You might also like
- Guidelines for Measuring Household and Individual Dietary DiversityFrom EverandGuidelines for Measuring Household and Individual Dietary DiversityNo ratings yet
- Basics of Therapeutic DietsDocument12 pagesBasics of Therapeutic DietstiruchanurNo ratings yet
- Soft Diet Guide for Easy Chewing and DigestionDocument11 pagesSoft Diet Guide for Easy Chewing and Digestionrlinao100% (1)
- Dorothea Orems Theory of Self Care DeficitDocument35 pagesDorothea Orems Theory of Self Care DeficitDiah Permata SariNo ratings yet
- Roth 10e Nclex Chapter 17Document4 pagesRoth 10e Nclex Chapter 17jennaaahhhNo ratings yet
- Enteral NutritionDocument73 pagesEnteral NutritionYosep SutandarNo ratings yet
- NCMA215 Course Task 6 Food Exchange List and Calorie AnalysisDocument4 pagesNCMA215 Course Task 6 Food Exchange List and Calorie AnalysisMIGUEL MORANo ratings yet
- Clinical Nutrition ManagementDocument458 pagesClinical Nutrition Managementlouise kartika100% (1)
- Nutritional Assessment MethodsDocument2 pagesNutritional Assessment Methodsyaleconsultancy100% (4)
- Dietary Standard RDADocument24 pagesDietary Standard RDANurul Afifah50% (2)
- AdimeDocument2 pagesAdimeapi-276849892No ratings yet
- Drug StudyDocument28 pagesDrug StudyJheryck SabadaoNo ratings yet
- PreschoolDocument40 pagesPreschoolosamaNo ratings yet
- NUR100 Sherpath CH 3 Community Based Nursing Public Health NursingDocument12 pagesNUR100 Sherpath CH 3 Community Based Nursing Public Health Nursingcaloy2345caloyNo ratings yet
- TPN CalculationsDocument4 pagesTPN Calculationsapi-293416259100% (1)
- Caring for Chronic Illness and the ElderlyDocument5 pagesCaring for Chronic Illness and the Elderlykamae_27No ratings yet
- Chapter 1 - Health Care Delivery and Nursing PracticeDocument4 pagesChapter 1 - Health Care Delivery and Nursing Practicejane amosNo ratings yet
- Painless Evidence-Based MedicineFrom EverandPainless Evidence-Based MedicineAntonio L. DansNo ratings yet
- Obesity and Esophageal DisordersFrom EverandObesity and Esophageal DisordersDhyanesh PatelNo ratings yet
- Allama Iqbal Open University, IslamabadDocument22 pagesAllama Iqbal Open University, Islamabadazeem dilawarNo ratings yet
- Am J Clin Nutr 2005 Wilson 1074 81Document8 pagesAm J Clin Nutr 2005 Wilson 1074 81Ilmi Dewi ANo ratings yet
- MST Nursing HandoutDocument3 pagesMST Nursing Handoutapi-261265221No ratings yet
- Mini Nutritional AssessmentDocument7 pagesMini Nutritional AssessmentJoão Mariano SantosNo ratings yet
- 337.1 s2.0 S0002916522046718 MainDocument10 pages337.1 s2.0 S0002916522046718 MaintereNo ratings yet
- Nutrition JournalDocument46 pagesNutrition JournaldesiNo ratings yet
- Working Together To Tackle Obesity in Adult Mental Health Secure UnitsDocument20 pagesWorking Together To Tackle Obesity in Adult Mental Health Secure UnitsDaniel DubeNo ratings yet
- Special Article: Preliminary Remarks Guideline Limitations Target AudienceDocument5 pagesSpecial Article: Preliminary Remarks Guideline Limitations Target AudiencegreencoleNo ratings yet
- Symposium: Challenges in Targeting Nutrition ProgramsDocument5 pagesSymposium: Challenges in Targeting Nutrition ProgramsMukhlidahHanunSiregarNo ratings yet
- Nutrition 508 CompliantDocument3 pagesNutrition 508 CompliantDr. Mohammed MahfoozNo ratings yet
- FANTASTIC Lifestyle AssessmentDocument6 pagesFANTASTIC Lifestyle AssessmentzacNo ratings yet
- Macronutrients, Food Groups, and Eating Patterns in The Management of DiabetesDocument12 pagesMacronutrients, Food Groups, and Eating Patterns in The Management of Diabetesannaafia69969No ratings yet
- Postpartum care for women with gestational diabetesDocument10 pagesPostpartum care for women with gestational diabetesA.No ratings yet
- Association of Self-Efficacy and Self-Care With Glycemic Control in DiabetesDocument7 pagesAssociation of Self-Efficacy and Self-Care With Glycemic Control in DiabetesSeptian M SNo ratings yet
- Nutrition Now - Enhancing Nutritional Care - RCNDocument36 pagesNutrition Now - Enhancing Nutritional Care - RCNNeha BhartiNo ratings yet
- Development and validation of the SNAQr hospital malnutrition screening toolDocument8 pagesDevelopment and validation of the SNAQr hospital malnutrition screening toolDanang Adit KuranaNo ratings yet
- Thigpen Matt CurriculumDocument12 pagesThigpen Matt Curriculumapi-261193383No ratings yet
- Nutritional Comparison of Obese and Non-Obese Female StudentsDocument37 pagesNutritional Comparison of Obese and Non-Obese Female StudentsJaspreet SinghNo ratings yet
- Nutrition Screening AssesmentDocument11 pagesNutrition Screening AssesmentIrving EuanNo ratings yet
- Artikel Pubmed 3Document6 pagesArtikel Pubmed 3Sofa AmaliaNo ratings yet
- Screening for Diabetes in Youth Evidence ReviewDocument127 pagesScreening for Diabetes in Youth Evidence Reviewtechindia2010No ratings yet
- Research Clinical 1 1Document18 pagesResearch Clinical 1 1api-459656816No ratings yet
- Mini Nutrition Assessment PDFDocument2 pagesMini Nutrition Assessment PDFDiyah RahmawatiNo ratings yet
- International Journal of Gerontology: Thiago J. Avelino-Silva, Omar JaluulDocument6 pagesInternational Journal of Gerontology: Thiago J. Avelino-Silva, Omar JaluulKaye Antonette AntioquiaNo ratings yet
- Self Help For Bulimia NervosaDocument6 pagesSelf Help For Bulimia NervosaAnonymous lNDP8O6TNo ratings yet
- Assessment of The Perceived Quality of Life of Non Insulin Dependent Diabetic Patients Attending The Diabetes Clinic in Kenyatta National HospitalDocument7 pagesAssessment of The Perceived Quality of Life of Non Insulin Dependent Diabetic Patients Attending The Diabetes Clinic in Kenyatta National HospitalIOSR Journal of PharmacyNo ratings yet
- Diet Quality of US Adolescents During The Transition To Adulthood: Changes and PredictorsDocument9 pagesDiet Quality of US Adolescents During The Transition To Adulthood: Changes and PredictorsmiraandrianiNo ratings yet
- DM Self AssessmentDocument6 pagesDM Self AssessmentruguNo ratings yet
- E827 FullDocument15 pagesE827 FullNeo YustindraNo ratings yet
- Ebp Team Assignment Group 10Document15 pagesEbp Team Assignment Group 10api-621785757No ratings yet
- A S P E N Clinical Guidelines - Nutrition Support of The Critically Ill ChildDocument56 pagesA S P E N Clinical Guidelines - Nutrition Support of The Critically Ill ChildPaulina Kristiani BangunNo ratings yet
- Clinical Nutrition: ESPEN Endorsed RecommendationDocument9 pagesClinical Nutrition: ESPEN Endorsed RecommendationjavierNo ratings yet
- Test Bank Medical Surgical Nursing Clinical Reasoning in Patient Care 6th Lemone Burke Bauldoff GubrudDocument60 pagesTest Bank Medical Surgical Nursing Clinical Reasoning in Patient Care 6th Lemone Burke Bauldoff GubrudMichaelBlairozrc100% (26)
- Validacion Del Criterio de Evaluacion Nut Global Del Adulto Mayor Chile 2001Document7 pagesValidacion Del Criterio de Evaluacion Nut Global Del Adulto Mayor Chile 2001Joanna Rudman AbzaradelNo ratings yet
- Pediatrics 2007 Barlow S164 92Document31 pagesPediatrics 2007 Barlow S164 92John'sSujonoNo ratings yet
- Recommendation Report DiMeglioDocument14 pagesRecommendation Report DiMeglioMarie DiMeglioNo ratings yet
- Hea 648 Final RommDocument25 pagesHea 648 Final Rommapi-293251016No ratings yet
- Small Animal Clinical Nutrition 5thDocument21 pagesSmall Animal Clinical Nutrition 5thJairo Pereira100% (1)
- Full Download Test Bank For Lutzs Nutrition and Diet Therapy 7th by Mazur PDF Full ChapterDocument14 pagesFull Download Test Bank For Lutzs Nutrition and Diet Therapy 7th by Mazur PDF Full Chapterexequycheluract6oi100% (17)
- Action Stat Aspiration Pneumonia.21Document1 pageAction Stat Aspiration Pneumonia.21vincesumergidoNo ratings yet
- Trauma - Paediatric Chest Trauma (Part 1) Initial Lethal InjuriesDocument13 pagesTrauma - Paediatric Chest Trauma (Part 1) Initial Lethal InjuriesvincesumergidoNo ratings yet
- Trauma Sellick's ManoeuvreDocument4 pagesTrauma Sellick's ManoeuvrevincesumergidoNo ratings yet
- Oncology (Pediatric) - Nutritional Issues in Adolescents After Bone Marrow Transplant, A Literature ReviewDocument12 pagesOncology (Pediatric) - Nutritional Issues in Adolescents After Bone Marrow Transplant, A Literature Reviewvincesumergido100% (1)
- Your Guide To Certification.6Document1 pageYour Guide To Certification.6vincesumergidoNo ratings yet
- Cardio Advances - Hyperaldosteronism in PregnancyDocument11 pagesCardio Advances - Hyperaldosteronism in PregnancyvincesumergidoNo ratings yet
- Treatment Strategies For Osteoarthritis Patients With Pain and HypertensionDocument13 pagesTreatment Strategies For Osteoarthritis Patients With Pain and HypertensionvincesumergidoNo ratings yet
- School Nursing - The Role of Sugar-Sweetened Beverage Consumption in Adolescent Obesity, A Review of The LiteratureDocument11 pagesSchool Nursing - The Role of Sugar-Sweetened Beverage Consumption in Adolescent Obesity, A Review of The LiteraturevincesumergidoNo ratings yet
- Sexuality - The Struggle Over Gay, Lesbian, Bisexual RightsDocument3 pagesSexuality - The Struggle Over Gay, Lesbian, Bisexual RightsvincesumergidoNo ratings yet
- Peripheral Extravasation, Management and PreventionDocument2 pagesPeripheral Extravasation, Management and PreventionvincesumergidoNo ratings yet
- Diabetes - Early-Onset Type 2 Diabetes, Not A Benign ConditionDocument3 pagesDiabetes - Early-Onset Type 2 Diabetes, Not A Benign ConditionvincesumergidoNo ratings yet
- Trauma - Fluids As Oxygen Carriers and The Potential Role in Trauma ResuscitationDocument10 pagesTrauma - Fluids As Oxygen Carriers and The Potential Role in Trauma ResuscitationvincesumergidoNo ratings yet
- School Nursing - Military Children, When Parents Are Deployed OverseasDocument9 pagesSchool Nursing - Military Children, When Parents Are Deployed OverseasvincesumergidoNo ratings yet
- School Nursing - School Nurse Case Management For Children With Chronic Illness, Health, Academic, and Quality of Life OutcomesDocument11 pagesSchool Nursing - School Nurse Case Management For Children With Chronic Illness, Health, Academic, and Quality of Life OutcomesvincesumergidoNo ratings yet
- Trauma - Coagulopathy in Trauma, Optimising Haematological StatusDocument16 pagesTrauma - Coagulopathy in Trauma, Optimising Haematological StatusvincesumergidoNo ratings yet
- Mens Health Adv - Depression, Focus On The Adolescent MaleDocument8 pagesMens Health Adv - Depression, Focus On The Adolescent MalevincesumergidoNo ratings yet
- DEBS Short Courses AY 2012-2013Document1 pageDEBS Short Courses AY 2012-2013vincesumergidoNo ratings yet
- 3 Deadly Trauma ComplicationsDocument7 pages3 Deadly Trauma ComplicationsvincesumergidoNo ratings yet
- Adult ADHD Test 18 Question ADHD-ASRS-v1-1 Adhd-Npf - Com Quality ApprovedDocument3 pagesAdult ADHD Test 18 Question ADHD-ASRS-v1-1 Adhd-Npf - Com Quality ApprovedADHD and ADD100% (14)
- AnemiaDocument1 pageAnemiavincesumergidoNo ratings yet
- Adam Glaser Slides 28 MarchDocument13 pagesAdam Glaser Slides 28 MarchvincesumergidoNo ratings yet
- Pressure Ulcers The Stakes Just Got HigherDocument3 pagesPressure Ulcers The Stakes Just Got HighervincesumergidoNo ratings yet
- A (H1N1)Document3 pagesA (H1N1)vincesumergidoNo ratings yet
- Cardio Advances - Low Sodium Intake Is Associated With Enhanced Vascular Endothelial Function in Mid-Aged & Older Adult With Elev SystolicDocument11 pagesCardio Advances - Low Sodium Intake Is Associated With Enhanced Vascular Endothelial Function in Mid-Aged & Older Adult With Elev SystolicvincesumergidoNo ratings yet
- MyomaDocument8 pagesMyomavincesumergidoNo ratings yet
- SOP NeuroDocument2 pagesSOP NeuroMani100% (2)
- Announcement PIR Kudus 2019Document2 pagesAnnouncement PIR Kudus 2019leiliaNo ratings yet
- Proclamation: Special Observances: National Hospice Month (Proc. 8079)Document2 pagesProclamation: Special Observances: National Hospice Month (Proc. 8079)Justia.comNo ratings yet
- Current Trends in Community NursingDocument9 pagesCurrent Trends in Community Nursingnavasree nimmiNo ratings yet
- Bag TechniqueDocument23 pagesBag TechniqueMamta Rajput83% (12)
- 2007 - Everyday Problem Solvin - Blanchard-Fields PDFDocument6 pages2007 - Everyday Problem Solvin - Blanchard-Fields PDFFlorencia GiulianiNo ratings yet
- Nursing Care Plan: Cues and Data Nursing Diagnosis Analysis Goal and Objectives Interventions Rationale EvaluationDocument3 pagesNursing Care Plan: Cues and Data Nursing Diagnosis Analysis Goal and Objectives Interventions Rationale EvaluationPaul Cubacub100% (1)
- Test Taking Skills and TipsDocument3 pagesTest Taking Skills and TipsabstabsNo ratings yet
- Amanda e Simo ResumeDocument1 pageAmanda e Simo Resumeapi-265680073No ratings yet
- Bidmc GraceDocument55 pagesBidmc GracemelissamattisonNo ratings yet
- 2017 JAMA Review - Delirium in Older Persons Advances in Diagnosis and Treatment PDFDocument14 pages2017 JAMA Review - Delirium in Older Persons Advances in Diagnosis and Treatment PDFgiseladlrNo ratings yet
- Pharma Cog Nos Ti Cal and Phyto-Chemical Evaluation of Vaishvanara Churna - An Ayurvedic FormulationDocument6 pagesPharma Cog Nos Ti Cal and Phyto-Chemical Evaluation of Vaishvanara Churna - An Ayurvedic FormulationijsidonlineinfoNo ratings yet
- Topic 5 DQ 2.Document3 pagesTopic 5 DQ 2.Emmanuel OpiyoNo ratings yet
- Universal Fall Precautions Are CalledDocument5 pagesUniversal Fall Precautions Are CalledsujathaNo ratings yet
- Evidence Based Aquatic Therapy in The ElderlyDocument42 pagesEvidence Based Aquatic Therapy in The ElderlyThermalBathsforActivNo ratings yet
- Essential Consumables & EquipmentDocument9 pagesEssential Consumables & EquipmentOverall Clinical CoordinatorNo ratings yet
- Geriatric Medicine: Dr. B. Goldlist Michael Bloom and Diana Tamir, Chapter Editors Harriette Van Spall, Associate EditorDocument12 pagesGeriatric Medicine: Dr. B. Goldlist Michael Bloom and Diana Tamir, Chapter Editors Harriette Van Spall, Associate EditorLaura Paola UrquizoNo ratings yet
- Brief Evaluation of Executive DysfunctionDocument2 pagesBrief Evaluation of Executive DysfunctionIon Arrieta ValeroNo ratings yet
- Introduction to Gerontological NursingDocument18 pagesIntroduction to Gerontological NursingEvelyn MedinaNo ratings yet
- Progressive Supranuclear Palsy. Kam Newman, Saeed KahkeshaniDocument1 pageProgressive Supranuclear Palsy. Kam Newman, Saeed KahkeshanijingerbrunoNo ratings yet
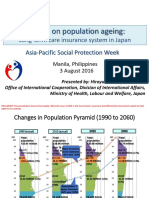
- APSP - Session 9A - Hiroyuki Yamaya - MHLWDocument8 pagesAPSP - Session 9A - Hiroyuki Yamaya - MHLWKristine PresbiteroNo ratings yet
- Geriatric PsychiatryDocument27 pagesGeriatric PsychiatryJosephine IrenaNo ratings yet
- Diabetes Care.: Daftar PustakaDocument3 pagesDiabetes Care.: Daftar PustakaariNo ratings yet
- HistoryDocument18 pagesHistoryshyam ShankarNo ratings yet
- Nursing Diagnosis Fatigue related to Hyper metabolic stateDocument3 pagesNursing Diagnosis Fatigue related to Hyper metabolic stateJohn CenasNo ratings yet
- Geriatric Physiology and The Frailty SyndromeDocument22 pagesGeriatric Physiology and The Frailty SyndromeJoe Polanco100% (1)
- Case Study GeriaDocument12 pagesCase Study GeriaMary Grace Ogatis0% (1)
- New Renalcare CatalogDocument16 pagesNew Renalcare CatalogKaushik Hanskumar ShahNo ratings yet
- Delainy Baker Resume CurrentDocument1 pageDelainy Baker Resume Currentapi-305276868No ratings yet
- Second Year B.SC Nursing Master PlanDocument3 pagesSecond Year B.SC Nursing Master Plancharanjit kaurNo ratings yet