You might also like
- PSM Investigation Compliance Checklist Incident Investigation GuidelineDocument1 pagePSM Investigation Compliance Checklist Incident Investigation GuidelineAndy DolmanNo ratings yet
- Incident InvestDocument1 pageIncident InvestAndy DolmanNo ratings yet
- Investigator Name: Event Assessed: Date of Assessment: Checklist For Formal, Written Reports (See Chapter 11)Document1 pageInvestigator Name: Event Assessed: Date of Assessment: Checklist For Formal, Written Reports (See Chapter 11)Andy DolmanNo ratings yet
- Investigator Name: Event Assessed: Date of AssessmentDocument1 pageInvestigator Name: Event Assessed: Date of AssessmentAndy DolmanNo ratings yet
- Checklist For Developing An Incident Investigation PlanDocument1 pageChecklist For Developing An Incident Investigation PlanAndy DolmanNo ratings yet
- Investigator Name: Event Assessed: Date of Assessment: Investigation Follow-Up Checklist Addressed? Follow-Up Issues Yes NoDocument1 pageInvestigator Name: Event Assessed: Date of Assessment: Investigation Follow-Up Checklist Addressed? Follow-Up Issues Yes NoAndy DolmanNo ratings yet
- Sample Investigation Improvement Checklist Incident Investigation GuidelineDocument2 pagesSample Investigation Improvement Checklist Incident Investigation GuidelineAndy DolmanNo ratings yet
- Customize This List For Your Use. See The CCPS Guideline For Investigating Chemical InformationDocument4 pagesCustomize This List For Your Use. See The CCPS Guideline For Investigating Chemical InformationAndy DolmanNo ratings yet
- Incident InvestDocument16 pagesIncident InvestAndy DolmanNo ratings yet
- Investigator Name: Event Assessed: Date of Assessment:: Sample Human Factors Checklist Incident Investigation GuidelineDocument1 pageInvestigator Name: Event Assessed: Date of Assessment:: Sample Human Factors Checklist Incident Investigation GuidelineAndy DolmanNo ratings yet
- Flashback From Waste Gas Incinerator Into Air Supply Piping: Rohm and Haas Texas Inc Deer Park, TX 77536Document8 pagesFlashback From Waste Gas Incinerator Into Air Supply Piping: Rohm and Haas Texas Inc Deer Park, TX 77536Andy DolmanNo ratings yet
- Comprehensive List of CausesDocument1 pageComprehensive List of CausesAndy DolmanNo ratings yet
- Sample Formal Report Outline Incident Investigation GuidelineDocument1 pageSample Formal Report Outline Incident Investigation GuidelineAndy DolmanNo ratings yet
- Investigator Name: Event Assessed: Date of Assessment:: Sample Human Factors Checklist Incident Investigation GuidelineDocument1 pageInvestigator Name: Event Assessed: Date of Assessment:: Sample Human Factors Checklist Incident Investigation GuidelineAndy DolmanNo ratings yet
- Quick Checklist For Investigators: Physical ItemsDocument4 pagesQuick Checklist For Investigators: Physical ItemsAndy DolmanNo ratings yet
- Propane Tank Flare Off in Topeka Cause and Effect Chart: (Simplified Version) 12-2-02Document2 pagesPropane Tank Flare Off in Topeka Cause and Effect Chart: (Simplified Version) 12-2-02Andy DolmanNo ratings yet
- Investigator Name: Event Assessed: Date of AssessmentDocument1 pageInvestigator Name: Event Assessed: Date of AssessmentAndy DolmanNo ratings yet
- Appendix G: Quick Checklist For InvestigatorsDocument5 pagesAppendix G: Quick Checklist For InvestigatorsAndy DolmanNo ratings yet
- Incident InvestDocument1 pageIncident InvestAndy DolmanNo ratings yet
- Appendix B: Professional Assistance DirectoryDocument2 pagesAppendix B: Professional Assistance DirectoryAndy DolmanNo ratings yet
- Appendix F: Selected OSHA and EPA Incident Investigation RegulationsDocument3 pagesAppendix F: Selected OSHA and EPA Incident Investigation RegulationsAndy DolmanNo ratings yet
- Incident InvestDocument5 pagesIncident InvestAndy DolmanNo ratings yet
- Appendix C: Photography Guidelines For Maximum ResultsDocument3 pagesAppendix C: Photography Guidelines For Maximum ResultsAndy DolmanNo ratings yet
- Continuous Improvement For The Incident Investigation SystemDocument10 pagesContinuous Improvement For The Incident Investigation SystemAndy DolmanNo ratings yet
- Incident InvestDocument17 pagesIncident InvestAndy DolmanNo ratings yet
- Appendix A: Relevant OrganizationsDocument3 pagesAppendix A: Relevant OrganizationsAndy DolmanNo ratings yet
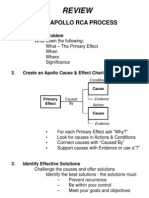
- Review: The Apollo Rca ProcessDocument1 pageReview: The Apollo Rca ProcessAndy DolmanNo ratings yet
- Checklist To Prepare For An Inspection Incident Investigation GuidelineDocument1 pageChecklist To Prepare For An Inspection Incident Investigation GuidelineAndy DolmanNo ratings yet
- Incident InvestDocument17 pagesIncident InvestAndy DolmanNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- GX Developer Ver8 - Operating Manual SH (NA) - 080373-AI (07.13)Document982 pagesGX Developer Ver8 - Operating Manual SH (NA) - 080373-AI (07.13)Filipe LinoNo ratings yet
- Seminar Grade 9 p6 - LATESTDocument44 pagesSeminar Grade 9 p6 - LATESTEdison OrgilNo ratings yet
- Կանխատեսում և պլանավորում 1-4 թեմաներ (1388)Document15 pagesԿանխատեսում և պլանավորում 1-4 թեմաներ (1388)Ashxen HakobyanNo ratings yet
- List of Largest Power Stations in The United StatesDocument14 pagesList of Largest Power Stations in The United Statesoem chhunNo ratings yet
- 1Document96 pages1Ninh Quoc TrungNo ratings yet
- Steam Turbine Working and TypesDocument1 pageSteam Turbine Working and Typesbekaen bekaenNo ratings yet
- Olle I. Elgerd, Patrick D. Van Der Puije (Auth.) - Electric Power Engineering (1998, Springer US) PDFDocument462 pagesOlle I. Elgerd, Patrick D. Van Der Puije (Auth.) - Electric Power Engineering (1998, Springer US) PDFel_ruso__83No ratings yet
- KI Solution Prep 130 MGDocument1 pageKI Solution Prep 130 MGDoreene AndresNo ratings yet
- Discussion Text Nuclear EnergyDocument2 pagesDiscussion Text Nuclear EnergySamuel Adi Santosa100% (1)
- PublicReviewDraft2314 PDFDocument30 pagesPublicReviewDraft2314 PDFJamesNo ratings yet
- Nuclear Security Briefing BookDocument371 pagesNuclear Security Briefing BookAnonymous Mpd6SWH4nENo ratings yet
- (VL) Extended EssayDocument6 pages(VL) Extended Essay민윤지No ratings yet
- Layout and Site SelectionDocument17 pagesLayout and Site Selectionjojo pantherNo ratings yet
- Te 504 WebDocument299 pagesTe 504 WebMaha Ahmed RasimNo ratings yet
- Regulatory Guide 1.138Document25 pagesRegulatory Guide 1.138Pandean Motor Mobil TemanggungNo ratings yet
- Transcript of NPC Uranium Workshop, Baker Lake, June 2007Document246 pagesTranscript of NPC Uranium Workshop, Baker Lake, June 2007NunatsiaqNewsNo ratings yet
- Sagar Mehta (11eebme753) Training Report (Ntps Nashik)Document59 pagesSagar Mehta (11eebme753) Training Report (Ntps Nashik)sagarmehta028No ratings yet
- Atomic Structure (Chemistry O Level)Document50 pagesAtomic Structure (Chemistry O Level)Ping Hui100% (1)
- Failure Rate Standar Data PredictionDocument298 pagesFailure Rate Standar Data Predictionratrihaningds100% (1)
- Power Sys. Analysis PDFDocument40 pagesPower Sys. Analysis PDFIrfan QureshiNo ratings yet
- Introduction To Fission and FusionDocument12 pagesIntroduction To Fission and Fusionkhandey_ramesh@yahoo.co.inNo ratings yet
- Draft National Electricity Plan 9 Sep 2022-2-1Document306 pagesDraft National Electricity Plan 9 Sep 2022-2-1Anonymous Gb3FHXYhNo ratings yet
- Whitcombe CorrespondenceDocument106 pagesWhitcombe CorrespondenceSouthern Alliance for Clean EnergyNo ratings yet
- GE2152 - BASIC CIVIL and MECH - Syllabus With Course OutcomeDocument1 pageGE2152 - BASIC CIVIL and MECH - Syllabus With Course OutcomerkumaravelanNo ratings yet
- Chernobyl Prayer A Chronicle of The Future by Svetlana Alexievich, Anna GuninDocument321 pagesChernobyl Prayer A Chronicle of The Future by Svetlana Alexievich, Anna GuninBooksBaazar KST100% (1)
- S.T.a.L.K.E.R. Savage Worlds ConversionDocument64 pagesS.T.a.L.K.E.R. Savage Worlds ConversionRhys MillerNo ratings yet
- Revised Risk-Informed Inservice Inspection Evaluation ProcedureDocument244 pagesRevised Risk-Informed Inservice Inspection Evaluation ProcedureDanie-ElsNo ratings yet
- Steam Generators Design and SafetyDocument181 pagesSteam Generators Design and Safetyரா. ராஜ பாண்டிNo ratings yet
- Manual AA560 All DiagramsDocument8 pagesManual AA560 All DiagramsmusebladeNo ratings yet