You might also like
- Eclampsia From MedscapeDocument11 pagesEclampsia From Medscapevicky v. p. wardenaar100% (1)
- ECLAMPSIA PresentationDocument16 pagesECLAMPSIA PresentationChristopher SimuntalaNo ratings yet
- Eclampsia: A Life-Threatening Complication of PregnancyDocument8 pagesEclampsia: A Life-Threatening Complication of PregnancyJoan Par GempesNo ratings yet
- EclampsiaDocument24 pagesEclampsiaHengky HanggaraNo ratings yet
- NIHRC Emergency Healthcare ReportDocument144 pagesNIHRC Emergency Healthcare ReportCesar Roberto Braga MacedoNo ratings yet
- Suctioning The Nasopharygeal and Oropharyngeal AirwaysDocument8 pagesSuctioning The Nasopharygeal and Oropharyngeal AirwaysChamelli RobinNo ratings yet
- MANG 502-Modules - Revised - 2009Document68 pagesMANG 502-Modules - Revised - 2009Sef MartinezNo ratings yet
- Pleurisy (Pleuritis): Causes, Symptoms, Tests and TreatmentDocument17 pagesPleurisy (Pleuritis): Causes, Symptoms, Tests and TreatmentkamilahfernandezNo ratings yet
- What Is PeritonitisDocument9 pagesWhat Is PeritonitisArsitoNo ratings yet
- GROUP 3 - CASE STUDY - TraumaDocument5 pagesGROUP 3 - CASE STUDY - TraumaDinarkram Rabreca EculNo ratings yet
- Fundamentals of Nursing RolesDocument15 pagesFundamentals of Nursing RolesDefprimal100% (1)
- Amniotic Fluid EmbolismDocument34 pagesAmniotic Fluid EmbolismReygie MataNo ratings yet
- Pathophysiology of Cervical Cancer-SEE N TREATDocument42 pagesPathophysiology of Cervical Cancer-SEE N TREATEtykaSari100% (1)
- Compare and Contrast Noli & El FiliDocument2 pagesCompare and Contrast Noli & El FiliJosh FuriscalNo ratings yet
- Aortic AneurysmDocument26 pagesAortic Aneurysmchetanm2563100% (1)
- Drug Study Er MedsDocument12 pagesDrug Study Er MedsJerald S. OlaloNo ratings yet
- Acute Respiratory Distress Syndrome (ARDS): Causes, Symptoms and TreatmentDocument30 pagesAcute Respiratory Distress Syndrome (ARDS): Causes, Symptoms and TreatmentOya Zuraini KamalNo ratings yet
- Ischemic Heart Disease Revised LMKDocument50 pagesIschemic Heart Disease Revised LMKLateef KhanNo ratings yet
- Management of SepsisDocument34 pagesManagement of SepsisTamim IshtiaqueNo ratings yet
- Study Questions 3Document12 pagesStudy Questions 3CGNo ratings yet
- Multiple Pregnancy Definition and DiagnosisDocument24 pagesMultiple Pregnancy Definition and DiagnosisNura BamaiyiNo ratings yet
- Emergency Rescue and TransferDocument35 pagesEmergency Rescue and TransferGavinKarl MianabanataoNo ratings yet
- Management of Infective EndocarditisDocument14 pagesManagement of Infective Endocarditismhafzam2020No ratings yet
- Head and Neck ExaminationDocument25 pagesHead and Neck ExaminationDarryl Betts100% (1)
- Systemic HypertensionDocument11 pagesSystemic HypertensionMeldaNo ratings yet
- Reviewer in The Rizl111Document9 pagesReviewer in The Rizl111MarizCaniculaCimanesNo ratings yet
- Cardiovascular AssessmentDocument182 pagesCardiovascular AssessmentAbie Jean BalbontinNo ratings yet
- Myasthenia GravisDocument3 pagesMyasthenia Gravisdmnd_cdNo ratings yet
- Iv Therapy: Presented By: Steven Jones, NREMT-PDocument29 pagesIv Therapy: Presented By: Steven Jones, NREMT-Pbalab2311No ratings yet
- Essential Newborn Care StepsDocument14 pagesEssential Newborn Care StepsTadesse MuhammedNo ratings yet
- Insulin AdministrationDocument15 pagesInsulin Administrationmec17No ratings yet
- RizalDocument10 pagesRizalBennard Cariño FajardoNo ratings yet
- Jade R. Dinolan BSN-4: Diagnosi SDocument5 pagesJade R. Dinolan BSN-4: Diagnosi SJhade Relleta100% (1)
- Coarctation of AortaDocument5 pagesCoarctation of AortaktNo ratings yet
- Diabetes InsipidusDocument39 pagesDiabetes Insipidusกรคุง ภิญโญพจนารถNo ratings yet
- MEDIATRIXDocument67 pagesMEDIATRIXMaria Consuelo LingcasoNo ratings yet
- Umbilical Cord ProlapseDocument6 pagesUmbilical Cord ProlapseCeth BeltranNo ratings yet
- Cardiac ArrythmiasDocument37 pagesCardiac ArrythmiasRubina100% (1)
- What Is TriagingDocument5 pagesWhat Is TriagingshairaNo ratings yet
- Close Right Arm Fracture Nursing CareDocument12 pagesClose Right Arm Fracture Nursing CareBrylle Capili100% (1)
- Altered Urinary Elimination - ADPCN Resource UnitDocument5 pagesAltered Urinary Elimination - ADPCN Resource UnitChillette FarraronsNo ratings yet
- Abruptio Placenta and AbortionDocument10 pagesAbruptio Placenta and Abortiondanica grace gubaNo ratings yet
- Case Report - Perianal AbscessDocument18 pagesCase Report - Perianal AbscessViras VitrianiNo ratings yet
- Donor Bleeding BasicsDocument4 pagesDonor Bleeding BasicsMark Vincent Sahagun100% (1)
- Stages of Fetal DevelopmentDocument42 pagesStages of Fetal DevelopmentKara Ashleigh0% (1)
- Cardiac TamponadeDocument6 pagesCardiac TamponadeJara Maris Moreno BudionganNo ratings yet
- Preeclampsia & EclampsiaDocument24 pagesPreeclampsia & EclampsiaIrfandy Chairi Sulaiman LubisNo ratings yet
- Anatomy and Physiology of The Endocrine SystemDocument41 pagesAnatomy and Physiology of The Endocrine SystemJessica Glitter100% (2)
- Pre-Analytical Consideration in PhlebotomyDocument3 pagesPre-Analytical Consideration in PhlebotomyJacinta Malamion100% (1)
- MedicationDocument32 pagesMedicationسلطان القلحNo ratings yet
- Care of The Mother and The FetusDocument99 pagesCare of The Mother and The FetusBea Bianca CruzNo ratings yet
- Idiopathic Thrombocytopenic Purpura (ITP)Document7 pagesIdiopathic Thrombocytopenic Purpura (ITP)Rizqka PertiwiNo ratings yet
- RAAS System and Drugs That Affect ItDocument22 pagesRAAS System and Drugs That Affect ItChandra pranataNo ratings yet
- Dengue FeverDocument27 pagesDengue FeverHari Mukti100% (4)
- SepsisDocument36 pagesSepsisWan FaizuddinNo ratings yet
- Determining Gravidity and Parity: I. GravidaDocument6 pagesDetermining Gravidity and Parity: I. GravidaDanica CorpuzNo ratings yet
- Life and Works of Rizal Lesson 1Document17 pagesLife and Works of Rizal Lesson 1Miljim UlayNo ratings yet
- Chronic Renal FailureDocument26 pagesChronic Renal FailurePriya GandhiNo ratings yet
- Hypertension PreeclampsiaDocument21 pagesHypertension PreeclampsiaAnis MalakNo ratings yet
- Signs and Symptoms: Pregnancy Tonic-Clonic Seizures Pre-EclampsiaDocument6 pagesSigns and Symptoms: Pregnancy Tonic-Clonic Seizures Pre-Eclampsiafidc_04283646No ratings yet
- Anatomy, Lecture 7, Thorax & Superior Mediastinum (Lecture NOtes)Document13 pagesAnatomy, Lecture 7, Thorax & Superior Mediastinum (Lecture NOtes)Ali Al-QudsiNo ratings yet
- Vetnizah Juniantito's CVDocument3 pagesVetnizah Juniantito's CVjuniantitoNo ratings yet
- Blood Supply of BrainDocument49 pagesBlood Supply of BrainDarling Sevenfoldism SynysterNo ratings yet
- How Your Diet Affects Your BrainDocument2 pagesHow Your Diet Affects Your BrainRusso Dalmasso50% (2)
- Mid Im 2020 AnatomyDocument178 pagesMid Im 2020 AnatomyXzailheene Dela FuenteNo ratings yet
- Local Media5240253493345788412Document2 pagesLocal Media5240253493345788412Miguelito DapieNo ratings yet
- BiobutanolDocument11 pagesBiobutanolPabloDoriaNo ratings yet
- Diffusion & OsmosisDocument16 pagesDiffusion & OsmosisWullant KesumasariiNo ratings yet
- Myocardial Infarction: Myocardial Infarction (MI) or Acute Myocardial Infarction (AMI), Commonly KnownDocument6 pagesMyocardial Infarction: Myocardial Infarction (MI) or Acute Myocardial Infarction (AMI), Commonly KnownLyka Cuanan CorcueraNo ratings yet
- Cat LegendsDocument84 pagesCat LegendsRoxolana KhrouchtchNo ratings yet
- CH 11 AnswersDocument23 pagesCH 11 AnswersJennifer Bash100% (4)
- Snaprevise Biology A2 Revision CheatsheetDocument15 pagesSnaprevise Biology A2 Revision CheatsheetSomaya AliNo ratings yet
- Frazeologie EnglezaDocument11 pagesFrazeologie EnglezaMaria MkNo ratings yet
- Some Answer of Problemset - 7 - KEYDocument3 pagesSome Answer of Problemset - 7 - KEYNihir PatelNo ratings yet
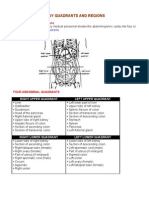
- Organs in The Body Quadrants and RegionsDocument3 pagesOrgans in The Body Quadrants and RegionsDavid HosamNo ratings yet
- The Acute NeurologiDocument343 pagesThe Acute Neurologizee zeeNo ratings yet
- Pharmacology Toxicology - 4th EdDocument41 pagesPharmacology Toxicology - 4th EdYorlenie Juárez100% (1)
- Encyclopedia of Gastroenterology PDFDocument2,352 pagesEncyclopedia of Gastroenterology PDFAndor Claudia Florentina100% (1)
- Adaptasi Biota LautDocument19 pagesAdaptasi Biota LautBudhi Agung Prasetyo100% (1)
- 3 Piece Intrusion Arch - Bhavana ShroffDocument8 pages3 Piece Intrusion Arch - Bhavana ShroffSai Seshadri Bharath ThotaNo ratings yet
- Hubungan Kadar Hemoglobin Dan Tercapainya Remisi Pada Anak Penderita Leukemia AkutDocument7 pagesHubungan Kadar Hemoglobin Dan Tercapainya Remisi Pada Anak Penderita Leukemia AkutRezky RahmadayantiNo ratings yet
- 10th SCERT KeralaDocument72 pages10th SCERT KeralaArun KNo ratings yet
- Plant Nosodes - According To DR John Henry ClarkeDocument29 pagesPlant Nosodes - According To DR John Henry Clarkemelos24No ratings yet
- Organ TransplantationDocument36 pagesOrgan TransplantationAnonymous 4TUSi0SqNo ratings yet
- Veta 3 - Datasheet - ENG - 20210315Document2 pagesVeta 3 - Datasheet - ENG - 20210315JuanNo ratings yet
- Myasthenia GravisDocument3 pagesMyasthenia GravisfsNo ratings yet
- PB - Interpreting An Investigation of Plant Hormones QPDocument6 pagesPB - Interpreting An Investigation of Plant Hormones QPRutba SafdarNo ratings yet
- Reflex Testing Methods For Evaluating C.N.S. Development - Anna's ArchiveDocument78 pagesReflex Testing Methods For Evaluating C.N.S. Development - Anna's ArchiveBrain AngNo ratings yet
- Uro ChordataDocument4 pagesUro ChordataSana SiddiqueNo ratings yet
- How to Build Sexual Anticipation and Satisfy Your Woman All Day LongDocument19 pagesHow to Build Sexual Anticipation and Satisfy Your Woman All Day Longdvladas100% (1)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (4)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (13)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (3)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsNo ratings yet
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (31)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisFrom EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (3)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- Secure Love: Create a Relationship That Lasts a LifetimeFrom EverandSecure Love: Create a Relationship That Lasts a LifetimeRating: 5 out of 5 stars5/5 (17)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (327)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)