You might also like
- An Overview of Incident Causation TheoriesDocument9 pagesAn Overview of Incident Causation TheoriesAndy DolmanNo ratings yet
- Incident InvestDocument16 pagesIncident InvestAndy DolmanNo ratings yet
- Incident InvestDocument17 pagesIncident InvestAndy DolmanNo ratings yet
- Incident InvestDocument15 pagesIncident InvestAndy DolmanNo ratings yet
- Appendix G: Quick Checklist For InvestigatorsDocument5 pagesAppendix G: Quick Checklist For InvestigatorsAndy DolmanNo ratings yet
- Incident InvestDocument8 pagesIncident InvestAndy DolmanNo ratings yet
- Continuous Improvement For The Incident Investigation SystemDocument10 pagesContinuous Improvement For The Incident Investigation SystemAndy DolmanNo ratings yet
- Investigator Name: Event Assessed: Date of AssessmentDocument1 pageInvestigator Name: Event Assessed: Date of AssessmentAndy DolmanNo ratings yet
- Investigator Name: Event Assessed: Date of Assessment: Investigation Follow-Up Checklist Addressed? Follow-Up Issues Yes NoDocument1 pageInvestigator Name: Event Assessed: Date of Assessment: Investigation Follow-Up Checklist Addressed? Follow-Up Issues Yes NoAndy DolmanNo ratings yet
- Use Case Histories To Energize Your HAZOPDocument6 pagesUse Case Histories To Energize Your HAZOPNanthawat BabybebNo ratings yet
- Ethics Challenger DisasterDocument38 pagesEthics Challenger DisasterHanif MazlanNo ratings yet
- Texas City Refinery Explosion ReportDocument10 pagesTexas City Refinery Explosion ReportNimra JalilNo ratings yet
- Process Safety Management SystemDocument28 pagesProcess Safety Management SystemmalisolangiNo ratings yet
- Application of Fish Bone Diagram To Identify The Root Causes of Any Major Occupational Hazard at Process IndustryDocument12 pagesApplication of Fish Bone Diagram To Identify The Root Causes of Any Major Occupational Hazard at Process IndustryMuneeb BhaniaNo ratings yet
- Ethylene Safety IncidentsDocument88 pagesEthylene Safety IncidentsDavid RodriguesNo ratings yet
- Hazop in HysysDocument8 pagesHazop in HysysSandraNo ratings yet
- Accident Investigation Report - Shell Chemical Company, Deer Park, TexasDocument83 pagesAccident Investigation Report - Shell Chemical Company, Deer Park, TexasAlejandro HernandezNo ratings yet
- Safety Management: University of The East College of EngineeringDocument8 pagesSafety Management: University of The East College of EngineeringAries MalicdemNo ratings yet
- Engineering EthicsDocument12 pagesEngineering Ethicsgopala krishnaNo ratings yet
- Root Causes-Failures That Casuse The Macondo Well ExplosionDocument28 pagesRoot Causes-Failures That Casuse The Macondo Well Explosionnissefar007100% (1)
- Glenn Erwin Written StatementDocument4 pagesGlenn Erwin Written StatementNational Commission on the BP Deepwater Horizon Oil Spill and Offshore DrillingNo ratings yet
- LPB ArticleDocument8 pagesLPB ArticleAndy DolmanNo ratings yet
- Lessons From Longford by Andrew HopkinsDocument21 pagesLessons From Longford by Andrew HopkinssafetysevenNo ratings yet
- TechnicalProgram NewYork PDFDocument118 pagesTechnicalProgram NewYork PDFMohammad WathaifiNo ratings yet
- Example of Chemical Incident Investigation ReportDocument53 pagesExample of Chemical Incident Investigation Reportbaaziz2015No ratings yet
- Unraveling The Cause of An Aircraft Acciden - 2019 - Engineering Failure AnalysiDocument19 pagesUnraveling The Cause of An Aircraft Acciden - 2019 - Engineering Failure AnalysiJimmy the ReverendNo ratings yet
- Dow Learnings and Actions From The Deepwater HorizonDocument10 pagesDow Learnings and Actions From The Deepwater HorizonAbdul AwanNo ratings yet
- Full Assignment 2Document7 pagesFull Assignment 2Klate Biso HohoNo ratings yet
- EPRI Cycle Chemistry Upsets During OperationDocument42 pagesEPRI Cycle Chemistry Upsets During OperationraharjoitbNo ratings yet
- Esso Longford Accident Talk Andrew HopkinsDocument8 pagesEsso Longford Accident Talk Andrew HopkinsP Francis100% (1)
- MT ErebusDocument21 pagesMT ErebusvonmanoNo ratings yet
- Don't Just Pass The Parcel Accidents That Would Not Have Occurred If Those Involved Had Talked TogetherDocument5 pagesDon't Just Pass The Parcel Accidents That Would Not Have Occurred If Those Involved Had Talked Togetherikhan1234No ratings yet
- Arizona State University Tri-University Lab Safety CommitteeDocument8 pagesArizona State University Tri-University Lab Safety Committeesushil@irdNo ratings yet
- Protecting Public Safety Through Excavation Damage PreventionDocument39 pagesProtecting Public Safety Through Excavation Damage PreventionDavid NavarreteNo ratings yet
- Research Paper 2Document5 pagesResearch Paper 2Acads Storage 02No ratings yet
- Summary 1 Analysis of Equipment Failures As Contributors To ChemicalDocument2 pagesSummary 1 Analysis of Equipment Failures As Contributors To ChemicalhafizaltecNo ratings yet
- An Expert System For Car Failure DiagnosisDocument5 pagesAn Expert System For Car Failure DiagnosisSyed Hani AbidiNo ratings yet
- Case Histories Training: ModwlesDocument6 pagesCase Histories Training: ModwlesJavier GiraldoNo ratings yet
- CHPDocument350 pagesCHPSHIVAJI CHOUDHURYNo ratings yet
- EPRI Coal-handling-equipment-Maint-Guide PDFDocument350 pagesEPRI Coal-handling-equipment-Maint-Guide PDFsetia siddiq100% (3)
- AndyDocument17 pagesAndyalim muhamadNo ratings yet
- STS Research PaperDocument19 pagesSTS Research PaperLE AHNo ratings yet
- The Lessons of Valujet 592Document2 pagesThe Lessons of Valujet 592hillerdrewNo ratings yet
- Chemical Plant SafetyDocument7 pagesChemical Plant SafetyCheng Huang100% (1)
- LadkinRCAoverview20130120 PDFDocument19 pagesLadkinRCAoverview20130120 PDFEka KusyantoNo ratings yet
- Process Safety in Chevron PDFDocument40 pagesProcess Safety in Chevron PDFAndika Dimas Prinanda100% (1)
- Yogi Insan PrayogiDocument3 pagesYogi Insan PrayogiYogi InsanNo ratings yet
- Risk Management in The Oil and Gas Industry-LevsonDocument10 pagesRisk Management in The Oil and Gas Industry-LevsonlizuttNo ratings yet
- Aviation Human Factors - Swiss Cheese and Error Chain Model AnalysisDocument18 pagesAviation Human Factors - Swiss Cheese and Error Chain Model AnalysisCharles JenkinsNo ratings yet
- Case Studies in Thermal Engineering: Dayan Li, Guoqing Zhu, Hui Zhu, Zhichao Yu, Yunji Gao, Xiaohui JiangDocument10 pagesCase Studies in Thermal Engineering: Dayan Li, Guoqing Zhu, Hui Zhu, Zhichao Yu, Yunji Gao, Xiaohui JiangArley Salazar HincapieNo ratings yet
- Safety in Chemical Process IndustriesDocument40 pagesSafety in Chemical Process IndustriesDevendra SharmaNo ratings yet
- Compressed Gas CylinderDocument12 pagesCompressed Gas CylinderladaojmNo ratings yet
- Process Hazard Analysis: Faculty of Chemical Engineering Universiti Teknologi MaraDocument30 pagesProcess Hazard Analysis: Faculty of Chemical Engineering Universiti Teknologi MaraSalihin FhooziNo ratings yet
- AGR OptimizationDocument43 pagesAGR Optimizationinara amatullahNo ratings yet
- Carbon Dioxide Total Flooding Fire Extinguishing SystemsDocument97 pagesCarbon Dioxide Total Flooding Fire Extinguishing SystemsKHA120096 StudentNo ratings yet
- Assignment 2Document8 pagesAssignment 2ainul sufiahNo ratings yet
- Osha 3895Document3 pagesOsha 3895Kaycee Lyn Pablo BautistaNo ratings yet
- Importance of Inspection For CorrosionDocument23 pagesImportance of Inspection For CorrosionabyNo ratings yet
- Health Safety and Environment (CDB 1012)Document6 pagesHealth Safety and Environment (CDB 1012)Hamizan FuadNo ratings yet
- PSM Investigation Compliance Checklist Incident Investigation GuidelineDocument1 pagePSM Investigation Compliance Checklist Incident Investigation GuidelineAndy DolmanNo ratings yet
- Investigator Name: Event Assessed: Date of AssessmentDocument1 pageInvestigator Name: Event Assessed: Date of AssessmentAndy DolmanNo ratings yet
- Incident InvestDocument1 pageIncident InvestAndy DolmanNo ratings yet
- Sample Investigation Improvement Checklist Incident Investigation GuidelineDocument2 pagesSample Investigation Improvement Checklist Incident Investigation GuidelineAndy DolmanNo ratings yet
- Investigator Name: Event Assessed: Date of Assessment: Investigation Follow-Up Checklist Addressed? Follow-Up Issues Yes NoDocument1 pageInvestigator Name: Event Assessed: Date of Assessment: Investigation Follow-Up Checklist Addressed? Follow-Up Issues Yes NoAndy DolmanNo ratings yet
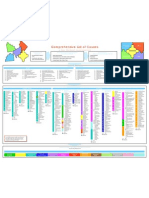
- Comprehensive List of CausesDocument1 pageComprehensive List of CausesAndy DolmanNo ratings yet
- Investigator Name: Event Assessed: Date of Assessment:: Sample Human Factors Checklist Incident Investigation GuidelineDocument1 pageInvestigator Name: Event Assessed: Date of Assessment:: Sample Human Factors Checklist Incident Investigation GuidelineAndy DolmanNo ratings yet
- Customize This List For Your Use. See The CCPS Guideline For Investigating Chemical InformationDocument4 pagesCustomize This List For Your Use. See The CCPS Guideline For Investigating Chemical InformationAndy DolmanNo ratings yet
- Quick Checklist For Investigators: Physical ItemsDocument4 pagesQuick Checklist For Investigators: Physical ItemsAndy DolmanNo ratings yet
- Checklist For Developing An Incident Investigation PlanDocument1 pageChecklist For Developing An Incident Investigation PlanAndy DolmanNo ratings yet
- Flashback From Waste Gas Incinerator Into Air Supply Piping: Rohm and Haas Texas Inc Deer Park, TX 77536Document8 pagesFlashback From Waste Gas Incinerator Into Air Supply Piping: Rohm and Haas Texas Inc Deer Park, TX 77536Andy DolmanNo ratings yet
- Propane Tank Flare Off in Topeka Cause and Effect Chart: (Simplified Version) 12-2-02Document2 pagesPropane Tank Flare Off in Topeka Cause and Effect Chart: (Simplified Version) 12-2-02Andy DolmanNo ratings yet
- Appendix B: Professional Assistance DirectoryDocument2 pagesAppendix B: Professional Assistance DirectoryAndy DolmanNo ratings yet
- Incident InvestDocument1 pageIncident InvestAndy DolmanNo ratings yet
- Investigator Name: Event Assessed: Date of AssessmentDocument1 pageInvestigator Name: Event Assessed: Date of AssessmentAndy DolmanNo ratings yet
- Appendix C: Photography Guidelines For Maximum ResultsDocument3 pagesAppendix C: Photography Guidelines For Maximum ResultsAndy DolmanNo ratings yet
- Appendix F: Selected OSHA and EPA Incident Investigation RegulationsDocument3 pagesAppendix F: Selected OSHA and EPA Incident Investigation RegulationsAndy DolmanNo ratings yet
- Appendix A: Relevant OrganizationsDocument3 pagesAppendix A: Relevant OrganizationsAndy DolmanNo ratings yet
- Review: The Apollo Rca ProcessDocument1 pageReview: The Apollo Rca ProcessAndy DolmanNo ratings yet
- Checklist To Prepare For An Inspection Incident Investigation GuidelineDocument1 pageChecklist To Prepare For An Inspection Incident Investigation GuidelineAndy DolmanNo ratings yet
- Continuous Improvement For The Incident Investigation SystemDocument10 pagesContinuous Improvement For The Incident Investigation SystemAndy DolmanNo ratings yet
- Plant Tech GuideDocument5 pagesPlant Tech GuideAndy DolmanNo ratings yet
- Critical Process Impact MatrixDocument1 pageCritical Process Impact MatrixAndy DolmanNo ratings yet
- Incident InvestDocument8 pagesIncident InvestAndy DolmanNo ratings yet
- 2018 Daubert Cromwell CatalogDocument12 pages2018 Daubert Cromwell CatalogRavindra ErabattiNo ratings yet
- Pipe ManufactureDocument26 pagesPipe ManufactureFazlul Karim AkashNo ratings yet
- NalcoDocument38 pagesNalcomohamadNo ratings yet
- ASTM B912 Passivation of Stainless Steels Using ElectropolishingDocument4 pagesASTM B912 Passivation of Stainless Steels Using ElectropolishingHeri VillaNo ratings yet
- Eval 3 Understanding, Observe & POV-digabungkanDocument78 pagesEval 3 Understanding, Observe & POV-digabungkanValentine Vallery HaryantoNo ratings yet
- IRITS0815141 0717 MR150 Man Rider WinchscreenDocument8 pagesIRITS0815141 0717 MR150 Man Rider WinchscreenPopovici AlexandruNo ratings yet
- 4W2007 Final ReportDocument294 pages4W2007 Final ReportmdchetrNo ratings yet
- CBSE NET Environmental Science Paper 2 June 2015Document8 pagesCBSE NET Environmental Science Paper 2 June 2015AlokfriNo ratings yet
- HAC-10143-MS-CIV-003-Method Statement For Concrete RepairDocument26 pagesHAC-10143-MS-CIV-003-Method Statement For Concrete RepairHema playsNo ratings yet
- Din 17744Document5 pagesDin 17744NastyNo ratings yet
- Closed & Open API 570 ExamDocument22 pagesClosed & Open API 570 ExammazpriNo ratings yet
- CANIN ManualDocument58 pagesCANIN ManualJohn MartinosNo ratings yet
- Water Treatment For Cooling TowersDocument8 pagesWater Treatment For Cooling TowersSrinivasan RaviNo ratings yet
- Wrapid Sleeve PDSDocument2 pagesWrapid Sleeve PDSjayhuacat7743No ratings yet
- Industriereiniger EngDocument6 pagesIndustriereiniger EngKiran DuggarajuNo ratings yet
- Astm B545Document8 pagesAstm B545MarcoAntonio100% (1)
- Thermally Sprayed Coatings Resistant To Erosion and Corrosion For Power Plant Boilers - A ReviewDocument12 pagesThermally Sprayed Coatings Resistant To Erosion and Corrosion For Power Plant Boilers - A ReviewLuis Duchesne GonzálezNo ratings yet
- Nickel Aluminium Bronze: A Reconsideration For Valve ManufactureDocument4 pagesNickel Aluminium Bronze: A Reconsideration For Valve ManufactureFred Duarte CaldeiraNo ratings yet
- Passenger Coach Design - Ease of Maintenance & Examination and Design ToolsDocument129 pagesPassenger Coach Design - Ease of Maintenance & Examination and Design Toolsravi_entertainfoNo ratings yet
- Tips For Repairing and Upgrading PumpDocument8 pagesTips For Repairing and Upgrading PumpBlack PearlNo ratings yet
- Architectural Specs PDFDocument391 pagesArchitectural Specs PDFUri BabaNo ratings yet
- Features: 40 - 600mm ASME Class 150Document5 pagesFeatures: 40 - 600mm ASME Class 150Capacitacion TodocatNo ratings yet
- Assessment of Air Preheater Effects On Power Plant EfficiencyDocument38 pagesAssessment of Air Preheater Effects On Power Plant Efficiencysugianto barusNo ratings yet
- Tutorial 3 PDFDocument9 pagesTutorial 3 PDFMurad AlamNo ratings yet
- To Foul or Not To FoulDocument8 pagesTo Foul or Not To FoulkcdeguzmanNo ratings yet
- STP1298 Eb.1415051 1 PDFDocument304 pagesSTP1298 Eb.1415051 1 PDFpaola100% (1)
- Astm A618-99Document4 pagesAstm A618-99Mohamed FaroukNo ratings yet
- Painting of Naval Ornance Equipment 1955Document17 pagesPainting of Naval Ornance Equipment 1955jinxx10No ratings yet
- Corrosion Prevention For MetalsDocument17 pagesCorrosion Prevention For Metalsabdul100% (1)
- Ac Corroosion PHD ThesisDocument168 pagesAc Corroosion PHD ThesisMn Hjhjj100% (1)