You might also like
- Ews Workshop Jcca Nov 2016Document56 pagesEws Workshop Jcca Nov 2016rezaNo ratings yet
- Obstetrical Hemorrhage: Reynold John D. ValenciaDocument82 pagesObstetrical Hemorrhage: Reynold John D. ValenciaReynold John ValenciaNo ratings yet
- mATERI PDTDocument58 pagesmATERI PDTdebieNo ratings yet
- SEPSIS Kuliah Prof Herdiman (S1) RevDocument41 pagesSEPSIS Kuliah Prof Herdiman (S1) RevSianipar Mangara Wahyu CharrosNo ratings yet
- Materi WS EWS 2018 - Dr. Raphael - CPR Update JCCA RPPDocument34 pagesMateri WS EWS 2018 - Dr. Raphael - CPR Update JCCA RPPMuhammadHazmiAnzhariNo ratings yet
- Managing Brain Injury AnesthesiaDocument62 pagesManaging Brain Injury AnesthesiaKelvin KelvinNo ratings yet
- Sepsis 1Document6 pagesSepsis 1icu demangNo ratings yet
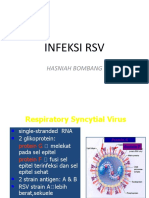
- Infeksi RSV: Hasniah BombangDocument12 pagesInfeksi RSV: Hasniah Bombangmuh hardiansyahNo ratings yet
- Electrical Cardiometry Parameter DefinitionsDocument21 pagesElectrical Cardiometry Parameter DefinitionsEveline FebrinaNo ratings yet
- Airway in Critical Care For GP RSUIDocument29 pagesAirway in Critical Care For GP RSUISeptiana Rizki FauziahNo ratings yet
- Transporting Critically Ill PatientsDocument48 pagesTransporting Critically Ill PatientsRichard GunawanNo ratings yet
- Free Paper Abstract BookDocument1,047 pagesFree Paper Abstract Bookkukadiya100% (1)
- Volume Resuscitation in Shock State Ppds I Prof HanafiDocument78 pagesVolume Resuscitation in Shock State Ppds I Prof HanafiAhmad RidwanNo ratings yet
- Neonatal ProceduresDocument74 pagesNeonatal ProceduresIbrahim Sabra100% (1)
- (FINAL) PK PD of Antimicrobials in Septic Pts - YDT 240721 - WatermarkDocument40 pages(FINAL) PK PD of Antimicrobials in Septic Pts - YDT 240721 - Watermarklia pramudha wardhaniNo ratings yet
- CNEP Guide to Code Blue ResponseDocument93 pagesCNEP Guide to Code Blue ResponsedindaNo ratings yet
- Amniotic Fluid Embolism: Women's Hospital School of Medicine Zhejiang Un Iversity Wang ZhengpingDocument19 pagesAmniotic Fluid Embolism: Women's Hospital School of Medicine Zhejiang Un Iversity Wang ZhengpingPoonam RanaNo ratings yet
- Anaesthesia SummaryDocument36 pagesAnaesthesia SummaryRazan QassemNo ratings yet
- SepsisDocument14 pagesSepsisyreshgemNo ratings yet
- Mengenal Resusitasi Pada Anak Dan Bayi Bagi Perawat PemulaDocument15 pagesMengenal Resusitasi Pada Anak Dan Bayi Bagi Perawat PemulaSiti Krisan WijayaNo ratings yet
- Manajemen Disritmia Kardiak IntraoperatifDocument53 pagesManajemen Disritmia Kardiak IntraoperatifAbi FaizNo ratings yet
- Agustus Monitoring HemodinamikDocument61 pagesAgustus Monitoring HemodinamikFikriYTNo ratings yet
- Resusitasi NeonatusDocument22 pagesResusitasi NeonatusnikkitaihsanNo ratings yet
- NEC in Preterm InfantsDocument2 pagesNEC in Preterm InfantsJDRN14No ratings yet
- Amniotic Fluid EmbolismDocument18 pagesAmniotic Fluid EmbolismmanjuNo ratings yet
- Principals of Mechanical Ventilation in Neonates: DR Mohd Maghayreh PRTH - IrbidDocument78 pagesPrincipals of Mechanical Ventilation in Neonates: DR Mohd Maghayreh PRTH - IrbidAnonymous 58LGc3No ratings yet
- Dr. Shaker's Guide to Managing Cyanotic Heart DiseaseDocument66 pagesDr. Shaker's Guide to Managing Cyanotic Heart DiseasePrasanth SankarNo ratings yet
- Say No To Code Blue, Say YesDocument36 pagesSay No To Code Blue, Say YesTheodorus PY PranotoNo ratings yet
- Perioperative Fluid Management in Pediatrics: By: Karim Kamal, MDDocument33 pagesPerioperative Fluid Management in Pediatrics: By: Karim Kamal, MDMohammed AKNo ratings yet
- Abg AnalysisDocument43 pagesAbg AnalysisHakuna MatataNo ratings yet
- Pregnancy With MS MRDocument74 pagesPregnancy With MS MRRaj K SharmaNo ratings yet
- Gestational Age Related Problems of The Newborn: Carla Reinke, RN, MN, Arnp, CNMDocument120 pagesGestational Age Related Problems of The Newborn: Carla Reinke, RN, MN, Arnp, CNMsulekhaanoobNo ratings yet
- Acute Respiratory FailureDocument29 pagesAcute Respiratory FailurePIYALI BISWASNo ratings yet
- Neonatal CareDocument59 pagesNeonatal CareKeith LajotNo ratings yet
- Cerebrospinal Meningitis (CSM) : Adwoa Baffour AwuahDocument38 pagesCerebrospinal Meningitis (CSM) : Adwoa Baffour AwuahMichael Adjei100% (1)
- Massive TransfusionDocument104 pagesMassive Transfusionbingkydoodle1012No ratings yet
- Approach Cyanosis FinalDocument31 pagesApproach Cyanosis Finalsuheena.CNo ratings yet
- Respiratory Distress Syndrome: Islamic University Nursing CollegeDocument21 pagesRespiratory Distress Syndrome: Islamic University Nursing Collegeyaumil agisnaNo ratings yet
- Challenges In Obstetric Anesthesia: 10 Key Issues for CRNAsDocument38 pagesChallenges In Obstetric Anesthesia: 10 Key Issues for CRNAsPaulHerreraNo ratings yet
- DIVITI Slide Prophylaxis VTE SPPD Ringkas-1Document11 pagesDIVITI Slide Prophylaxis VTE SPPD Ringkas-1Fera NurrizaNo ratings yet
- Malaysiantriagescalenewrevised2019!1!221014090642 28d8e1aeDocument18 pagesMalaysiantriagescalenewrevised2019!1!221014090642 28d8e1aenaqibsakila4286No ratings yet
- Non-Cyanotic Congenital Heart Disease-UpDate 4-22-53Document136 pagesNon-Cyanotic Congenital Heart Disease-UpDate 4-22-53getnusNo ratings yet
- Fluid Balance and Venous Access in ChildrenDocument51 pagesFluid Balance and Venous Access in Childrenhayssam rashwan100% (1)
- Airway Control Management, RSPMDocument59 pagesAirway Control Management, RSPMzakia4nisakNo ratings yet
- Lec#10Document30 pagesLec#10hani bilalNo ratings yet
- Ductus Arteriosus Dependent Congenital Heart Disease: Amjad Kouatli MD. FAAP. FACCDocument28 pagesDuctus Arteriosus Dependent Congenital Heart Disease: Amjad Kouatli MD. FAAP. FACCKartik KumarasamyNo ratings yet
- Prevention & Treatment of Rop: Presentation: DR Manaswinee Sahoo Guide: DR Swati UpadhyayDocument42 pagesPrevention & Treatment of Rop: Presentation: DR Manaswinee Sahoo Guide: DR Swati Upadhyaypranaya mallNo ratings yet
- VAP SlidesDocument25 pagesVAP SlidesGladys OliviaNo ratings yet
- Vdocument - in Physiological Changes in Pregnancy 5584a97a1a6f9Document34 pagesVdocument - in Physiological Changes in Pregnancy 5584a97a1a6f9Bader AlqattanNo ratings yet
- Disseminated Intravascular CoagulationDocument16 pagesDisseminated Intravascular CoagulationDocRNNo ratings yet
- Mechanical Ventilation and Intracranial PressureDocument30 pagesMechanical Ventilation and Intracranial PressureFlavius AnghelNo ratings yet
- 04.06.2018 - 6 - V. Kushakovsky - Pediatric AnaesthesiaDocument46 pages04.06.2018 - 6 - V. Kushakovsky - Pediatric AnaesthesiaPhilippe KinnaerNo ratings yet
- Regional Anesthesia Techniques - Spinal, Epidural, and Nerve BlocksDocument76 pagesRegional Anesthesia Techniques - Spinal, Epidural, and Nerve BlocksjanaNo ratings yet
- European Consensus On The Management of RDSDocument41 pagesEuropean Consensus On The Management of RDSDeddy Supriyadi100% (1)
- NEONATAL HYPOGLYCAEMIA: CAUSES, SIGNS AND MANAGEMENTDocument31 pagesNEONATAL HYPOGLYCAEMIA: CAUSES, SIGNS AND MANAGEMENTJian Han LiewNo ratings yet
- The Nurses and Midwives Act No. 10 of 2019. PMDDocument43 pagesThe Nurses and Midwives Act No. 10 of 2019. PMDhfcvbNo ratings yet
- Close Chest Tube Insertion ThoracostomyDocument15 pagesClose Chest Tube Insertion ThoracostomyMae Navidas DigdiganNo ratings yet
- Neonatal Emergencies FinalDocument90 pagesNeonatal Emergencies FinalDr Raseena VattamkandathilNo ratings yet
- Understanding Mechanical Ventilation Modes & WeaningDocument52 pagesUnderstanding Mechanical Ventilation Modes & WeaningDeepa BhattacharjeeNo ratings yet
- Vitiligo in Adults and Children PDFDocument28 pagesVitiligo in Adults and Children PDFFatahillah NazarNo ratings yet
- Vitiligo in Adults and Children PDFDocument28 pagesVitiligo in Adults and Children PDFFatahillah NazarNo ratings yet
- Tinea Versicolor An Epidemiology 1948 5948.1000010Document6 pagesTinea Versicolor An Epidemiology 1948 5948.1000010Fatahillah NazarNo ratings yet
- Clinical Pathway Pneumonia Komunitas 2Document17 pagesClinical Pathway Pneumonia Komunitas 2Fatahillah Nazar100% (1)
- SICH Mgmt2Document9 pagesSICH Mgmt2Lennon Ponta-oyNo ratings yet
- Clinical pathway for mild-moderate acute diarrheaDocument14 pagesClinical pathway for mild-moderate acute diarrheaFatahillah Nazar100% (1)
- Article WJPR 1409139461Document10 pagesArticle WJPR 1409139461syafahalimNo ratings yet
- ABC of Sexually Transmitted InfectionsDocument99 pagesABC of Sexually Transmitted InfectionsPriscilia FooNo ratings yet
- Elston2013 PDFDocument9 pagesElston2013 PDFFatahillah NazarNo ratings yet
- Program Peningkatan Mutu dan Keselamatan PasienDocument28 pagesProgram Peningkatan Mutu dan Keselamatan PasienFatahillah Nazar0% (1)
- CLINICAL PATHWAY Hernia Inguinalis Diedit PPKnyaDocument14 pagesCLINICAL PATHWAY Hernia Inguinalis Diedit PPKnyaFatahillah NazarNo ratings yet
- Audit CP Dokter. Revisi 05-09-17Document84 pagesAudit CP Dokter. Revisi 05-09-17Fatahillah NazarNo ratings yet
- Lampiran Pasient SafetyDocument2 pagesLampiran Pasient SafetyFatahillah NazarNo ratings yet
- Clinical Pathway Demam Tifod by KarsDocument15 pagesClinical Pathway Demam Tifod by KarsFatahillah NazarNo ratings yet
- Trauma Saraf SpinalDocument41 pagesTrauma Saraf SpinalFatahillah NazarNo ratings yet
- TrebleDocument1 pageTrebleFatahillah NazarNo ratings yet
- Pocket Emergency Paediatric CareDocument217 pagesPocket Emergency Paediatric Careapi-26171905No ratings yet
- Core Competency Matrix FinalDocument2 pagesCore Competency Matrix Finalpenunjang medikNo ratings yet
- Dr. Raihan, Sp.ADocument68 pagesDr. Raihan, Sp.AFatahillah NazarNo ratings yet
- Mengenali Kegawatan Dengue 2013Document40 pagesMengenali Kegawatan Dengue 2013Fatahillah NazarNo ratings yet
- Cardio Pulmonary R Ry Resuscitation 2010Document26 pagesCardio Pulmonary R Ry Resuscitation 2010Fatahillah NazarNo ratings yet
- Gels III Fluid TherDocument57 pagesGels III Fluid TherFatahillah NazarNo ratings yet
- Gels III Fluid TherDocument57 pagesGels III Fluid TherFatahillah NazarNo ratings yet
- Gels I AbDocument65 pagesGels I AbFatahillah NazarNo ratings yet
- Acute Coronary Syndrome 052014Document91 pagesAcute Coronary Syndrome 052014Fatahillah NazarNo ratings yet
- Surgical Skills PracticumDocument7 pagesSurgical Skills PracticumFatahillah NazarNo ratings yet
- PlavixDocument80 pagesPlavixFatahillah NazarNo ratings yet
- Asama PosterDocument1 pageAsama Postershuvojit moulikNo ratings yet
- Pharmacology Lab (1) : Routes of Drug AdministrationDocument14 pagesPharmacology Lab (1) : Routes of Drug AdministrationBotan AbdullahNo ratings yet
- 11.efficacy and Stability of The Alar Base Cinch SutureDocument4 pages11.efficacy and Stability of The Alar Base Cinch SutureFabian Camelo OtorrinoNo ratings yet
- Expanding Consensus in Portal HypertensionDocument29 pagesExpanding Consensus in Portal HypertensionJosé Pepo Apey Reinoso100% (1)
- Ophthalmology Set 8Document5 pagesOphthalmology Set 8ajay khadeNo ratings yet
- Rubrics Normal DeliveryDocument3 pagesRubrics Normal DeliveryKYLE MITZIE SENGCONo ratings yet
- Implant Failure and ManagementDocument59 pagesImplant Failure and ManagementDrIbrahimShaikh0% (1)
- Randomized, Placebo-Controlled Trial of Xyloglucan and Gelose For The Treatment of Acute Diarrhea in ChildrenDocument8 pagesRandomized, Placebo-Controlled Trial of Xyloglucan and Gelose For The Treatment of Acute Diarrhea in ChildrenvalenciaNo ratings yet
- Postpartum Purulent-Septic Diseases (Peritonitis, Sepsis, Toxic-Infectious Shock)Document64 pagesPostpartum Purulent-Septic Diseases (Peritonitis, Sepsis, Toxic-Infectious Shock)Muhammed ElnakibNo ratings yet
- The Paleopathology of Specific Infectious Diseases From Southeastern Hungary: A Brief OverviewDocument6 pagesThe Paleopathology of Specific Infectious Diseases From Southeastern Hungary: A Brief OverviewLucía Chavarría RíosNo ratings yet
- Demodex CanisDocument19 pagesDemodex Canisapi-337841627No ratings yet
- Efficacy and Safety of Rabeprazole in Children.20Document10 pagesEfficacy and Safety of Rabeprazole in Children.20Ismy HoiriyahNo ratings yet
- Essential Intrapartum and Newborn Care (EINC) Bulletin 1Document10 pagesEssential Intrapartum and Newborn Care (EINC) Bulletin 1maxicap7386% (7)
- Distraksi Menonton Efektif Menurunkan Nyeri Ringan Pasien: Congestive Heart Failure (CHF)Document7 pagesDistraksi Menonton Efektif Menurunkan Nyeri Ringan Pasien: Congestive Heart Failure (CHF)Devy YahyaNo ratings yet
- Nursing Skills Checklist - RTDocument6 pagesNursing Skills Checklist - RTapi-309674272No ratings yet
- MOH, DHA and HAAD recalls from 2017 WhatsApp groupDocument32 pagesMOH, DHA and HAAD recalls from 2017 WhatsApp groupshahzadNo ratings yet
- Scientists transform spinach leaf into beating human heart tissueDocument4 pagesScientists transform spinach leaf into beating human heart tissueSkye M. PetersNo ratings yet
- Eight Hallmarks of Cancer ExplainedDocument40 pagesEight Hallmarks of Cancer ExplainedArnab KalitaNo ratings yet
- Skills Math WorksheetDocument4 pagesSkills Math WorksheetBrennan MaguireNo ratings yet
- Biosure RGDocument2 pagesBiosure RGJuan Martinez Del AngelNo ratings yet
- REFKAS - Dr. LusitoDocument43 pagesREFKAS - Dr. LusitoRizal LuthfiNo ratings yet
- SDL 3 MCN 1Document3 pagesSDL 3 MCN 1Milagros Florita100% (1)
- Greater Political ParticipationDocument12 pagesGreater Political ParticipationBe-COOL State Of MindNo ratings yet
- 2013 Pankaj R BodadeDocument8 pages2013 Pankaj R BodadeGeorge StoicaNo ratings yet
- Maternity Clinical Network Contact DetailsDocument18 pagesMaternity Clinical Network Contact DetailsAlina-Gabriela MarinNo ratings yet
- Arterial DiseaseDocument191 pagesArterial DiseaseAura DiscyacittaNo ratings yet
- Annex A. ChecklistDocument2 pagesAnnex A. ChecklistroseannurakNo ratings yet
- Hormonal Replacement Therapy Lesson PlanDocument9 pagesHormonal Replacement Therapy Lesson PlanBaljinder kaurNo ratings yet
- Clinical Laboratory TransesDocument2 pagesClinical Laboratory TransesjulianneNo ratings yet
- 3.2. The Hospital Medical VocabularyDocument7 pages3.2. The Hospital Medical VocabularyMarkus ZahndNo ratings yet