval. Neuraminidase inhibitors for inuenza in healthy adults The authors would like to thank Professor Arnold Monto, Drs Penelope Ward, Bina Rawal for the help received and Mrs Carol Hobbs for assistance with trial retrieval. Economic evaluation The authors gratefully acknowledge the assistance given by the editorial base of the Cochrane Acute Respiratory Infections Group to the Cochrane reviews and by Stephen Morris. The authors also gratefully acknowledge the extensive editorial assistance given by Ms Elizabeth Hayden and Dr Abraham Palache. Potential conict of interest Dr Jeerson is an ad hoc consultant for Homann-La Roche Ltd.
984
V. Demicheli et al. / Vaccine 18 (2000) 9571030
Appendix A. Producers of inuenza vaccines and their products [7] Country Australia Bulgaria Canada France Germany Germany Hungary Italy Italy Italy Japan Japan Japan Japan Korea Korea Korea Korea Korea Korea Korea Netherlands Romania Romania Russian Federation Russian Federation Russian Federation Russian Federation Slovakia Switzerland UK USA USA USA Yugoslavia Producer CSL Ltd MA Research Institute of Infectious and Parasitic Diseases IAF BIO Va. Inc. Pasteur-Merieux Serums & Vaccines Behringwerke Aktiengesellischaft Veb Sachsisches Serumwerk Dresen Omnivest Institute BIOCINE spa Istituto Sieroterapico Italiano spa Istituto Vaccinogeno Pozzi spa Denka Seiken Co. The Chemo-Sero-Therapeutic Research Institute The Kitasato Institute The Research Foundation for Microbial Diseases of Osaka University Boryung Biopharma Co. Cheil Foods and Chemicals Inc. Dong Shin Pharmaceutical Co Ltd DongA Pharmaceutical Co Ltd Korea Green Cross Corporation Korea Vaccine Co Ltd LG Chemical Ltd Solvay Pharmaceuticals bv Cantacuzino Institute Stefan S Nicolau Institute of Virology Bacteriological preparations division of the St Petersburg Institute for Vaccine and Serum Research Immunopreparat Irkutsk Bilogical Preparation Company Pasteur Institute St Petersburg Imuna sp. Swiss Serum and Vaccine Institute Berne Evans Medical Connaught Laboratories Inc. Parke Davis Wyeth Laboratories Inc. Institute of Immunology and Virology Torlak Product type Split virion Live vaccine Trivalent whole virion, split virion Whole virion, split virion Split virion liquid Split virion Inactivated Whole virion, subunit virion Whole, split and subunit virion Whole, split and subunit virion Whole virion Whole virion Whole virion Whole virion Whole virion Whole virion Whole virion Whole virion Whole virion Whole virion Whole virion Whole virion, subunit virion Whole virion, split virion Whole virion Live intranasal, whole virion Whole virion Intranasal Whole virion Subunit virion Whole virion Subunit virion Subunit virion, whole virion Subunit virion, whole virion Subunit virion Whole virion
V. Demicheli et al. / Vaccine 18 (2000) 9571030
985
Appendix B. Questionnaire used to assess trial design quality and results, as inclusion criteria for systematic review 1. Generation of allocation schedule Did the author(s) use: Random number tables: Computer random-number generator: Coin tossing: Shuing of allocation cards: Any other method which appeared random: 2. Concealment of treatment allocation Which of the following was carried out: There was some form of centralised randomization scheme where details of an enrolled participant were passed to a trial oce or a pharmacy to receive the treatment group allocation: Treatment allocation was assigned by means of an on-site computer using a locked le which could be accessed only after inputting the details of the participant: There were numbered or coded identical looking vials (or ready-drawn syringes) which were administered sequentially to enrolled participants: There were opaque envelopes which had been sealed and serially numbered utilised to assign participants to intervention(s): A mixture of the above approaches including innovative schemes, provided the method appears impervious to allocation bias: Allocation by alternation or date of birth or case record or day of the week or presenting order or enrolment order: 3. Exclusion of allocated participants from the analysis of the trial Did the report mention explicitly the exclusion of allocated participants from the analysis of trial results?: If so did the report mention the reason(s) for exclusion?: 4. Measures to implement double blinding Did the report mention explicitly measures to implement and protect double blinding? Did the author(s) report on the physical aspect of vaccinationi.e. appearances, colour, route administration)? Measure(s) taken to conceal treatment allocation were assessed as follows: yes/no yes/no yes/no yes/no (if yes, specify) yes/no yes/no yes/no yes/no yes/no yes/no yes/no yes/no yes/no yes/no yes/no (specify)
Category A: adequatein the following circumstances: . there was some form of centralised randomization scheme where details of an enrolled participant were passed to a trial oce or a pharmacy to receive the treatment group allocation. Alternatively treatment allocation could have been assigned using an on-site computer using a locked le which could be accessed only after inputting the details of the participant. . there were numbered or coded identical looking tablets or spray devices which were administered sequentially to enrolled participants; . a mixture of the above approaches including innovative schemes, provided the method appears impervious to allocation bias. Category B: inadequatein the following circumstances: . when alternation, date of birth, case record, day of the week, presenting order, enrolment order etc. were used. . when an open system of random numbers or assignments was used. Category C: unclearin the following circumstances: . when only terms such as `lists' or `tables' or `sealed envelopes' or `randomly assigned' were mentioned in the text. in all other circumstances where a prospective trial using intervention or placebo assignments were mentioned without specifying the method of allocation.
986
Appendix C. Characteristics of included studies Description of studies included in the Vaccine Review Study and reference Eddy Eddy, T.S. and Davies, N.A. The eect of vaccine on a closed epidemic of Hong Kong inuenza. South African Medical Journal 1970, 21, 214216. Methods South African CCT: 1254 subjects took monovalent inactivated and 413 received placebo. Controls were selected using a 1-in-4 systematic sample from a ranked list of personnel numbers. `Double blinding' was not mentioned, but the control group received an injection of `dummy vaccine'. Each arm counted 975 and 878 subjects for adverse eects; 933 and 841 subjects for symptoms dened cases. Participants 1758 healthy male Bantu employees aged 1865, housed in a large factory in the Western Cape. 91 failed to appear for vaccination and were excluded from the experiment. Interventions Monovalent inactivated: A2/Aichi/2/68 (Hong Kong variant) administered subcutaneously. Placebo: sterile water. Outcomes Clinical cases of `inuenza' (no better dened) and inpatient days. First clinical case of inuenza appeared on May, 21 1969; the last 6 weeks later. All ill persons were admitted to hospital; no denition of inuenza-like illness was given. Notes Outbreak was due to an A2/Hong Kong/68 virus. The recommended monovalent vaccine for that year in the USA was A2/Aichi/2/68. The vaccine strain was considered to be recommended and matching the circulating strain.
V. Demicheli et al. / Vaccine 18 (2000) 9571030
Edmonson Edmonson, K.W., Graham, S.M. and Warburton, M.F. A clinical trial of inuenza vaccine in Canberra. Medical Journal of Australia 1970, 4, 613.
1983 healthy volunteers (1284 males, 699 females) from amongst Canberra public servants.
Bivalent vaccine (inuenza A and B) containing A2/N.T./ 60/68 (8000 HA units) and B/Victoria/ 2/65 (3000 HA units) strains, against a monovalent B vaccine containing a B/ Victoria/2/65 (3000 HA units) strain. Vaccines were administered by injection in two doses 20 days apart.
Clinically dened cases, working days lost and adverse eects. Sick leave records were considered to classify diagnoses: inuenza, other respiratory diseases, injuries and all other illnesses. Local adverse eects were minimal (when not aecting activities), mild (discomfort when the arm was used; redness, swelling but no absence from work) or severe (causing absence from work). Systemic adverse eects were minimal, mild (interference with normal activities but no absence from work) or severe.
Conducted during the winter of 1969. Epidemic period length is unknown but probably comprises whole follow-up period. The circulating virus, isolated from patients, was A2/H.K./68. The monovalent vaccine recommended for that year in the USA was A2/ Aichi/2/68. The vaccine strain was considered to be recommended and matching the circulating strain.
Edwards 1 Edwards, K.M., Dupont, W.D., Westrich, M.K. et al. A randomized controlled trial of cold adapted and inactivated vaccines for the prevention of inuenza A disease. Journal of Infectious Diseases 1994, 169, 6876.
RCT conducted in USA. Subjects recruited from seven organisation and assigned to a study group using a permuted block randomisation scheme stratied by treatment centre and age group. Double blind.
5210 healthy children and adults of metropolitan Nashville aged 15
Data extracted and loaded: Edwards 1: 198687 outbreak; live cold adapted against placebo; 872 treated, 439 placebo. Cold adapted: Texas/ 1/85 H1N1 and Bethesda/1/85 H3N2 (107107,6 pfu/ml); placebo: allantoic uid.
Clinical and laboratory conrmed cases and adverse eects. Inuenza like illness dened as fever or abrupt onset with rone of: chills, headache, malaise, myalgia, cough, pharyngitis, other respiratory complaints, and presented for throat culture (positive illness dened by presence of inuenza A virus). Retrospectively reported illness: stating at time of spring blood sampling that they had an inuenza-like illness the previous winter. Seroconverted: fourfold rise in titre from postvaccination to spring sera for inuenza A virus circulated that season. Side eects were those experienced by all subjects vaccinated in the ve-year study. Local adverse eects: redness, induration, tenderness. Systemic adverse eects: fever, sore throat, coryza, lethargy, chills, nausea, headache, muscle ache, cough.
Circulating virus: Taiwan/1/86 (antigenic drift from vaccine strain). Epidemic period 56 days. The WHO recommended vaccine for that year contained A/ Chile/1/83, A/Singapore/ 6/86, A/Mississipi/1/85 and B/Ann Arbor/1/86. The A strains administered in the study matched the recommended ones.
V. Demicheli et al. / Vaccine 18 (2000) 9571030 987
Edwards 2 Edwards, K.M., Dupont, W.D., Westrich, M.K. et al. A randomized controlled trial of cold adapted and inactivated vaccines for the prevention of inuenza A disease. Journal of Infectious Diseases 1994, 169, 6876. Edwards 3 Edwards, K.M., Dupont, W.D., Westrich, M.K. et al. A randomized controlled trial of cold adapted and inactivated vaccines for the prevention of inuenza A disease. Journal of Infectious Diseases 1994, 169, 6876.
See Edwards 1
See Edwards 1
Data extracted and loaded: Edwards 2: 198687 outbreak; trivalent inactivated commercial vaccine against inactivated inuenza B vaccine; 878 treated, 439 placebo.
See Edwards 1
See Edwards 1
988 V. Demicheli et al. / Vaccine 18 (2000) 9571030
See Edwards 1
See Edwards 1
Data extracted and loaded: Edwards 3: 198788 outbreak; live cold adapted against placebo; 1029 treated, 532 placebo. Cold adapted: Kawasaki/9/86 H1N1 and Bethesda/1/85 H3N2 (107107,6 pfu/ml); placebo: allantoic uid.
See Edwards 1
Circulating viruses Sichuan/2/87 (H3N2) (antigen drift from vaccine strain) and B/ Victoria/2/87; epidemic period 101 days. The WHO recommended vaccine for that year contained A/Singapore/ 6/86, A/Leningrad/360/ 86 and B/Ann Arbor/1/ 86. Only one of the A strains contained in the study vaccine was recommended.
Edwards 4 Edwards, K.M., Dupont, W.D., Westrich, M.K. et al. A randomized controlled trial of cold adapted and inactivated vaccines for the prevention of inuenza A disease. Journal of Infectious Diseases 1994, 169, 6876.
See Edwards 1
See Edwards 1
Data extracted and loaded: Edwards 4: 198788 outbreak; trivalent inactivated commercial vaccine against inactivated inuenza B vaccine; 1060 treated, 532 placebo. Inactivated vaccine formula: Taiwan/1/86 H1N1 and Leningrad/360/86 H3N2 (15 mg each strain). B strain contained in the vaccines was not described. Data extracted and loaded: Edwards 5: 198889 outbreak; live cold adapted against placebo; 1114 treated, 562 placebo. Cold adapted: Kawasaki/9/86 H1N1 and Los Angeles/2/87 H3N2 (107107,6 pfu/ml); placebo: allantoic uid.
See Edwards 1
See Edwards 1
V. Demicheli et al. / Vaccine 18 (2000) 9571030
Edwards 5 Edwards, K.M., Dupont, W.D., Westrich, M.K. et al. A randomized controlled trial of cold adapted and inactivated vaccines for the prevention of inuenza A disease. Journal of Infectious Diseases 1994, 169, 6876.
See Edwards 1
See Edwards 1
See Edwards 1
Circulating viruses Taiwan/1/86 (H1N1) and B/Yamagata/16/88; epidemic period 78 days. WHO recommended vaccine contained A/ Singapore/6/86, A/ Sichuan/2/87 and B/ Beijing/1/87. Only one of the A strains contained in the study vaccine was recommended. The vaccine was considered to be recommended and matching the circulating strain.
989
Edwards 6 Edwards, K.M., Dupont, W.D., Westrich, M.K. et al. A randomized controlled trial of cold adapted and inactivated vaccines for the prevention of inuenza A disease. Journal of Infectious Diseases 1994, 169, 6876.
See Edwards 1
See Edwards 1
Data extracted and loaded: Edwards 6: 198889 outbreak; trivalent inactivated commercial vaccine against inactivated inuenza B vaccine; 1126 treated, 562 placebo; Inactivated vaccine formula: Taiwan/1/86 H1N1 and Sichuan/2/87 H3N2 (15 mg each strain). B strain contained in vaccines not described. Data extracted and loaded: Edwards 7: 198990 outbreak; live cold adapted against placebo; 999 treated, 508 placebo. Cold adapted: Kawasaki/9/86 H1N1 and Los Angeles/2/87 H3N2 (107107,6 pfu/ml); placebo: allantoic uid.
See Edwards 1
See Edwards 1
990 V. Demicheli et al. / Vaccine 18 (2000) 9571030
Edwards 7 Edwards, K.M., Dupont, W.D., Westrich, M.K. et al. A randomized controlled trial of cold adapted and inactivated vaccines for the prevention of inuenza A disease. Journal of Infectious Diseases 1994, 169, 6876.
See Edwards 1
See Edwards 1
See Edwards 1
Circulating virus Shangai/11/87 (H3N2); epidemic period 80 days. WHO recommended vaccine contained A/ Singapore/6/86, A/ Shanghai/11/87 and B/ Yamagata/16/88. Only one A strain contained in study vaccine was recommended. The vaccine was considered to be recommended and matching the circulating strain
Edwards 8 Edwards, K.M., Dupont, W.D., Westrich, M.K. et al. A randomized controlled trial of cold adapted and inactivated vaccines for the prevention of inuenza A disease. Journal of Infectious Diseases 1994, 169, 6876.
See Edwards 1
See Edwards 1
Data extracted and loaded: Edwards 8: 198990 outbreak; trivalent inactivated commercial vaccine against inactivated inuenza B vaccine; 1016 treated, 508 placebo Inactivated vaccine formula: Taiwan/1/86 H1N1 and Shanghai/11/87 H3N2 (15 mg each strain). B strain contained in the vaccines was not described. A trivalent, subunit vaccine containing 200 IU of A/Victoria/ 3/75, 250 IU of A/ Scotland/840/74 and 300 IU of B/Hong Kong/8/73 (as issued for general use), was compared against placebo (diphtheria and tetanus toxoids). Vaccines were administered subcutaneously.
See Edwards 1
See Edwards 1
V. Demicheli et al. / Vaccine 18 (2000) 9571030
Hammond Hammond, M.L., Ferris, A.A., Faine, S. et al. Eective protection against inuenza after vaccination with subunit vaccine. Medical Journal of Australia 1978, 1, 301303.
Australian CCT, double blind. Coded identical looking vials were sequentially administered to enrolled participants.
225 volunteers, medical students or sta members of the Monash University. 116 subjects in the vaccine group and 109 subjects in the placebo group.
Clinical and laboratory conrmed cases. Inuenza dened as: suffering a respiratory illness associated with the isolation of inuenza virus, a four-fold or greater rise in antibody titre occurred between postvaccination and postepidemic sera, or both. Adverse eects are not considered.
Epidemic inuenza was dened by virus isolation and serology tests and lasted from middle April to middle August 1976. Outcomes were detected during the whole epidemic period. A/Vic/3/75 was isolated from patients. The recommended formula for that year was: A/ Victoria/3/75, A/ Scotland/840/74 and of B/Hong Kong/8/73.
991
Hobson Hobson, D., Baker, F.A., Chivers, C.P. et al. A comparison of monovalent Hong Kong inuenza virus vaccine with vaccines containing only pre1968 Asian strains in adult volunteers. Journal of Hygiene 1970, 68, 369378.
UK RCT comparing monovalent inactivated vaccine of Hong Kong strain of inuenza A virus against polyvalent vaccine containing only pre-1968 Asian viruses. Volunteers allocated to one of three groups by random numbers. Double-blinding maintained throughout trial by coded preparation. Vaccines administered intramuscularly in two groups and placebo (saline) administered nasally. The third group received both vaccines: monovalent nasally; polyvalent intramuscularly.
1601 volunteers, industrial workers aged 1664.
Data extracted and loaded: Polyvalent intramuscular (N = 545) against monovalent intramuscular inuenza A (N = 508) polyvalent formula was: A2/ Eng/12/64 3000 HA units, A2/Eng/76/66 6000 HA units, B/ Eng/5/66 3000 HA units, B/Swiss/265/67 3000 HA units monovalent was a Hong Kong virus: A2/Eng/ 344/68 7000 HA units
Clinical cases and WDLS. Clinical cases were dened as `respiratory illness' or `clinical inuenza' according to the clinical syndromes characterised by StuartHarris (1965).
Epidemic period lasted 10 weeks. Vaccine ecacy was evaluated during the whole 1968 69 inuenza season (23 weeks). The viral strain isolated from patients was antigenically identical to A2/Eng/344/68. The monovalent vaccine recommended for that year in the USA was A2/Aichi/2/68 (a Hong Kong virus). The monovalent A vaccine was considered to be recommended and matching the circulating strain.
992 V. Demicheli et al. / Vaccine 18 (2000) 9571030
Hoskins Hoskins, T.W., Davies, J.R., Allchin, A. et al. Controlled trial of inactivated inuenza vaccine containing the A/Hong Kong strain during an outbreak of inuenza due to the A/ England/42/72 strain. Lancet 1973, 21, 116 120.
Quasi-randomised, double blind, not placebo controlled trial, conducted in a UK boarding school. Boys were allocated to the two arms of the study according to date of birth. The vaccines were labelled according to a code.
800 boys 1119 yearold. 384 subjects received inuenza A vaccine; 340 boys received inuenza B vaccine.
Monovalent inactivated inuenza A vaccine containing the A/Hong Kong/68 strain vs monovalent inactivated inuenza B vaccine. Study lasted three years (197072): boys were re-vaccinated staying in the same vaccine group, and new entrants were allocated as before. Viral strain used in vaccines were:winter 197071: A2/Hong Kong/X31/68 (H3N2) 200 IU and B/ England/5/66 200 IUwinter 197172: A2/Hong Kong/X31/ 68 (H3N2) 200 IU and B/England/5/66 200 IUwinter 197273: A2/Hong Kong/1/68X (H3N2) 200 IU and B/ Victoria/98926/70 200 IU. Each vaccine was given subcutaneously.
Clinical and laboratory conrmed cases and adverse eects. Clinical cases dened as `febrile respiratory infection'. Laboratory cases dened by isolation of an inuenza virus from throat swabs or a fourfold or greater rise in antibody titre occurred between acute and convalescent sera. Reactions to vaccination had insucient denition to be extracted.
The protective ecacy of the vaccines was evaluated during an outbreak of inuenza due to A/England/42/72, a strain which had undergone to a recent antigenic shift. The epidemic period lasted from December 5 to December 15, 1972. The recommended formula for those years in the USA was A2/Aichi/2/68, B/Massachusetts/1/72. The vaccine was considered to match one of the recommended strains.
V. Demicheli et al. / Vaccine 18 (2000) 9571030 993
Keitel 1 Keitel, W.A., Cate, T.R. and Couch, R.B. Ecacy of sequential annual vaccination with inactivated inuenza virus vaccine. American Journal of Epidemiology 1988, 127, 353364.
RCT Volunteers randomly allocated to receive vaccine or placebo using a table of random numbers according to prior vaccination experience. Three groups were formed: rst vaccinated, multivaccinated and placebo. Each arm counted, respectively, 162, 138 and 298 subjects. Double blind.
598 healthy volunteers, 3060 years old, working in the Texas Medical Center in Huston, Texas, or in surrounding industrial companies.
Data extracted and loaded: Keitel 1: 198384 outbreak; trivalent inactivated, killed whole, intramuscularly administered, commercial vaccine against placebo; 300 treated, 298 placebo Each dose of the commercial vaccine contained 15 mg of hemagglutinin of each of the following inuenza strains: A/ Philippines/2/82 (H3N2), A/Brazil/11/ 78 (H1N1) and B/ Singapore/222/79. Placebo was sterile saline for injection.
Clinical and laboratory conrmed cases. Illnesses classied as `any', `u-like' (lower respiratory and/or systemic illness) or `febrile' (oral temperature of r37.8) from ndings at initial examination. Symptoms and signs of disease of trachea, bronchi and/or lung were designated lower respiratory illness. Systemic illness dened by: myalgia, malaise, fatigue, lethargy, chills, sweats and anorexia. Laboratory conrmation was based on culture and/or rfour-fold rise in antibody titre between postvaccination (pre-epidemic), acute, convalescent and/or spring (postepidemic) sera, and is reported separately for inuenza A or inuenza B and for culture or serological positivity. Authors don't specify when culture and serological conrmation are obtained on same subject. Adverse eects are not considered. Outcomes were detected during the whole epidemic period ('interval during which community surveillance recovered inuenza viruses from r10% of person with febrile respiratory illness per calendar week').
The epidemic period was from January 8 to March 17, 1984. Viral strains isolated from cases were A/Victoria/7/ 83 (H1N1) and B/ USSR/100/83. The WHO recommended formula for that year was: A/Brazil/11/78, A/ Philippines/2/82 and of B/Singapore/222/79.
994 V. Demicheli et al. / Vaccine 18 (2000) 9571030
Keitel 2 Keitel, W.A., Cate, T.R. and Couch, R.B. Ecacy of sequential annual vaccination with inactivated inuenza virus vaccine. American Journal of Epidemiology 1988, 127, 353364.
See Keitel 1
See Keitel 1
Data extracted and loaded: Keitel 2: 198485 outbreak; trivalent inactivated, killed whole, intramuscularly administered, commercial vaccine against placebo; 456 treated, 241 placebo Commercial vaccine for fall of 1984 contained 15 mg of hemagglutinin of each of following inuenza strains: A/ Philippines/2/82 (H3N2), A/Chile/1/83 (H1N1) and B/ USSR/100/83. Placebo was sterile saline for injection. Data extracted and loaded: Mair 1: monovalent inuenza A matching circulating strain (N = 85) against monovalent B (N = 155). Vaccine strains were respectively: A/England/42/ 72 (H3N2) (recombinant XPR8, 600 IU), B/Victoria/98926/70 (400 IU).
See Keitel 1
Epidemic period was from January 6 to March 9, 1985. The viral strain isolated from cases was an A/ Philippines/2/82 (H3N2)-like. The WHO recommended formula for that year was: A/ Philippines/2/82 (H3N2), A/Chile/1/83 (H1N1) and B/USSR/ 100/83. The vaccine was considered to be recommended and matching the circulating strain.
V. Demicheli et al. / Vaccine 18 (2000) 9571030
Mair 1 Mair, H.J., Sansome, D.A.W. and Tillett, H.E. A controlled trial of inactivated monovalent inuenza A vaccines in general practice. Journal of Hygiene 1974, 73, 317327.
UK CCT, with allocation by day of birth. Double blind. Compares two monovalent, inactivated, intramuscularly administered inuenza A vaccines against a monovalent inactivated inuenza B vaccine used as placebo.
507 volunteers, patients from general practices. Complete follow up was obtained for 465 of them. Three arms which counted, respectively, 141,169 and 155 subjects.
Clinical and laboratory conrmed cases and adverse eects. Illness dened as `any symptoms of inuenza'. Laboratory conrmation by inuenza virus isolation from throat swabs or four-fold rise in antibody titre between acute and convalescent sera. Local adverse eects were mild (slight swelling, aching) or severe (painful, red and swollen arm). Systemic adverse eects were mild (slight pyrexia, mild aching of back and limbs) or severe (inuenza-like symptoms).
Trial was conducted during the 197273 inuenza season. The follow up period lasted 13 weeks. Authors don't specify the length of the epidemic period. Viral strains isolated from cases was A/England. The recommended formula for that year in the USA was A2/Aichi/2/68, B/Massachusetts/1/72.
995
Mair 2 Mair, H.J., Sansome, D.A.W. and Tillett, H.E. A controlled trial of inactivated monovalent inuenza A vaccines in general practice. Journal of Hygiene 1974, 73, 317327.
See Mair 1
See Mair 1
Data extracted and loaded: Mair 2: monovalent inuenza A matching circulating strain (N = 84) against monovalent A (N = 141). Vaccine strains were respectively: A/England/42/ 72 (H3N2) (recombinant XPR8, 600 IU), A/Hong Kong/1/68 (H3N2) (recombinant X31, 600 IU). Data extracted and loaded: Mair 3: monovalent recommended inuenza A strain (N = 71) against monovalent B (N = 155). Vaccine strains were respectively: A/Hong Kong/ 1/68 (H3N2) (recombinant X31, 600 IU), B/Victoria/98926/70 (400 IU). Data extracted and loaded: Mair 4: monovalent recommended inuenza A strain (N = 70) against monovalent A (N = 169). Vaccine strains were respectively: A/Hong Kong/ 1/68 (H3N2) (recombinant X31, 600 IU), A/England/42/72 (H3N2) (recombinant XPR8, 600 IU).
See Mair 1
See Mair 1
996 V. Demicheli et al. / Vaccine 18 (2000) 9571030
Mair 3 Mair, H.J., Sansome, D.A.W. and Tillett, H.E. A controlled trial of inactivated monovalent inuenza A vaccines in general practice. Journal of Hygiene 1974, 73, 317327.
See Mair 1
See Mair 1
See Mair 1
See Mair 1
Mair 4 Mair, H.J., Sansome, D.A.W. and Tillett, H.E. A controlled trial of inactivated monovalent inuenza A vaccines in general practice. Journal of Hygiene 1974, 73, 317327.
See Mair 1
See Mair 1
See Mair 1
See Mair 1
Maynard Maynard, J.E., Dull, H.B., Hanson, M.L., et al. Evaluation of monovalent and polyvalent inuenza vaccines during an epidemic of type A2 and B inuenza. American Journal of Epidemiology 1968, 87, 148157.
Randomised, not placebo controlled Alaskan trial with no of blinding, comparing a monovalent inactivated inuenza A and a monovalent inactivated inuenza B vaccine against the standard commercial polyvalent AB formulation. All vaccines administered subcutaneously.
502 volunteer students 1418 year-old, not previously immunised. 488 completed the study.
Data extracted and loaded: Standard commercial polyvalent AB formulation (N = 159) against monovalent B (N = 158) polyvalent formula: A/PR8 100 CCA, A1/Ann Arbor/1/57 100 CCA, A2/Jap/170/62 100 CCA, A2/Taiwan/1/ 64 100 CCA, B/ Maryland/1/59 200 CCA. monovalent B: B/Maryland/1/59 400 CCA
Clinical and laboratory conrmed cases. Adverse eects not considered. A case was dened `inuenza-like' with three of: fever, cough, headache, myalgia, sore throat. Serological studies were done on one-third random sample from each of the three groups. Laboratory conrmation seen by four-fold rise in antibody titre between post-vaccination and post-epidemic sera. Throat swabs and acute convalescent sera were collected from a few ill individuals to conrm circulating inuenza virus. Attack rates by vaccine groups were reported for clinical illness during the whole epidemic period.
Protective ecacy of vaccines was evaluated during a simultaneous outbreak of inuenza A and B virus strains, peaking in February and March 1966 respectively. Epidemic period from February 17 to March 18 dened by increase in absenteeism. Circulating strains were B/Alaska/1/ 66 and an A2 virus; both had only minor antigenic variation from B/Maryland and A2/ Taiwan contained in the vaccines. Recommended formula that year in the USA: A/PR8, A1/Ann Arbor/1/57, A2/Jap/170/ 62, A2/Taiwan/1/64, B/ Maryland/1/59 and completely matched the polyvalent vaccine.
V. Demicheli et al. / Vaccine 18 (2000) 9571030 997
Mogabgab 1 Mogabgab, W.J. and Leiderman, E. Immunogenicity of 1967 polyvalent and 1968 Hong Kong inuenza vaccines. Journal of the American Medical Association 1970, 211, 16721676.
Randomised trial, no mention of blinding, carried out in a USA Air Force Base.
Airmen, 1821 yearold, previously unvaccinated.
Data extracted and loaded: Mogabgab 1: monovalent inactivated inuenza A vaccine (A2/Aichi 2/ 68 300 CCA) against placebo (saline treated with formaldehyde solution). Arm sizes: monovalent A (N = 881); placebo (N = 521) Vaccines administered subcutaneously.
Clinical and laboratory conrmed illnesses, complications and admissions. Numbers of illnesses were counted. Adverse eects not considered. All respiratory illnesses classied as febrile (r38.38C), afebrile, pharyngitis, bronchitis or pneumonia (complication). Laboratory conrmation obtained (by culture or 4fold antibody titre increase in acuteconvalescent sera) on 20 men randomly selected each week among illnesses. See Mogabgab 1
Protective ecacy of the vaccines evaluated during the 196869 inuenza outbreak, from December 9 to February 3. Virus isolated from patients was an A2/ Hong Kong and matched the vaccine strain. The monovalent vaccine recommended for that year in the USA was A2/Aichi/2/68. The vaccine strain was considered to be recommended and matching the circulating strain.
998 V. Demicheli et al. / Vaccine 18 (2000) 9571030
Mogabgab 2 Mogabgab, W.J. and Leiderman, E. Immunogenicity of 1967 polyvalent and 1968 Hong Kong inuenza vaccines. Journal of the American Medical Association 1970, 211, 16721676.
See Mogabgab 1
See Mogabgab 1
Data extracted and loaded: Mogabgab 2: Polyvalent inuenza A and B vaccine (1967 military formula A/Swine/33 100 CCA, A/PR8/34 100 CCA, A1/AA 1/57 100 CCA, A2/Taiwan 1/64 400 CCA, B/ Lee/40 100 CCA, B/ Mass 3/66 200 CCA) against placebo (saline treated with formaldehyde solution). Arm size: polyvalent (N = 1030); placebo (N = 521) Administered subcutaneously.
Protective ecacy of vaccines evaluated during 196869 inuenza outbreak, December 9 to February 3. Virus isolated from patients was A2/Hong Kong and did not match vaccine strains. Recommended polyvalent formula that year in USA was: A/PR/8/34, A1/AA/1/57, A2/Japan/ 170/62, A2/Taiwan/1/64, B/Mass/3/66. The vaccine strain was considered to be recommended.
Monto Monto, A.S., DeWolfe Miller, F. and Maassab, H.F. Evaluation of an attenuated, cold recombinant inuenza B virus vaccine. Journal of Infectious Diseases 1982, 145, 5764.
Randomised, single blind, placebo controlled USA trial. Subjects were given a serial number previously assigned randomly by a code to the vaccine or placebo group.
306 volunteer university students. 154 participants in vaccine arm, placebo arm 152. 144 and 140 students respectively completed study.
Monovalent, live attenuated, intranasal inuenza B vaccine against placebo (vaccine diluent). The vaccine virus, cold recombinant, was produced by recombining the attenuated B/Ann Arbor/1/66 with a wild strain B/ Hong Kong/8/73.
Clinical and laboratory conrmed cases and adverse eects. Patients suered a respiratory illness if they had r2 respiratory symptoms. Cases were laboratory conrmed by an increase in antibody titre against 3 inuenza B virus antigens, i.e. if there was a four-fold increase from an initial sample. Adverse eects were dened as sore throat, coryza, hoarseness, cough, muscle aches, temperature >100 F occurred during the rst three days after vaccination. Clinical cases symptoms dened, WDL, and adverse eects. Patients were dened as cases if they had rone upper respiratory illness (a sore throat associated with fever or cough lasting r24 h). Local adverse eects were dened as arm soreness. Systemic adverse eects were dened as fever, tiredness, feeling under the weather, muscle ache, headache.
Protective ecacy of vaccine evaluated during 197980 outbreak; epidemic period dened by rst and last isolation (February 11March 18). Circulating virus strains were B/ Singapore/79like and B/Buenos Aires/79like, antigenically dierent from vaccine. WHO recommended formula that year: A/USSR/90/77 or A/Brazil/11/78, A/ Texas/1/77, B/Hong kong/5/72, and did not match the strains used to produce the recombinant virus.
V. Demicheli et al. / Vaccine 18 (2000) 9571030
Nichol Nichol, K.L., Lind, A., Margolis, K.L. et al. The eectiveness of vaccination against inuenza in healthy, working adults. New England Journal of Medicine 1995, 333, 889893.
USA RCT on full-time employed volunteers. Randomisation performed according to a computer-generated randomisation schedule. Double blinding was ensured by preloaded, coded identical looking syringes.
849 healthy volunteers, 1864 years; 841 had follow up interviews to ascertain side eects. Complete follow up data were obtained for 416 of 422 placebo recipients and 409 of 419 vaccine recipients.
A subvirion, trivalent, parenteral inuenza A and B vaccine was compared against placebo (vaccine diluent). Vaccine strains were A/Texas/36/91, A/Shangdong/9/93, B/Panama/45/90.
Trial was conducted during the 199495 inuenza season. The follow up period was dened as 1 December, 1994 to 31 March, 1995 (the inuenza season). The USA recommended formula for that year was: A/Texas/36/91, A/ Shangdong/9/93, B/ Panama/45/90.
999
Powers 1 Powers, D.C., Smith, G.E., Anderson, E.L. et al. Inuenza A virus vaccine containing puried recombinant H3 hemagglutinin are well tolerated and induce protective immune responses in healthy adults. Journal of Infectious Diseases 1995, 171, 15951599.
USA RCT. 127 subjects randomly assigned to receive one of ve vaccine preparations in a double-blinded manner.
Healthy volunteers in university of St Luis. 1845 year-old.
Data extracted and loaded: Powers 1: recombinant HA0 (N = 77) against placebo (N = 12) The recombinant HA vaccine contained fulllength uncleaved hemagglutinin (HA0) glycoprotein from the inuenza A/Beijing/ 32/92 (H3N2) virus. Three vaccine preparations (15 mg of rHA0, 15 mg of rHA0 plus alume, 90 mg of rHA0). Placebo was saline for injection. All the vaccines were administered intramuscularly.
Clinical and laboratory conrmed cases and adverse eects. `Inuenza like illness': presence of any respiratory symptom(s) for r2 days, with fever or systemic symptoms of myalgias or chills. Laboratory evidence of inuenza A (H3N2) virus infection dened as either or both of the isolation of virus from nasopharyngeal secretion and a rfour-fold increase in serum HAI antibody titre between 3week post-vaccination (preseason) specimen and corresponding postseason specimen collected the following spring. Adverse eects either local: erythema, pain, tenderness, induration, arm stiness; or systemic: headache, generalized myalgia, diarrhoea, nausea, feverishness, temperature >37.88C.
Protective ecacy of the vaccines was evaluated during the 199394 inuenza season. Vaccinations were done during the last November and the rst December. The study ended in the following spring, at least 23 weeks after inuenza viruses were no longer circulating in local communities. The circulating strain was an A (H3N2). The USA recommended formula for that year was: A/Texas/36/91, A/ Beijing/32/92, B/ Panama/45/90. Vaccine matched one of the recommended strains.
1000 V. Demicheli et al. / Vaccine 18 (2000) 9571030
Powers 2 Powers, D.C., Smith, G.E., Anderson, E.L. et al. Inuenza A virus vaccine containing puried recombinant H3 hemagglutinin are well tolerated and induce protective immune responses in healthy adults. Journal of Infectious Diseases 1995, 171, 15951599.
See Powers 1
See Powers 1
Data extracted and loaded: Licensed trivalent (N = 26) against placebo (N = 12) Licensed subvirion trivalent AB vaccine contained 15 mg/dose of each the HAs from inuenza A/Texas/36/91 (H1N1), A/Beijing/ 32/92 (H3N2) and B/ Panama/45/90 viruses Placebo was saline for injection. All the vaccines were administered intramuscularly. Ecacy of a single or double doses a live attenuated, bivalent, intranasal inuenza A (containing 10 exp7,2 EID50) and B (containing 10 exp7,8 EID50 ) vaccine was tested against placebo (5% sucrose). Vaccine virus strains were A/England/42/ 72 (H3N2) and B/ Hong Kong/5/72.
See Powers 1
See Powers I. Vaccine matched the recommended formula.
V. Demicheli et al. / Vaccine 18 (2000) 9571030
Rytel Rytel, M.W., Jakson, L.J., Niebojewski, R.A. et al. Field trial of live attenuated inuenza A/B (`Alice'/R-75) vaccine. American Journal of Epidemiology 1977, 105, 4955.
USA RCT, single blind. Subjects randomly assigned to three subgroups.
Three subgroups received either two doses of the vaccine (N = 47), one dose of vaccine and one dose of placebo (N = 48) or two doses of placebo (N = 48) 14 days apart.
Laboratory conrmed cases (presence of a ulike illness: rthree symptoms of acute respiratory disease and temperature greater then 37.2; and virus isolation and/or four fold rise in antibody titre in sera obtained at 30 days and 6 months following immunisation) and adverse eects (URI symptoms and cough; subdivided into moderate and severe). No general adverse eects denition given (again distinguished among moderate and severe).
Conducted during the 197475 inuenza season in which a two months epidemic period is described by the authors with no reference to a denition. The follow-up period of the study was generically dened as `winter and spring', lasted six months and comprised the epidemic period. The circulating strain was A/ PortChalmers/1/73 (H3N2) and presented a slight antigenic drift when compared with vaccine strain.
1001
Sumarokow Sumarokow, A.A., Popov, V.F., Nefedova, L.A. et al. A study of live inuenza vaccines in a controlled trial. Zhumal Mikrobiologii Epidemiologii Immunobiologii 1971, 48, 4652.
Russian eld trial. Vaccinations were carried out using coded preparation.
76150 persons. A rst study group of 36665 children 312 years old. A second study group counted 39485 subjects aged 1325. Only data regarding the latter were extracted and loaded.
Compared two live vaccines against placebo. Strains used in the vaccines were not reported. Study arms were the following: allantoic intranasal vaccine; N = 9945 placebo; N = 9942 tissue vaccine for oral administration; N = 9817placebo; N = 9781 Only data from the rst two groups were included in the meta-analysis. Trivalent vaccine (A/ Brazil/11/78, A/ Bangkok/1/79, B/ Singapore/222/79 7 mg each) against placebo (sterile saline). Vaccine or placebo was administered by the subcutaneous route.
Clinical and laboratory conrmed cases, deaths, severity. Clinical outcomes were all acute respiratory infections. Laboratory conrmation of illness was obtained by virus isolation or demonstration of seroconversion. Bronchitis, opti and pneumonia were considered as complications.
Outcomes were detected during the entire period of inuenza outbreak. Epidemic period dened as the period of highest inuenza morbidity, lasting 11 weeks from the 22January to the 10 April. Virus circulating was A2/Hong Kong/68, and did not matched the vaccine strains.
1002 V. Demicheli et al. / Vaccine 18 (2000) 9571030
Tannock Tannock, G.A., Bryce, D.A., Hensley, M.J. et al. Responses to one or two doses of a deoxycholate subunit inuenza vaccine in a primed population. Vaccine 1984, 2, 100105.
Australian CCT double blind, placebo controlled,. Volunteers allocated by alternation to receive one or two doses of a trivalent subunit vaccine or placebo.
88 volunteers, aged 1664, sta from a Newcastle Hospital and Commonwealth Steel Corporation. 46 volunteers assigned to each treatment; only individuals receiving expected doses of vaccine considered part of study (29, 27 and 32 for each group). Complete follow up data were obtained for 18, 19, and 20 subjects respectively.
Laboratory conrmed cases (respiratory illness, retrospectively reported, was associated with a 4 fold antibody titre increase between postvaccination and postepidemic sera) and adverse eects. Reactions to vaccination were local reaction: redness, swelling, warmth or irritation; local pain: pain on contact, pain with pressure, continuous pain, or restriction of arm movement; systemic reaction: fever, chills, sweating, drowsiness or insomnia.
Follow up period of 20 weeks and comprised the epidemic period (year 1981) Viral strain isolated from patients was A/Bangkok/1/79. The recommended formula for that year was: A/Brazil/11/78, A/ Bangkok/1/79, B/ Singapore/222/79
Waldman 1 Waldman, R.H. and Coggins, W.J. Inuenza immunization: eld trial on a university campus. Journal of Infectious Diseases 1972, 126, 242248.
USA RCT on a university campus, allocated randomly to study groups and immunised double blinded. Two inactivated vaccines (monovalent A and bivalent AB) by subcutaneous and aerosol administration were compared against placebo (saline).
864 volunteer students and sta members.
Data extracted and loaded: Monovalent A (A2/Aichi/1/68) 200 CCA aerosol against placebo. 195 treated, 98 placebo.
Clinical cases (febrile respiratory illness with oral temperature >99.5 F) and adverse eects. Systemic adverse eects were dened as respiratory (runny and/or stuy nose, sore throat, cough, shortness of breath).
Protective ecacy of vaccines was evaluated during 196869 outbreak. Study follow-up lasted 88 days; likely to cover whole epidemic period. Circulating viral strain was A2/ HongKong virus and matched vaccine strain. Monovalent vaccine recommended in USA was A2/Aichi/2/68. The vaccine strain was considered to be recommended and matching the circulating strain.
V. Demicheli et al. / Vaccine 18 (2000) 9571030
Waldman 2 Waldman, R.H. and Coggins, W.J. Inuenza immunization: eld trial on a university campus. Journal of Infectious Diseases 1972, 126, 242248.
See Waldman 1
See Waldman 1
Data extracted and loaded: Monovalent A (A2/Aichi/1/68) 200 CCA subcutaneous against placebo. 190 treated, 25 placebo.
See Waldman 1
1003
Waldman 3 Waldman, R.H. and Coggins, W.J. Inuenza immunization: eld trial on a university campus. Journal of Infectious Diseases 1972, 126, 242248.
See Waldman 1
See Waldman 1
Data extracted and loaded: Bivalent AB (A2/Japan/170/62 150 CCA, A2/Taiwan/1/ 64 150 CCA and B/ Massachusttes/3/66 200 CCA) aerosol against placebo. 194 treated, 25 placebo.
See Waldman 1
Protective ecacy of vaccines evaluated during 196869 outbreak. Follow-up lasted 88 days and is likely to have covered the whole epidemic period. Circulating viral strain was A2/HongKong virus. Recommended polyvalent formula in USA was: A/PR/8/34, A1/AA/1/57, A2/Japan/ 170/62, A2/Taiwan/1/64, B/Mass/3/66 The vaccine strain was considered to be recommended. See Waldman 3
1004 V. Demicheli et al. / Vaccine 18 (2000) 9571030
Waldman 4 Waldman, R.H. and Coggins, W.J. Inuenza immunization: eld trial on a university campus. Journal of Infectious Diseases 1972, 126, 242248.
See Waldman 1
See Waldman 1
Data extracted and loaded: Bivalent AB (A2/Japan/170/62 150 CCA, A2/Taiwan/1/ 64 150 CCA and B/ Massachusttes/3/66 200 CCA) subcutaneous against placebo. 187 treated and 23 placebo.
See Waldman 1
Waldman 5 Waldman, R.H., Bond, J.O., Levitt, L.P. et al. An evaluation of inuenza Immunization. Bulletin of the World Health Organization 1969, 41, 543548.
Compared two inactivated vaccines (monovalent A and commercial polyvalent AB), administered by dierent schedules (1 or 2 doses) and by intramuscular or aerosol, against placebo (saline). Subjects were randomly divided into 9 groups. Vaccine and placebo were administered double blind on two occasion 3 weeks apart. Study was completed by 99% against placebo (N = 237). See Waldman 5
2100 school teachers; volunteers.
Data extracted and loaded: Waldman 5: monovalent (A/Hong Kong/68) intramuscularly administered (N = 465) against placebo (N = 59).
Clinical cases (temperature >1008F or feverish feeling plus any 2 of the following symptoms: sore throat, muscle or joint pain, cough, stuy or runny nose and side eects). Data concerning adverse eects were only partially reported by graph.
Protective ecacy of vaccines evaluated during the 196869 inuenza season. Follow up lasted 10 weeks and comprised the epidemic period. Outbreak was caused by an A2/Hong Kong/68 inuenza virus. The monovalent vaccine recommended for that year in the USA was A2/Aichi/2/68. Vaccine was considered to be recommended and matching the circulating strain.
V. Demicheli et al. / Vaccine 18 (2000) 9571030
Waldman 6 Waldman, R.H., Bond, J.O., Levitt, L.P. et al. An evaluation of inuenza Immunization. Bulletin of the World Health Organization 1969, 41, 543548.
See Waldman 5
Data extracted and loaded: Waldman 6: polyvalent (A2/ Japan/170/62 150 CCA, A2/Taiwan/1/ 64 150 CCA, B/ Massachusetts/3/66 300 CCA) intramuscularly administered (N = 471) against placebo (N = 59);
See Waldman 5
Protective ecacy of vaccines was evaluated during 196768 inuenza season. Follow up lasted 10 weeks and comprised epidemic period. Outbreak caused by A2/Hong Kong/68 inuenza virus. Polyvalent formula recommended in USA was: A/PR/8/34, A1/AA/1/ 57, A2/Japan/170/62, A2/Taiwan/1/64, B/ Mass/3/66 Viruses used in the vaccines matched the recommended strains.
1005
Waldman 7 Waldman, R.H., Bond, J.O., Levitt, L.P. et al. An evaluation of inuenza Immunization. Bulletin of the World Health Organization 1969, 41, 543548. Waldman 8 Waldman, R.H., Bond, J.O., Levitt, L.P. et al. An evaluation of inuenza Immunization. Bulletin of the World Health Organization 1969, 41, 543548.
See Waldman 5
See Waldman 5
Data extracted and loaded: Waldman 7: monovalent A/Hong Kong/68 aerosol administered (N = 479) against placebo (N = 59);
See Waldman 5
See Waldman 5
1006
See Waldman 5
See Waldman 5
Data extracted and loaded: Waldman 8: polyvalent (A2/ Japan/170/62 150 CCA, A2/Taiwan/1/ 64 150 CCA, B/ Massachusetts/3/66 300 CCA) aerosol administered (N = 471) against placebo (N = 59);
See Waldman 5
See Waldman 7
V. Demicheli et al. / Vaccine 18 (2000) 9571030
Weingarten Weingarten, S., Stanilo, H., Ault, M. et al. Do hospital employees benet from the inuenza vaccine? Journal of General and Internal Medicine 1988, 3, 32 37.
RCT conducted in USA Participants were assigned using a random-number generator. The injections were given and the data were collected in a double blind manner.
179 healthy volunteer hospital employees, 2165 year-old; 91 and 88 subjects respectively.
Split trivalent containing 15 mg each of A/Chile/1/83 (H1N1), A/Philippines/2/82 (H3N2), and B/ USSR/100/83 hemagglutinin antigens) Saline placebo. All injections were given intramuscularly.
Clinical cases symptoms dened, WDL, and adverse eects. Inuenza illness dened by CDC case denition: documented temperature greater than 1008F and at least the symptoms of cough or sore throat. Data regarding adverse eects were not complete and therefore not considered.
Trial was conducted during 1985-86 inuenza season. Epidemic inuenza dened according to population surveillance data (without better explanation), from December 1985 to February 1986. Follow up comprised the epidemic period and lasted 67 days. Most inuenza infections were caused by type B. Authors stated opinion of poor closeness of t between the virus in vaccine and the circulating virus. Recommended formula that year was A/Chile/1/ 83 (H1N1), A/ Philippines/2/82 (H3N2), and B/USSR/ 100/83.
V. Demicheli et al. / Vaccine 18 (2000) 9571030 1007
Williams Williams, M.C., Davignon, L., McDonald, J.C. et al. Trial of aqueous killed inuenza vaccine in Canada, 196869. Bulletin of the World Health Organization 1973, 49, 333340.
Double-blind randomised eld trials in Canadian military bases. Volunteer details were entered in order of attendance on vaccination registers that indicate by code letter the vaccine to be given. Allocation of vaccine code was at random. Vials were coded in so vaccinator did not know which type of vaccine it contained.
Healthy volunteer military recruits.
Data extracted and loaded: a monovalent `standard' IMH aqueous killed inuenza A vaccine (A2/HK/ 68) against a monovalent inuenza B vaccine (B/Mass/66). Participants in the arms were: 1947 (monovalent A), 1955 (monovalent B) All the vaccines were inoculated subcutaneously.
Clinical cases (`respiratory illness' without further specication) and side eects; unsatisfactory denition to be extracted and loaded. Only cases occurred during the epidemic period were evaluated.
In one of the bases an inuenza outbreak occurred during the last week of December 1968 and January 1969. 3 strains, identied as A2/ Hong Kong, were isolated from ill men and were considered matching the monovalent A vaccine. The follow up period lasted 16 weeks. The monovalent vaccine recommended for that year in the USA was A2/Aichi/2/68. The vaccine strain was considered to be recommended and matching the circulating strain.
1008 V. Demicheli et al. / Vaccine 18 (2000) 9571030
Description of studies included in the Amantadine/Rimatadine review Brady Preventive randomised 228 healthy not predouble-blind controlled viously vaccinated Brady, M.T., Sears, trial of rimantadine adult volunteers aged S.D., Pacini, D.L., during an epidemic of 18 to 55. Samorodin, R., inuenza A/Leningrad/ DePamphilis, J., 87 [H3N2] virus. Oakes, M., Soo, W. and Clements, M.L. Safety and prophylactic ecacy of lowdose rimantadine in adults during an inuenza A epidemic. Antimicrobial Agents and Chemotherapy 1990, 34, 16331636.
Randomised to receive either rimantadine 100 mg daily or placebo for six weeks.
Paired sera taken from all participants at beginning and end of the study. Within-trial surveillance carried out weekly basis; cases dened on the basis of seroconversion and a pre-dened list of symptoms and signs. Viral isolation by nasal washout.
Clearly written and wellreported trial (with the exception of the minor discrepancy between text and tables on the aliation of drop-outs). Randomisation was computer generated and allocation was concealed with a centralised scheme. Intention to treat analysis is clearly stated in the text.
Callmander Callmander, E. and Hellgren, L. Amantadine hydrochloride as a prophylactic in respiratory infections. A doubleblind investigation of its clinical use and serology. Journal of Clinical Pharmacology 1968, 8, 186189. Dolin Dolin, R., Reichman, R.C., Madore, H.P., Maynard, R., Linton, P.N. and WebberJones J. A controlled trial of amantadine and rimantadine in the prophylaxis of inuenza A infection. New England Journal of Medicine 1982, 307, 580584.
Randomised controlled trial conducted in a community, including some military personnel. During the trial there was considerable inuenza A2 (Leningrad) activity.
94 volunteers from 20 to 60 years (44 male and 50 female).
Intervention arm received 100 mg of amantadine hydrochloride twice daily; the control arm a no better described placebo.
Expressed in numbers of clinically dened cases (from a symptoms list) in each arm and a symptom score (reported without an indication of time of intensity). Surveillance for adverse eects (systemic) was carried out. List of symptoms (without a denominator) is reported.
Randomisation, allocation and concealment are no further dened, making it impossible to assess methodological rigour although as the distribution of sex and age was checked and found to be similar, randomisation is likely to have been satisfactory.
V. Demicheli et al. / Vaccine 18 (2000) 9571030
Preventive randomised double-blind placebo controlled trial in Burlington Vermont, USA, starting 10 January 1981 during an outbreak of inuenza A/ Bangkok/1/79H3N2 and A/Brazil/11/78H1N1 detected by surveillance (see Fig. 1).
450 healthy non-vaccinated volunteers aged 18 to 45 (mean age 25.6 20.45 years). Final total of participants was 378 (132 in the placebo arm, 133 in the rimantadine arm and 113 in the amantadine arm).
Amantadine 200 mg daily or rimantadine 200 mg or placebo.
Case denition based on a list of symptoms plus virus isolation or a rise in serum antibody titres to inuenza A; both clinically-dened cases and cases dened on the basis of laboratory conrmation.
Although a well-written report, no real information is given on random allocation, blinding and concealment. Intention to treat analysis was not carried out.
1009
Galbraith Galbraith, A.W., Oxford, J.S., Schild, G.C., Potter, C.W. and Watson, G.I. Therapeutic eect of 1adamantanamine hydrochloride in naturally occurring inuenza A 2/Hong Kong infectiona controlled doubleblind study. Lancet 1971, 2, 113115.
Trial carried out December 1969 January 1970, at the time of an epidemic caused by a variant of A2/Hong Kong/68.
Unvaccinated family members aged >2 years recruited by 57 family doctors in the United Kingdom.
153 participants with laboratory-conrmed diagnosis of inuenza A2 randomised to receive either doses appropriate to their ages, for adults amantadine 200 mg a day (N = 72, mean age 37.4 years) or placebo (N = 81, mean age 39.1). Treatment commenced within 48 h of symptoms and continued for seven days. Randomised to receive either amantadine (N = 9, mean 19.1 years) or diluted water placebo (N = 11, mean age 20.3 years) within 48 h of developing symptoms for a duration of four days.
Outcomes are clinical and serological. In our meta-analysis, we included duration of fever in days after commencement of treatment approximating the standard deviation of duration (not reported in the text) from the P value reported in the table. No adverse eect is mentioned or reported in the text.
Although randomisation is clearly mentioned, no detailed description of allocation and concealment is given, making its assessment impossible.
1010 V. Demicheli et al. / Vaccine 18 (2000) 9571030
Hayden 1980 Hayden, F.G., Hall, W.J. and Douglas, R.G. Therapeutic eects of aerosolized amantadine in naturally acquired infection due to inuenza A virus. Journal of Infectious Diseases 1980, 141, 535542.
Randomised doubleblind, placebo controlled treatment trial of inhaled (20 mg daily) amantadine.
20 participants
Inuenza A/Texas/77 [H3N2] and inuenza A/ USSR/77 [H1N1] infections. Cases ascertained clinically and immunologically; outcomes presented as scores at day 2 of follow up for `respiratory illness' and `constitutional illness', not including u-like symptoms. Adverse eects are all local and due to aerosol. We only included nasal burning as the most signicant.
Trial was randomised, but no description of allocation and concealment is given making its assessment impossible. Additionally the rationale for distinguishing between constitutional and respiratory illness is unclear, results of outcomes are not clearly reported (mean scores only are given) and reasons for dropouts are not explained.
Hayden 1981 Hayden, F.G., Gwaltney, J.M., van de Castle, R.L., Adams, K.F. and Giordani, B. Comparative toxicity of amantadine hydrochloride and rimantadine hydrochloride in healthy adults. Antimicrobial Agents and Chemotherapy 1981, 19, 226233.
Toxicity study reporting a randomised control trial in an unspecied period in USA.
State farm insurance company; 251 adult volunteers, aged between 1865 (mean age of 32).
Two trials were carried out simultaneously, both involving Rimantadine and Amantadine. One was a low dose (200 mg daily of each drug, N = 52) trial and the other a higher dose (300 mg daily of each drug, N = 199). The low dose trial however has been excluded due to the absence of any `cases' data, and the lack of outcomes. Randomised to rimantadine 200 mg once daily (mean age 28 years) or placebo (mean age 23 years) for ve days. Treatment started within 48 h of symptom onset.
41 out of 67 (61%) in the Amantadine arm, 13 out of 66 in the placebo arm (20%), and 18 out of 63 in the Rimantadine arm (29%) experienced adverse eects. Adverse eects (systemic only with no other classication) were noted, although not specied.
Randomisation, allocation and concealment practices are no further dened, although all doses were stated as being administered by a project nurse. This is a poorly reported trial as no detailed classication of adverse eects is given, which is a strange practice for a toxicity study. Additionally, data reported in the text does is not consistent with that in Table 1c,
V. Demicheli et al. / Vaccine 18 (2000) 9571030
Hayden 1986 Hayden, F.G. and Monto, A.S. Oral rimantadine hydrochloride therapy of inuenza A virus H3N2 subtype infection in adults. Antimicrobial Agents and Chemotherapy 1986, 29, 339341.
Randomised doubleblind, placebo controlled treatment trial of oral rimantadine in the universities of Virginia and Michigan in 1983.
14 adults with conrmed A/Bangkok/1/ 79(H3N2) inuenza.
Nasal virus shedding, duration of fever (in h) and symptom scores (presented broken down into systemicheadache, chills, malaise etc. and respiratory). Average duration of fever in the rimantadine arm was 31 h (SD=22 h) and 68 (SD=8 h) in the placebo group.
Although the trial is extremely clearly reported, no description of allocation and concealment is given.
1011
Hornick/Wynne Hornick, R.B., Togo, Y., Mahler, S. and Iezzoni, D. Evaluation of amantadine hydrochloride in the treatment of A2 inuenzal disease. Bulletin of the World Health Organization 1969, 41, 671676. Hornick/Richmond Hornick, R.B., Togo, Y., Mahler, S. and Iezzoni, D. Evaluation of amantadine hydrochloride in the treatment of A2 inuenzal disease. Bulletin of the World Health Organization 1969, 41, 671676. Hornick/Walls Hornick, R.B., Togo, Y., Mahler, S. and Iezzoni, D. Evaluation of amantadine hydrochloride in the treatment of A2 inuenzal disease. Bulletin of the World Health Organization 1969, 41, 671676.
Placebo controlled double-blind treatment comparison of amantadine 100 mg with lactose placebo twice daily for 10 days.
153 inmates of four prisons: Richmond, Wynne, Walls and Jessup.
Wynne site (renamed Hornick/Wynne) amantadine N = 17 mean duration 49.8 h, placebo N = 17, mean duration 82.1 h, duration SD=39 h (for both arms).
Inuenza diagnosis was made on the basis of clinical and laboratory ndings. 94 inmates were randomised to receive amantadine and 103 placebo in January 1968, during an epidemic of inuenza A2.
The word `randomised' in not visible in the text, however denominators in each of the arms are highly suggestive of randomisation. No mention of the allocation procedure is made in the text, nor are drop-outs mentioned.
1012
See Hornick 1
See Hornick 1
Richmond site (renamed Hornick/ Richmond) amantadine N = 21 mean duration 60.9 h, placebo N = 28, mean duration 80.1 h, duration SD= 33 h (for both arms).
See Hornick 1
See Hornick 1
V. Demicheli et al. / Vaccine 18 (2000) 9571030
See Hornick 1
See Hornick 1
Walls site (renamed Hornick/Walls) amantadine N = 23 mean duration 65.1 h, placebo N = 20, mean duration 88.3 h, duration SD=28 h (for both arms).
See Hornick 1
See Hornick 1
Hornick/Wynne Hornick, R.B., Togo, Y., Mahler, S. and Iezzoni, D. Evaluation of amantadine hydrochloride in the treatment of A2 inuenzal disease. Bulletin of the World Health Organization 1969, 41, 671676. Kantor Kantor, R.J., Potts, D.W., Stevens, D. and Noble, G.R. Prevention of inuenza A/USSR/77 (H1N1): an evaluation of the side eects and ecacy of amantadine in recruits at Fort Sam Houston. Military Medicine 1980, 145, 312315. Kitamoto 1968 Kitamoto, O. Therapeutic eectiveness of amantadine hydrochloride in inuenza A2double blind studies. Japanese Journal of Tuberculosis and Chest Diseases 1968, 15, 1726.
See Hornick 1
See Hornick 1
Wynne site (renamed Hornick/Wynne) amantadine N = 17 mean duration 49.8 h, placebo N = 17, mean duration 82.1 h, duration SD=39 h (for both arms).
See Hornick 1
See Hornick 1
Preventive double-blind randomised controlled trial of ecacy and safety of oral amantadine compared to a (not further dened) placebo, from 20 February7 March 1978. The target serotype was A/USSR/ 77.
139 healthy paramedic recruits (mean age 22 years) in the military barracks at Fort Sam Houston (FSH), Texas.
Randomised to receive either amantadine 100 mg tablets twice daily (N = 64) or placebo (N = 62).
Case denition by a list of recognised symptoms and serological conrmation and adverse eects were recorded in the questionnaires. Paired sera were obtained at the beginning of the study and ve weeks later. Cases were also presented by severity.
Although the trial was randomised and allocation concealment was protected through a system of sealed envelopes, the diculty in reconciling gures and understanding what actually happened during the trial makes this a very poorly reported study. No reason for the loss of 20 participants to follow up is given.
V. Demicheli et al. / Vaccine 18 (2000) 9571030
Randomised doubleblind, placebo controlled treatment trial of oral amantadine, during the 196768 inuenza season throughout Japan.
Not specied
355 participants randomised to amantadine (N = 182) (200 mg/day for adults) or placebo (N = 173) within 48 h of developing symptoms.
Case denition based on symptoms and serological conrmation. During the trial A2/Kumamoto/ 1/65 virus and its drifted variants were circulating in the community.
Although the trial is adequately reported and clearly randomised, no description of allocation and concealment is given making its assessment impossible.
1013
Kitamoto 1971 Kitamoto, O. Therapeutic eectiveness of amantadine hydrochloride in naturally occurring Hong Kong inuenzadouble-blind studies. Japanese Journal of Tuberculosis & Chest Diseases 1971, 17, 1 7. Knight Knight, V., Fedson, D., Baldini, J., Douglas, R.G. and Couch, R.B. Amantadine therapy of epidemic inuenza A2 (Hong Kong). Infection and Immunity 1970, 1, 200204.
Randomised doubleblind, placebo controlled treatment trial of oral amantadine, during the 196869 inuenza season throughout Japan.
Seventy nine participants were randomised to amantadine (200 mg/day for adults) and 76 placebo for seven days within 48 h of developing symptoms.
Amantadine and placebo in a treatment role.
Case denition based on symptoms and serological conrmation of infection. Outcomes were duration of fever (in days), dened as a temperature of more that 378C and there were no dropouts from the study.
Although randomisation was clearly applied and no dropouts are reported, no description of allocation and concealment is given making its assessment impossible. In addition the fate to follow up of 353 participants is unclear.
1014 V. Demicheli et al. / Vaccine 18 (2000) 9571030
Randomised double blind comparison treatment trial in two units of the Texas Department of Corrections during a A2/Hong Kong inuenza outbreak in January 1969.
29 unvaccinated male inmates 2242 years. Only men with serological and culture (nasal virus shedding) illness conrmation took part, i.e. 29 of 37. Illness manifested an average of 42 h before in amantadinetreated men and 36 h for placebo; authors state dierences not signicant.
Amantadine compared to placebo. Randomised to amantadine 100 mg (N = 13) or placebo capsules (N = 16) twice daily for at least 6 days.
Clinical (duration of fever and symptom score) or serological and laboratory-based (antibody titre and viral shedding).
Although randomisation was clearly applied and no dropouts are reported, no description of allocation and concealment is given making its assessment impossible.
Monto Monto, A.S., Gunn, R.A., Bandyk, M.G. and King, C.L. Prevention of Russian inuenza by amantadine. Journal of the American Medical Association 1979, 241, 10031007.
Preventive randomised double-blind placebo controlled trial from February 1978, during outbreak of inuenza A/ USSR-like (H1N1) for seven weeks (end of outbreak conrmed by clinical and serological surveillance).
Healthy student volunteers at University of Michigan, USA.
286 students aged 18 to 24 randomly assigned to amantadine 100 mg twice daily or placebo. Follow up weekly for seven weeks, the remaining duration of the outbreak of inuenza.
Respiratory and adverse eect symptoms were recorded in weekly calendar-diaries and paired sera samples were taken at the beginning and end of the trial (including 5 dropouts from the trial because of clinical inuenza or major adverse eects) from 281 of the participants. Numbers of clinically dened cases from a symptom score coupled with virus-specic antibody rise, allowing the authors to distinguish non-inuenza related illness during periods 1 and 2 (reported without an indication of intensity of symptoms). During period 1 six students had inuenza (5 with serological conrmation) out of the 53 in the intervention arm and 10 (2 with serological conrmation) out of the 52 in the placebo arm.
The trial is well written and appears well conducted with only minor discrepancies in total numbers. The practice of random allocation and concealment appear adequate. Analysis was not carried on an intention to treat basis.
Muldoon Muldoon, R.L., Stanley, E.D. and Jackson, G.G. Use and withdrawal of amantadine chemoprophylaxis during epidemic inuenza A. American Review of Respiratory Disease 1976, 113, 487491.
Crossover preventive controlled trial conducted in a school near Chicago (USA) between 2 December and 20 December 1968 (period 1).
105 unvaccinated volunteer students aged around 21.
At beginning and end of period 1 (18 days) blood samples were taken; 53 individuals in intervention arm received 100 mg of amantadine hydrochloride twice daily, and control arm an 'oral placebo'. After a `holiday' period of 16 days (period 2) participants were crossed over to assess whether withdrawal of amantadine rendered participants more or less susceptible to infection. The procedure was inverted and students were followed up for a further 10 days (period 3).
The practices of randomisation, allocation and concealment are not dened, making it impossible to assess methodological rigour, although the similar numbers of participants in each arm led us to consider this a randomised trial. No drop outs are reported.
V. Demicheli et al. / Vaccine 18 (2000) 9571030 1015
Oker-Blom Oker-Blom, N., Hovi, T., Leinikki, P., Palosuo, T., Pettersson, R. and Suni, J. Protection of man from natural infection with inuenza A2 Hong Kong virus by amantadine: a controlled eld trial. British Medical Journal 1970, 3, 676 678. Payler Payler, D.K. and Purdham, P.A. Inuenza A prophylaxis with amantadine in a boarding school. Lancet 1984, 1, 502 504.
Preventive randomised double-blind placebo controlled trial from 20 January 1969 in Helsinki, Finland for 30 days.
391 healthy medical students (132 females and 259 males) aged on average 22 years. Inuenza A2 Hong Kong was the main circulating strain at the time.
Randomised to amantadine 100 mg or placebo (tablets containing calcium lactate) twice daily. Additionally the authors analysed agestratied results for each arm (although the results are not included in the text).
Self-reported (by questionnaire) clinical symptoms and serological titres. Adverse eects were recorded too.
Randomisation and allocation are not suciently described whereas the placebo tablets are described as `identical'. No reason is given for the two dropouts from the study.
1016 V. Demicheli et al. / Vaccine 18 (2000) 9571030
Preventive randomised open trial of 536 members of Malvern Boys School in the UK.
Boys, 13 to 19 had been previously immunised in the autumn of 1982 (viral strain not reported).
Randomised to amantadine 100 mg daily (N = 267 or no treatment N = 269) for 14 days from 18 February 1983, as soon as the cases of laboratory-conrmed inuenza were described.
Case denition is unclear but from the results it would appear that clinical denitions and laboratory isolates were used. A/H1N1 was the prevalent viral strain.
Although the trial was randomised, the design is open and the analysis was not carried out on intention to treat. Additionally, length of follow up is not reported.
Peckinpaugh 1 Peckinpaugh, R.O., Askin, F.B., Pierce, W.E., Edwards, E.A., Johnson, D.P. and Jackson, G.G. Field studies with amantadine: acceptability and protection.
A randomised factorial double-blind controlled trial conducted from 5 December 1967 to 1 June 1968.
US Naval trainees; 2079 oral amantadine and 2104 placebo.
Comparison of oral amantadine (200 mg daily) on 2079 individuals and oral placebo on 2104 individuals, with and without vaccine. Administration continued for 28 days. Individuals in each arm, three days after commencing treatment were assigned to receive either vaccine (2059 individuals) or subcutaneous saline placebo (2124 individuals). Randomised to receive either amantadine 200 mg daily (N = 1329) or placebo (N = 1321) orally for 20 days.
Presented by intervention arm: amantadine and vaccine1039 individuals, vaccine and oral placebo1020 individuals, amantadine and subcutaneous placebo 1040 and subcutaneous and oral placebo1084 individuals. Outcomes are % of participants not seeking treatment, sought treatment as outpatients, or admitted to local hospital.
The study was denitely randomised and arrangements to conceal allocation appear adequate. The standard of reporting is poor with outcomes reported in histogram form, making estimation of their incidence necessary.
V. Demicheli et al. / Vaccine 18 (2000) 9571030
Peckinpaugh 2 Peckinpaugh, R.O., Askin, F.B., Pierce, W.E., Edwards, E.A., Johnson, D.P. and Jackson, G.G. Field studies with amantadine: acceptability and protection.
Study conducted from December 1968 to May 1969.
US Naval recruits
As in Peckinpaugh 1, serological assessment was carried out on one fourth of participants (416 sera pairs). Outcome denition and presentation were similar to those in Peckinpaugh 1, as is our transformation of them.
The study was randomised and arrangements to conceal allocation appear adequate. Reporting standard is poor with outcomes reported in histogram form, making estimation of their incidence necessary. Contradictory statements in the text concerning denition of cases and serological outcomes make interpretation dicult.
1017
Pettersson Pettersson, R.F., Hellstrom, P.E., Penttinen, K., Pyhala, R., Tokola, O., Vartio, T. and Visakorpi, R. Evaluation of amantadine in the prophylaxis of inuenza A (H1N1) virus infection: a controlled eld trial among young adults and high-risk patients. Journal of Infectious Diseases 1980, 142, 377383. Plesnik Plesnik, V., Heinz, F., Bindas, B. et al. Controlled study of inuenza prophylaxis using amantadine VUFB. Cs Epidemiologie mikrobiologie, immunologie 1977, 4. (translated from Czeck).
Preventive randomised placebo- controlled double-blind trial in a military training centre in Finland commencing on 17 January 1978. At the time an epidemic of A H1N1 was underway in the surrounding community.
192 participants (military recruits aged 21 average).
Randomly assigned to receive either amantadine 200 mg daily of calcium lactate placebo tablets.
Follow up for three weeks and cases were dened on the basis of retrospective analysis of questionnaires and antibody titre rise in paired sera. Infection with inuenza A H3N2 virus also was veried serologically.
Although the study report is well written and random allocation was carried out on the basis of random number tables, allocation concealment was unspecied and intention to treat analysis did not take place.
1018 V. Demicheli et al. / Vaccine 18 (2000) 9571030
Preventive randomised double-blind controlled trial of amantadine during an epidemic of inuenza A/Victoria/42/ 75 [H3N2] virus from mid March 1976 in the former Czechoslovakia and lasted 20 days.
1133 healthy students, industrial workers and elderly aged 10 to 69.
Randomised to receive either amantadine 100 mg once or twice daily (N = 574) or placebo (N = 559), one or two tablets daily.
Case denition was based on inuenza symptoms and antibody titre rise from paired sera and viral isolation (although from the translated text it is not clear whether this practice covered the whole study population). Adverse eects are reported in detail in the trial.
Although randomisation, allocation and analysis on an intention to treat are not described, concealment is described as a centralised scheme with coded tablets and is therefore assessed as adequate.
Quarles Quarles, J.M., Couch, R.B., Cate, T.R. and Goswick, C.B. Comparison of amantadine and rimantadine for prevention of type A (Russian) inuenza. Antiviral Research 1981, 1, 149155.
Preventive randomised double blind placebocontrolled trial at the University of Texas. Trial commenced on week 7 (? mid February) 1978 during an epidemic of inuenza A/USSR/ 90/77 virus.
444 healthy students aged 18 to 24 followed up for six weeks on the basis weekly of self-reporting.
Randomised to amantadine (100 mg), or rimantadine (100 mg), or placebo (not specied) tablets twice daily.
Cases were dened on the basis of paired sera and clinical symptoms. Viral isolation from throat swabs was additionally carried out.
The practices of randomisation, allocation and concealment are not dened, making it impossible to assess methodological rigour. Analysis on the basis of intention to treat was not carried out and the overall quality of reporting is poor (with no complete details of reasons for dropout). The study is of good quality with computergenerated randomisation, checks on allocation concealment and good blinding procedures. No dropouts are reported.
V. Demicheli et al. / Vaccine 18 (2000) 9571030
Reuman Reuman, P.D., Bernstein, D.I., Keefer, M.C., Young, E.C., Sherwood, J.R. and Schi, G.M. Ecacy and safety of low dosage amantadine hydrochloride as prophylaxis for inuenza A. Antiviral Research, 1989, 11, 2740.
Double-blind preventive randomised controlled trial. Follow up weekly for six weeks through symptom diaries and visits; those reporting with inuenza- like illness had examination and nasal washouts on two consecutive days. Adverse eects were recorded. Random blood tests on 48 subjects gave results consistent with compliance. Paired sera from beginning and end of trial were tested for antibodies against A/Chile/ 1/83(H1N1), A/ Philippines/1/82(H3N2) and B/USSR/100/83, the prevalent viruses during the study period. Viral assays were performed from nasal washouts.
476 healthy hospital personnel aged 18 to 55 at Cincinnati Christ Hospital, Ohio, USA during the 198586 inuenza season.
Three arms to the trial: (a) 159 subjects randomly allocated to receive amantadine 100 mg/day (b) 159 subjects randomly allocated to receive amantadine 200 mg/ day (c) 158 subjects randomly allocated to receive identical looking placebo capsules each day.
Five participants were infected in the placebo group, two subjects in the 100 mg group and one in the 200 mg group. The number of participants with at least one (systemic) adverse eect was 49 in the placebo arm, 47 in the 100 mg arm and 71 in the 200 mg arm, indicating a clear dose-adverse eect relationship. Inuenza-like illness predened from a list of signs and symptoms.
1019
Schapira Schapira, M., Oxford, J.S. and Galbraith, A.W. A study of 1 adamantamine hydrochloride during the 1970 Hong Kong inuenza epidemic. Journal of the Royal College of General Practitioners 1971, 21, 695697.
Placebo-controlled trial of amantadine conducted in the Northern English village of Keighly by a general practitioner during the winter of 196869.
297 healthy volunteers from rms, schools, a newspaper, a bank and families. Mean age was evenly matched at 38 years (active arm) and 38.5 years (placebo arm).
Amantadine 100 mg every 12 h (157 participants) or oil-based placebo capsule (140 participants), identied by a code. Follow up was 10 days. Sera were screened prior to commencement; those mentioning symptoms of inuenza underwent a second antibody titre estimation against A2/Hong Kong/1/68, the prevalent strain. Some participants may have been infected prior to commencement; authors point out that trial is preventive and curative.
49 of 157 volunteers in treatment arm suered inuenza symptoms compared to 39 out 140 in placebo arm. However only 8 and 15 cases respectively were serologically conrmed as inuenza. Twelve paired sera were unavailable for the 49 symptomatic volunteers in the treatment arm; three paired sera were unavailable although the authors do not explain the reason for the drop outs. Adverse eects are not reported.
The authors conclude that the trial provides `marginal' evidence of preventive eect of amantadine. The practices of randomisation, and allocation are not described, making it impossible to assess methodological rigour, although the similar numbers of participants in each arm led us to consider this a randomised trial. Allocation concealment appeared adequate.
1020 V. Demicheli et al. / Vaccine 18 (2000) 9571030
Smorodintsev Smorodintsev, A.A., Karpuhin, G.I., Zlydnikov, D.M., Malyseva, A.M., Svecova, E.G., Burov, S.A., Hramcova, L.M., Romanov, J.A., Taros, L.J., Ivannikov, J.G. and Novoselov, S.D. The prophylactic eectiveness of amantadine hydrochloride in an epidemic of Hong Kong inuenza in Leningrad in 1969. Bulletin of the World Health Organization 1970, 42, 865872. van Voris van Voris, L.P., Betts, R.F., Hayden, F.G., Christmas, W.A. and Douglas, R.G. Successful treatment of naturally occurring inuenza A/USSR/77 H1N1. Journal of the American Medical Association 1981, 245, 11281131.
Preventive randomised double-blind placebo controlled trial carried out in eight engineering schools around Leningrad, in the former USSR. The design comprised an `internal' (day students) and `external' (i.e. boarders) do-nothing control groups which will not be further taken into consideration as they took no medication.
Males, aged 1830.
Randomised to receive amantadine 100 mg daily (N = 5092) or placebo tablets (N = 3175). Commenced around January 1969 with staggered starts, according to the results of school specic surveillance against A2/Hong Kong/68 virus. Dierential follow-up is also recorded between placebo and amantadine arms (30 days) and controls (12 days).
Case denition was based on a list of symptoms plus a four-fold rise in serum antibody titres to inuenza A.
Although randomisation occurred and concealment is described in an adequate manner, an unknown number of participants were given amantadine syrup. As no reference to syrup placebo is made in the text (only to tablet form), robustness of blinding and concealment is questionable. Additionally the numerous discrepancies in the text make this a poorly reported trial.
V. Demicheli et al. / Vaccine 18 (2000) 9571030
Randomised in a double-blind design treatment trial.
45 students with laboratory conrmed inuenza A/USSR/77 [H1N1] in February 1978 in University of Rochester, USA .
Amantadine 200 mg daily (N = 14) or rimantadine 200 mg daily (N = 14) or inert placebo capsules (N = 12) and followed up for ve days.
Symptom scores, duration of temperature. We used the outcome `number of participants with temperatures >37.58C", 48 h after commencing medication (a dichotomous outcome). Data on mean duration of fever were not given.
The trial is well reported and denitely randomised. Allocation concealment is described and appears to be adequate.
1021
Wendel Wendel, H.A., Snyder, M.T. and Pell, S. Trial of amantadine in epidemic inuenza. Clinical Pharmacology and Therapeutics 1966, 7, 3843. Wingeld Wingeld, W.L., Pollack, D. and Grunert, R.R. Therapeutic ecacy of amantadine HC1 and rimantadine HC1 in naturally occurring inuenza A2 respiratory illness in man. New England Journal of Medicine 1969, 281, 579584.
Preventive and treatment randomised double blind placebo-controlled trial in a prison community in Philadelphia, USA in January 1963.
Prison inmates aged 1754 exposed to naturally occurring inuenza A2Japan305/57 virus.
Placebo was a lactose tablet. In the preventive trial 794 inmates were randomised to receive amantadine 200 mg daily (N = 439) or placebo (N = 355). Follow-up length was 10 days.
Cases were dened both clinically and serologically.
The trials are well reported although randomisation was not good (as conrmed by uneven numbers in the arms20% excess in the amantadine arm) and allocation concealment is adequate
1022
Randomised double blind placebo-controlled treatment trial in the Virginia State Penitentiary, USA, during an outbreak of inuenza A2/Rockville/ 1/65 in JanuaryFebruary 1968.
95 inmates whose symptoms developed in the previous 24 h.
Randomised to amantadine 100 mg (N = 23), or rimantadine 150 mg (N = 24) or placebo lactose capsules (N = 48) twice daily. Medication commenced within 24 h of developing symptoms and continued for 10 days. The nal denominators for which data are provided in the report: Placebo N = 39 Amantadine N = 20 Rimantadine=20.
Only data relating to participants with temperatures of r37.58C on the rst day of the study were analysed of the duration of fever outcome and one participant was later found not to have a rise at the second antibody titre estimation. We have included duration of fever as the clinical outcome in our meta-analysis.
Randomisation and allocation concealment are detailed in the text with individual coded `vials' (which we assume to mean containers) system. Intention to treat analysis appears to have taken place on individuals who fullled clinical and serological criteria.
V. Demicheli et al. / Vaccine 18 (2000) 9571030
Younkin Younkin, S.W., Betts, R.F., Roth, F.K. and Douglas, R.G. Reduction in fever and symptoms in young adults with inuenza A/Brazil/78 H1N1 infection after treatment with aspirin or amantadine. Antimicrobial Agents and Chemotherapy 1983, 23, 577582.
Randomised double blind comparison of amantadine with aspirin, during an outbreak of inuenza A/Brazil/78 [H1N1] in the winter of 1981.
48 otherwise healthy college students aged 17 to 20 from the University of Rochester, New York, USA. Participants all had clinical and (later) laboratory conrmed diagnosis of inuenza.
Randomised to amantadine 100 mg a day (N = 16), 200 mg a day (N = 14) or aspirin 3.25 grams a day (N = 17).
Outcomes are presented as both symptoms scores and duration of fever (in the text).
Randomisation and allocation concealment are well detailed in the text and concealment in particular appears very robust with an elaborate system of envelopes. To uniformly make up the tablets number, the aspirin arm had two placebo tablets included. Compliance was equally tested by daily questioning.
V. Demicheli et al. / Vaccine 18 (2000) 9571030
Description of studies included in the neuraminidase inhibitor review Calfee 1 Calfee, D.P., Peng, A.W., Cass, L.M.R., Lob, M. and Hayden, F.G. Protective ecacy of intravenous Zanamivir in experimental human inuenza. Abstract H58 at the 38th Interscience Conference of Antimicrobial Agents and Chemotherapy on 2427 September 1998. Randomised placebo controlled preventive trial of IV Zanamivir in experimental inuenza. 16 healthy adults male volunteers. Saline placebo or Zanamivir 600 mg twice daily for 5 days beginning four h before inoculation with A/Texas/91 [H1N1]. A mixture of serological, clinical and laboratoryconrmed. The authors conclude that this study is the rst to show the IV Zanamivir is protective against inuenza (for example being 100% eective in preventing viral nasal shedding). The methodological quality of the study is dicult to assess as no description is given. Randomisation is explicitly mentioned in the text of the abstract.
1023
Calfee 2 Calfee, D.P., Peng, A.W., Hussey, E.K., Lobo, M. and Hayden, F.G. Protective ecacy of reduced frequency dosing of intranasal Zanamivir in experimental human inuenza. Abstract H68 at the 38th Interscience Conference of Antimicrobial Agents and Chemotherapy on 2427 September 1998. Hayden 1996a Hayden, F.G., Lobo, M., Hussey, E.K. and Eason, C.U. Ecacy of intranasal GG167 in experimental human inuenza A and B virus infection. In: Options for the control of inuenza III (Eds Brown, L.E., Hampson, A.W. and Webster, R.G.). Elsevier Science, Amsterdam, 1996, pp. 718724.
Preventive placebo controlled double-blind randomised trial of Zanamivir nasal spray in 43 individuals experimentally exposed to A/ Texas/91 [H1N1] virus.
Arms 3 and 4 of the trial were carried out on 19 subjects (10 in the active arm and 9 in the placebo arm).
Administration of a single dose of Zanamivir began either 48 h, or 4 h (N = 12). These subjects were given intranasal Zanamivir daily for 3 days from the day of experimental exposure).
A mixture of laboratory and clinical but in our review we include data on laboratory conrmed individuals with symptoms. The authors conclude that their trial provides the rst evidence on humans that a single daily dose of Zanamivir is ecacious in the prevention of inuenza.
The methodological quality of the studies is dicult to assess as no detailed description is given in the abstract. Randomisation is explicitly mentioned and was conrmed to the reviewers by the manufacturers.
1024 V. Demicheli et al. / Vaccine 18 (2000) 9571030
Preventive placebo controlled double-blind randomised trial of Zanamivir.
Nasal spray in 34 individuals experimentally exposed to B/ Yamagata/88 virus.
Administration of GG167 began four h prior to inoculation with the virus and continued for ve days. Susceptible individuals were assigned to receive either GG167 3.2 mg twice daily (N = 9), or 6.4 mg twice daily (N = 8), or 6.4 mg once daily (N = 8) or aqueous placebo spray (N = 9).
Infection (viral nasal shedding and HI antibody rise) or upper respiratory illness dened as the presence of rtwo respiratory symptoms on r2 days.
The authors remark that the proportion of subjects developing illness was signicantly lower in the two twice-daily arms. The methodological quality of the study is dicult to assess as no detailed description of methods is given, although a note under Table 1 describes the necessity to randomise each placebo group in a 3:1 ratio to preserve double-blinding. Randomisation is explicitly mentioned.
Hayden 1996b Hayden, F.G., Treanor, J.J., Betts, R.F., Lobo, M., Esinhart, J.D. and Hussey, E.K. Safety and ecacy of the neuraminidase inhibitor GG167 in experimental human inuenza. Journal of the American Medical Association 1996, 275, 295299.
As Hayden 1996a
As Hayden 1996a
As Hayden 1996a
Outcomes were infection (viral nasal shedding and HI antibody rise) or upper respiratory illness dened as the presence of rtwo respiratory symptoms on r2 days.
As Hayden 1996a
V. Demicheli et al. / Vaccine 18 (2000) 9571030 1025
Hayden 1997 Hayden, F.G., Osterhaus, A.D., Treanor, J.J., Fleming, D.M., Aoki, F.Y., Nicholson, K.G., Bohnen, A.M., Hirst, H.M., Keene, O. and Wightman, K. Ecacy and safety of the neuraminidase inhibitor Zanamivir in the treatment of inuenza virus infections. New England Journal of Medicine 1997, 337, 874880.
Two multicentre trials in North America (38 centres, 220 individuals) and Europe (32 centres, 197 individuals) conducted during the 1994 95 inuenza season to assess the treatment eects of Zanamivir using a randomised, double-blind, placebo controlled design.
Otherwise healthy individuals with symptoms suggestive of inuenza persisting longer than 48 h. Mean ages of subjects in the three arms were 3133 years.
Randomised to 10 mg of inhaled Zanamivir by mouth plus 6.4 mg by intranasal spray or 10 mg of inhaled Zanamivir and intranasal placebo spray or aqueous placebo by both routes twice daily for ve days. During convalescence HAI titres were assessed and 262 individuals had laboratory conrmed inuenza. Of these, 56% were due to A/ H3N2 and 44B virus.
Nine placebo patients and 10 from each of the other arms withdrew or were lost to follow-up (explained in the text as failure to at tend for the follow-up visits). The major outcome assessed in the trial was `time to alleviation of major symptoms' (dened as absence of fever and headache, muscle ache, sore throat and cough). Additionally, time to resumption of usual activities are also reported.
Individuals commencing treatment 30 h from illness onset fared signicantly better than those commencing later. Both interventions signicantly shortened duration of illness compared to placebo (5.3 and 5.4 days compared to 6.3 days). Inhaled and intranasal Zanamivir signicantly shortened non-eective time compared to placebo. No eect seen on non-inuenza infected patients (although data not presented in text). Adverse eects are generalised (respiratory tract and gastrointestinal) or local (perinasal). Authors conclude that Zanamivir is safe and eective treatment against inuenza A and B if given early in illness. Although clearly randomised, no details of allocation or double blinding are given. Intention to treat analysis has clearly taken place
1026 V. Demicheli et al. / Vaccine 18 (2000) 9571030
Monto Monto, A.S., Robinson, D.P., Herlocher, L., Hinson, J.M., Elliott, M. and Keene, O. Ecacy and safety of Zanamivir in prevention of inuenza among healthy adults. Abstract LB7 at 38th Interscience Conference of Antimicrobial Agents and Chemotherapy on 2427 September 1998. WV 15673 & WV 15697 Ro640796 (GS 4104): results and safety update from studies conducted in the Northern Hemisphere 19978. 1. Prophylaxis studies WV 15673 and WV 15697. Homan LaRoche 1998 (unpublished manuscript).
Preventive placebo controlled double-blind randomised trial of Zanamivir nasal spray in healthy individuals naturally exposed to mainly A [H3N2] virus.
1107 healthy individuals naturally exposed to mainly A [H3N2] virus.
Randomised to Zanamivir (N = 553) or placebo (N = 554), 10 mg inhaled for 4 weeks.
A mixture of laboratory and clinical but we have included data only on laboratory conrmed symptomatic cases in our review. Adverse eects were no dierent in the two arms. Withdrawals due to adverse eects in the two arms were less than 1%. The authors conclude that their trial provides evidence that Zanamivir is ecacious in the prevention of inuenza.
The methodological quality of the study is dicult to assess as no detailed description is given in the abstract. Randomisation is explicitly mentioned.
V. Demicheli et al. / Vaccine 18 (2000) 9571030
WV 15673 and WV 15697 are short reports of randomised double blind placebo controlled preventive phase IIIa trials of Oseltamivir conducted in the Northern Hemisphere during the 199798 winter.
1559 healthy unvaccinated adults aged 18 65.
Participants were randomised to receive either Oseltamivir 75 mg daily orally (N = 520), or twice daily (N = 520) or placebo (N = 519). Medication continued for 6 weeks after recognition of the outbreak in the study area (not better identied).
Cases of clinically dened inuenza and adverse events.
Authors conclude that protection of 76% is satisfactory given low level of inuenza activity. Preliminary safety data indicate good tolerability. Methodological quality of studies is dicult to assess as no description is given. Randomisation is not explicitly mentioned but was conrmed to reviewers by the principal investigator.
1027
WV 15670 Ro640796 (GS 4104): results and safety update from studies conducted in the Northern Hemisphere 19978. 2. Treatment studies WV 15670 and WV 15671. Homan LaRoche 1998 (unpublished manuscript).
WV 15670 is a short report of randomised double blind placebo controlled preventive phase IIIa trials of Oseltamivir. WV 15670 was conducted in Europe, Canada and China during the 1997 98 winter.
473 otherwise healthy individuals who presented with at least on respiratory and one constitutional symptom were randomised within 36 h of onset.
Oseltamivir 75 mg daily orally (N = 155), or twice daily (N = 157), or placebo (N = 161) for ve days.
Time to alleviation of symptoms expressed in days and type and incidence of adverse events. Additionally severity of illness was also assessed by means of a symptom score.
Time to alleviation of symptoms was signicantly reduced in active arms, and 30% reduction in symptoms scores of active arms of both trials. As in prophylaxis/ prevention trials, nausea was most reported systemic adverse event, especially at higher dose (see WV 15671). Methodological quality of study dicult to assess as no description is given, in keeping with preliminary report nature. Randomisation is explicitly mentioned in text.
1028 V. Demicheli et al. / Vaccine 18 (2000) 9571030
WV 15671 Ro640796 (GS 4104): results and safety update from studies conducted in the Northern Hemisphere 19978. 2. Treatment studies WV 15670 and WV 15671. Homan LaRoche 1998 (unpublished manuscript).
WV 15671 is a short report of a randomised double blind placebo controlled preventive phase IIIa trials of Oseltamivir. WV 15671 was conducted in the USA during the 1997 98 winter.
368 otherwise healthy individuals who presented with at least on respiratory and one constitutional symptom were randomised within 36 h of onset.
Participants received either Oseltamivir 75 mg twice daily orally (N = 128), or 150 mg twice daily (N = 122), or placebo (N = 128) for ve days.
As in WV 15670.
Time to alleviation of symptoms was signicantly reduced in active arms, and 30% reduction in symptoms scores of active arms of both trials. As in prophylaxis/ prevention trials of Oseltamivir, nausea was most reported systemic adverse event, especially at the higher dose. In view of this and lack of signicant dierence between doses, trialists recommend that future trials adopt lower (75 mg twice daily) dose. Methodological quality of study is dicult to assess as no description is given, in keeping with nature of report. Randomisation is explicitly mentioned in the text.
V. Demicheli et al. / Vaccine 18 (2000) 9571030 1029
1030
V. Demicheli et al. / Vaccine 18 (2000) 9571030 [22] Penn CR. Inhibitors of inuenza virus neuraminidase. In: Nicholson KG, Hay RG, Webster AJ, editors. Textbook of Inuenza. London: Blackwell, 1998. p. 47787 (Chapter 36). [23] Couch RB. A new antiviral agent for inuenza: Is there a clinical niche? New England Journal of Medicine 1997;337:9278 (editorial). [24] Pfeier N. Firms racing to develop drugs for inuenza virus. Genetic Engineering News 1997;17(1 November):116. [25] Wright LA, Demicheli V, Gillespie W, Jeerson TO. Morbidity surveillance in the British Army the rst 12 months. J R Army Med Corps 1998;144:117. [26] McMenamin J, Morton R, McEwen J. Report of a pilot programme of enhanced surveillance of respiratory illness in the British Army (UK). University of Glasgow, Department of Public Health, 1998. [27] Demicheli V, Rivetti D, Deeks JJ, Jeerson TO. Inuenza vaccines in healthy adults. Cochrane Database of Systematic Reviews (Acute Respiratory Infections Module). Update Software 1999 (forthcoming). [28] Jeerson TO, Demicheli V, Deeks JJ, Rivetti D. Amantadine & rimantadine for inuenza. Cochrane Database of Systematic Reviews (Acute Respiratory Infections Module). Update Software 1999, issue 2. [29] Jeerson TO, Demicheli V, Deeks JJ, Rivetti D. Neuraminidase inhibitors for inuenza. Cochrane Database of Systematic Reviews (Acute Respiratory Infections Module). Update Software 1999, issue 2. [30] Drummond MF, Jeerson TO (for the BMJ Working Party on guidelines for authors peer-reviewers of economic submissions to the British Medical Journal) Buxton M Demicheli V, Donaldson C, Jonsson B, Mugford M, Rennie D, Rovira J, Rutten F, Schulman K, Smith R, Tonks A, Torrance G, Towse A. Guidelines for authors and peer-reviewers of economic submissions to the British Medical Journal. BMJ 1996;313(3 August):27583. [31] Cochrane Acute Respiratory Infections Group. Search strategy for specialised register. Cochrane Library 1998 Issue 1. Oxford: Update Software (updated quarterly). [32] Jeerson TO, Jeerson VM. The quest for trials on the ecacy of human vaccines. Results of the handsearch of `Vaccine'. Vaccine 1996;14:4614. [33] Jeerson TO. Vaccine trial data systematically assembled, pooled and disseminated by the Cochrane Collaboration. Vaccine 1998;16:148795. [34] Schulz KF, Chalmers I, Hayes RJ, Altman DG. Empirical evidence of bias. Dimensions of methodological quality associated with estimates of treatment eects in controlled trials. JAMA 1995;273:40812. [35] Jeerson TO Demicheli V. Economic evaluation of Inuenza vaccination and economic modelling. Can results be pooled? Pharmacoeconomics 1996;9(Suppl 3):6772. [36] Jeerson TO, Demicheli V. A systematic review of world literature on the economics of inuenza. Information and News on Inuenza. European Scientic Working Group on Inuenza (Newsletter) 1997;7:6. [37] Aoki FY. Amantadine and rimantadine. In: Nicholson KG, Hay AJ, Webster RG, editors. Textbook of Inuenza. London: Blackwell, 1998. p. 45776.
References
[1] Wiselka M. Inuenza: diagnosis, management and prophylaxis. BMJ 1994;308:13415. [2] Bonn D. Spared an inuenza pandemic for another year? Lancet 1997;349:36. [3] Belshe RB. Inuenza as a zoonosis: how likely is a pandemic? Lancet 1998;351:4601. [4] Yuen KY, Chan PKS, Peiris M, et al. Clinical features and rapid viral diagnosis of human disease associated with avian inuenza A H5N1 virus. Lancet 1998;351:46771. [5] Claas EC, Osterhaus ADM, van Beek R, et al. Human inuenza A H5N1 virus related to a highly pathogenic avian inuenza virus. Lancet 1998;351:4727. [6] Jeerson TO, Demicheli V. The socioeconomics of inuenza. In: Nicholson, Hay, Webster, editors. Textbook of Inuenza. London: Blackwell, 1998. p. 5417. [7] World Health Organisation (WHO). International list of availability of vaccines and sera. Fourth edition. Geneva 1996 (updated February). [8] McDowell I, Newell C, Rosser W. Comparison of three methods of recalling patients for inuenza vaccination. Can Med Assoc J 1986;135:9917. [9] Lukasik MH, Pratt G. The telephone: an overlooked technology for prevention in family medicine. Can Fam Physician 1987;33:19972021. [10] Gerace TM, Sangster JF. Inuenza vaccination: a comparison of two outreach strategies. Fam Med 1988;20:435. [11] Advisory Committee on Immunisation Practices. Prevention and control of inuenza. MMWR 1998;47(3 no RR-6). [12] Gross PA, Hermogenes AW, Sacks HS, et al. The ecacy of inuenza vaccines in elderly people: A meta-analysis and review of the literature. Annals of Internal Medicine 1995;123:51827. [13] Strassburg MA, Greenland S, Sorvillo FJ, et al. Inuenza in the elderly: report of an outbreak and a review of vaccine eectiveness reports. Vaccine 1986;4:3844. [14] Couch R. Summary of medical literature review of eectiveness of inactivated inuenza virus vaccines. In: Cost Eectiveness of Inuenza Vaccination. Washington: Oce of Technology Assessment, 1981. p. 435. [15] Hobson D. Assessment of the ecacy of inuenza vaccines against natural challenge. Develop Biol Standard 1975;28:285 94. [16] Advisory Committee on Immunisation Practices. Prevention and control of inuenza. MMWR 1988;37:36173. [17] Advisory Committee on Immunisation Practices. Prevention and control of inuenza. MMWR 1998;47(3 no RR-6.). [18] Advisory Committee on Immunisation Practices (ACIP). Prevention and control of inuenza: Part II, antiviral agents. MMWR 1994;43:19. [19] Loughlin CA. The discovery and development of therapies for inuenza infections. In: Hannoun C, et al., editors. Options for the control of inuenza. Amsterdam: Elsevier, 1993. p. 32731. [20] Hayden FG, Couch RB. Clinical and epidemiological importance of inuenza A viruses resistant to amantadine and rimantadine. In: Hannoun C, et al., editors. Options for the control of inuenza. Amsterdam: Elsevier, 1993. p. 33342. [21] Wintermeyer SM, Nahata MC. Rimantadine: a clinical perspective. The Annals of Pharmacotherapy 1995;29:299310.
You might also like
- Intrathecal Antibacterial and Antifungal TherapiesDocument24 pagesIntrathecal Antibacterial and Antifungal TherapiesntnquynhproNo ratings yet
- WHO 2019 NCoV Vaccine Effectiveness VE Evaluations 2022.1 EngDocument30 pagesWHO 2019 NCoV Vaccine Effectiveness VE Evaluations 2022.1 EngDhani Rinaldi MaulanaNo ratings yet
- Chemotherapy and febrile neutropenia – Diagnostic and therapeutic managementFrom EverandChemotherapy and febrile neutropenia – Diagnostic and therapeutic managementNo ratings yet
- Guidelines For The Clinical Management of Severe Illness From Influenza Virus InfectionsDocument89 pagesGuidelines For The Clinical Management of Severe Illness From Influenza Virus InfectionsNguyễn Thu TrangNo ratings yet
- Medical treatment and operative repair of abdominal aortic aneurysmsFrom EverandMedical treatment and operative repair of abdominal aortic aneurysmsNo ratings yet
- Antifungicos y Antibioticos IntratecalesDocument24 pagesAntifungicos y Antibioticos IntratecalesRu MNo ratings yet
- Al Musawe2019Document8 pagesAl Musawe2019Jesus CarvalhoNo ratings yet
- Contents - Part 1: 1 Infection Control Strategy 1-1Document51 pagesContents - Part 1: 1 Infection Control Strategy 1-1Arie KusumodewiNo ratings yet
- WHO Vaccine Manual PDFDocument112 pagesWHO Vaccine Manual PDFRagel CorpsNo ratings yet
- Catheter-Associated UrinaryDocument78 pagesCatheter-Associated UrinaryFaozan FikriNo ratings yet
- Cardiothoracic Care for Children and Young People: A Multidisciplinary ApproachFrom EverandCardiothoracic Care for Children and Young People: A Multidisciplinary ApproachKerry CookNo ratings yet
- Evaluation and Optimization of Laboratory Methods and Analytical ProceduresFrom EverandEvaluation and Optimization of Laboratory Methods and Analytical ProceduresNo ratings yet
- Astpreg FullDocument72 pagesAstpreg FullDeni Andre AtmadinataNo ratings yet
- Autoimmune Hepatitis, Overlap Syndrome, Primary Sclerosing Cholangitis and Primary Biliary Cirrhosis in Clinical PracticeFrom EverandAutoimmune Hepatitis, Overlap Syndrome, Primary Sclerosing Cholangitis and Primary Biliary Cirrhosis in Clinical PracticeNo ratings yet
- Remdesivir Against Covid19Document21 pagesRemdesivir Against Covid19elsie versieNo ratings yet
- Effectiveness Sterile NeedleDocument61 pagesEffectiveness Sterile NeedleDescriminalización.orgNo ratings yet
- Bernhard Et AlDocument13 pagesBernhard Et AlPramod N KNo ratings yet
- Barium and Barium Compounds: Concise International Chemical Assessment Document 33Document57 pagesBarium and Barium Compounds: Concise International Chemical Assessment Document 33Javad MousavyNo ratings yet
- Normansell Et Al-2015-Cochrane Database of Systematic ReviewsDocument152 pagesNormansell Et Al-2015-Cochrane Database of Systematic ReviewsfiskaderishaNo ratings yet
- WHO 2019 nCoV Vaccine Effectiveness Measurement 2021.1 EngDocument70 pagesWHO 2019 nCoV Vaccine Effectiveness Measurement 2021.1 EngChio MoranteNo ratings yet
- Antibióticos para La Neumonía Asociada Al Ventilador.Document96 pagesAntibióticos para La Neumonía Asociada Al Ventilador.Julio GonzalesNo ratings yet
- Lengkap PusingDocument52 pagesLengkap PusingAyuNo ratings yet
- Rizzieri 2016Document13 pagesRizzieri 2016alinamatei1000000No ratings yet
- Clinical Educators Guide 2010Document20 pagesClinical Educators Guide 2010PPINo ratings yet
- Immunosensors For Detection of Pesticide ResiduesDocument11 pagesImmunosensors For Detection of Pesticide Residuescatherine_henry-de-villeneuveNo ratings yet
- Ber IliumDocument76 pagesBer IliumMulki RachmawatiNo ratings yet
- Deficiencies of the Urea Cycle - Clinical Significance and TherapyFrom EverandDeficiencies of the Urea Cycle - Clinical Significance and TherapyNo ratings yet
- Aftryp SWG PDFDocument182 pagesAftryp SWG PDFij EducationNo ratings yet
- Healthcare Waste Management in IndiaDocument11 pagesHealthcare Waste Management in IndiaSunny Naresh ManchandaNo ratings yet
- 2023 CPG On The Management of Atherosclerotic Carotid and Vertebral Artery DiseaseDocument105 pages2023 CPG On The Management of Atherosclerotic Carotid and Vertebral Artery DiseaseElisa NovaesNo ratings yet
- Guidelines For The Management of Multidrug-Resistant Tuberculosis in MyanmarDocument192 pagesGuidelines For The Management of Multidrug-Resistant Tuberculosis in MyanmarAdhi PradanaNo ratings yet
- Carotid ESVS 2018Document79 pagesCarotid ESVS 2018Ahmed ElmallahNo ratings yet
- Sap 000Document164 pagesSap 000pathuri rangaNo ratings yet
- Retention and Selectivity in Liquid Chromatography: Prediction, Standardisation and Phase ComparisonsFrom EverandRetention and Selectivity in Liquid Chromatography: Prediction, Standardisation and Phase ComparisonsNo ratings yet
- Clinical Microbiology Reviews-2019-Baird-e00011-19.full PDFDocument68 pagesClinical Microbiology Reviews-2019-Baird-e00011-19.full PDFMahesa Kurnianti PutriNo ratings yet
- N207917 Adapalene and Benzoyl Peroxide Clinical PREA 2 PDFDocument49 pagesN207917 Adapalene and Benzoyl Peroxide Clinical PREA 2 PDFKing MatNo ratings yet
- SpanacDocument127 pagesSpanacTimothy BensonNo ratings yet
- Farmacocinetica y Farmacodinami de MMF Clin Pharmacokinet 2007 46 1 13-58Document46 pagesFarmacocinetica y Farmacodinami de MMF Clin Pharmacokinet 2007 46 1 13-58Maria Marina Papaginovic LeivaNo ratings yet
- Prima PDFDocument173 pagesPrima PDFnafisNo ratings yet
- Izazovi U Menadzmentu Snabdevanja Lekovima Indija - SHAMIMA TAYOB FINAL EXAMDocument221 pagesIzazovi U Menadzmentu Snabdevanja Lekovima Indija - SHAMIMA TAYOB FINAL EXAMHokusyNo ratings yet
- Childhood MedulloblastmaDocument17 pagesChildhood MedulloblastmaIrenaNo ratings yet
- The Intensive Care Unit MaualDocument356 pagesThe Intensive Care Unit MaualMariefel Villanueva AlejagaNo ratings yet
- Asthama in ElderlyDocument72 pagesAsthama in ElderlyboyzonerajNo ratings yet
- Technical Guide: Sputum Examination For Tuberculosis by Direct Microscopy in Low Income CountriesDocument32 pagesTechnical Guide: Sputum Examination For Tuberculosis by Direct Microscopy in Low Income CountriesRevix Adalah Ita'No ratings yet
- C Ovid 19 Treatment GuidelinesDocument459 pagesC Ovid 19 Treatment GuidelinesRamya RSNo ratings yet
- Kardiovaskular 1Document92 pagesKardiovaskular 1419022 MELA ANANDA PUTRIANANo ratings yet
- Effectiveness of Homeopathy For Clinical Conditions - Evaluation of The Evidence PDFDocument301 pagesEffectiveness of Homeopathy For Clinical Conditions - Evaluation of The Evidence PDFYaniv AlgrablyNo ratings yet
- Poultry Subsector in Tanzania Final ReportDocument44 pagesPoultry Subsector in Tanzania Final ReportRika YamazakiNo ratings yet
- Managemen of Vascular Graft and Stent Graft Infections Mar 2020Document46 pagesManagemen of Vascular Graft and Stent Graft Infections Mar 2020GhaithNo ratings yet
- Msds BenzeneDocument32 pagesMsds BenzeneMertcan AslanNo ratings yet
- Central Bicol Masterlist Sort AddressDocument6 pagesCentral Bicol Masterlist Sort Addresskentclark03No ratings yet
- Eye Movement Desensitization Reprocessing For Children and Adolescents With Posttraumatic Stress Disorder: A Systematic Narrative ReviewDocument14 pagesEye Movement Desensitization Reprocessing For Children and Adolescents With Posttraumatic Stress Disorder: A Systematic Narrative ReviewNerea F GNo ratings yet
- Endodontic Treatment in Single and Multiple Visits - An Overview of Systematic Reviews (1138)Document7 pagesEndodontic Treatment in Single and Multiple Visits - An Overview of Systematic Reviews (1138)alondraNo ratings yet
- Sudden Death During Sport Activities A Malaysian PerspectiveDocument10 pagesSudden Death During Sport Activities A Malaysian PerspectiveRosaniza KamarudinNo ratings yet
- Color Atlas & Synopsis of Clinical Ophthalmology - Wills Eye Institute CorneaDocument384 pagesColor Atlas & Synopsis of Clinical Ophthalmology - Wills Eye Institute Corneam.No ratings yet
- Peperiksaan Percubaan SPM 2008 Marking Scheme English For Science andDocument3 pagesPeperiksaan Percubaan SPM 2008 Marking Scheme English For Science andkamil muhammadNo ratings yet
- HES 005 Session 6 SASDocument10 pagesHES 005 Session 6 SASG INo ratings yet
- 2022 Year 10 Camp EXTREMEDocument11 pages2022 Year 10 Camp EXTREMEJohn BroughtonNo ratings yet
- Polyhydramnios Sem5Document9 pagesPolyhydramnios Sem5Siti Nur AmirahNo ratings yet
- Brochure Arogya Sanjeevani Policy V 1 0204 WebDocument9 pagesBrochure Arogya Sanjeevani Policy V 1 0204 Webshaheen moideenNo ratings yet
- Disturbed Sensory PerceptionDocument2 pagesDisturbed Sensory Perceptionsuper ahga-once0% (1)
- GliclazideDocument2 pagesGliclazideNicholas Tagle100% (1)
- Lab Act Introduction Hemostasis Bleeding Time Tourniquet Test Week 4Document23 pagesLab Act Introduction Hemostasis Bleeding Time Tourniquet Test Week 4Arief AbidinNo ratings yet
- 128 HZ Tuning Fork A Screening Tool For Diabetic NeuropathyDocument4 pages128 HZ Tuning Fork A Screening Tool For Diabetic NeuropathyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- 87-Article Text-892-1-10-20210531Document12 pages87-Article Text-892-1-10-20210531Nurul HidayatiNo ratings yet
- USG THYROID PPT 1Document42 pagesUSG THYROID PPT 1Jahanavi JaluNo ratings yet
- 19 Ag 10 PDFDocument4 pages19 Ag 10 PDFfebyan yohanesNo ratings yet
- MantulDocument4 pagesMantulAbba PothetNo ratings yet
- Kashmir Healthline - IIDocument20 pagesKashmir Healthline - IIKashmir WatchNo ratings yet
- cc2019b1 SampleDocument27 pagescc2019b1 SampletanjudinNo ratings yet
- Notre Dame of Educational Association.Document10 pagesNotre Dame of Educational Association.Maui TingNo ratings yet
- Test Name Result Flag Reference Range Lab: Patient InformationDocument1 pageTest Name Result Flag Reference Range Lab: Patient InformationRaquel LujanNo ratings yet
- ResumeDocument4 pagesResumeAizack Gavrielle AbenganaNo ratings yet
- Nano Technology in MedicineDocument23 pagesNano Technology in MedicineAmitoj Singh100% (1)
- Ministry of Health & Family Welfare: Directorate General of CGHSDocument47 pagesMinistry of Health & Family Welfare: Directorate General of CGHSRahulTanejaNo ratings yet
- National Consumer Disputes Redressal Commission New Delhi Consumer Case No. 173 of 2011Document7 pagesNational Consumer Disputes Redressal Commission New Delhi Consumer Case No. 173 of 2011Arnav JoshiNo ratings yet
- K12 Grade 8 - Health (Curriculum Guide)Document7 pagesK12 Grade 8 - Health (Curriculum Guide)DepEdResources100% (21)
- Full-Sentence Speech FinalDocument2 pagesFull-Sentence Speech Finalapi-363883917No ratings yet
- Antibiotics 101Document49 pagesAntibiotics 101Tony VoNo ratings yet
- Hepatic Cysts Workup: Approach ConsiderationsDocument4 pagesHepatic Cysts Workup: Approach ConsiderationsMariska JuanitaNo ratings yet