You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Jps R 06101406Document4 pagesJps R 06101406Afiqah RahahNo ratings yet
- Pedia Allergic DisordersDocument4 pagesPedia Allergic Disordersmia liaNo ratings yet
- Food AllergyDocument6 pagesFood AllergyMegaWulandariNo ratings yet
- Homeopathy remedies for different types of allergyDocument4 pagesHomeopathy remedies for different types of allergyMahmood MuftiNo ratings yet
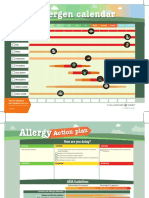
- Allergen Calendar - EnglishDocument2 pagesAllergen Calendar - Englishpkgill15No ratings yet
- SDS Erapol E83A ISS141003 EnglishDocument7 pagesSDS Erapol E83A ISS141003 EnglishLucas NievaNo ratings yet
- DR Ediyono SP P Sub Dep Paru RSAL DR Ramelan: Farmasi UBY S2 April 2016Document132 pagesDR Ediyono SP P Sub Dep Paru RSAL DR Ramelan: Farmasi UBY S2 April 2016Sukmawati Eka Bima SahputriNo ratings yet
- The Allergy Book 1st Edition 2015 PDFDocument211 pagesThe Allergy Book 1st Edition 2015 PDFtuilaai100% (1)
- Allergen Immunotherapy Extract Preparation GuideDocument44 pagesAllergen Immunotherapy Extract Preparation Guidesara-1234No ratings yet
- Healing Hacker Q&A With DR Xiu-Min LiDocument10 pagesHealing Hacker Q&A With DR Xiu-Min LiRuth LinNo ratings yet
- Chronic Actinic DermatitisDocument5 pagesChronic Actinic DermatitisdarshinidaveNo ratings yet
- Pharmacognosy Book of Pharmacy TechnicianDocument138 pagesPharmacognosy Book of Pharmacy TechnicianSabeen MustafaNo ratings yet
- 3gallergy 2020 - Specific - IgE - Universal - Kit - IMMULITE - 2000 - Systems - Rev - 32 - DXDCM - 09017fe9804a6eb0-1598648757334Document49 pages3gallergy 2020 - Specific - IgE - Universal - Kit - IMMULITE - 2000 - Systems - Rev - 32 - DXDCM - 09017fe9804a6eb0-1598648757334Pierre LavoisierNo ratings yet
- Legumes and Oilseeds Bahan #4-5 PDFDocument57 pagesLegumes and Oilseeds Bahan #4-5 PDFAde Kurnia Febriansyah100% (1)
- Childhood Asthma Etiology and EpidemiologyDocument24 pagesChildhood Asthma Etiology and EpidemiologyEstella100% (1)
- Pathophysiology Exam QuestionsDocument11 pagesPathophysiology Exam Questionsjimmy100% (2)
- Contact Dermatitis: A Practice ParameterDocument38 pagesContact Dermatitis: A Practice ParameterdhirazhrNo ratings yet
- Surgery For Allergic Rhinitis Chhabra2014Document5 pagesSurgery For Allergic Rhinitis Chhabra2014Gaby ToledoNo ratings yet
- Educational Program To Prevent Foodborne Diseases at Restaurants of Suez Canal UniversityDocument138 pagesEducational Program To Prevent Foodborne Diseases at Restaurants of Suez Canal UniversityAmalElnawasanyNo ratings yet
- Anaphylaxis TalkDocument60 pagesAnaphylaxis TalkAqib NabiNo ratings yet
- United States District Court Middle District of Florida Orlando DivisionDocument12 pagesUnited States District Court Middle District of Florida Orlando DivisionJ Rohrlich100% (1)
- Prevalens of Tree Nut AllergyDocument13 pagesPrevalens of Tree Nut AllergyponbohacopNo ratings yet
- Biotechnology 101Document273 pagesBiotechnology 101Mitasha Bharadwaj AroraNo ratings yet
- Allergy Skin TestsDocument6 pagesAllergy Skin TestsAnindya Putri KusumajatiNo ratings yet
- Review Garlic (Allium Sativum L.) : Adverse Effects and Drug Interactions in HumansDocument12 pagesReview Garlic (Allium Sativum L.) : Adverse Effects and Drug Interactions in HumansRizkaa Harinii QuinshaNo ratings yet
- Book-Based Pathophysiology of Allergic and Non-Allergic RhinitisDocument2 pagesBook-Based Pathophysiology of Allergic and Non-Allergic RhinitisJeraldine Corpuz PascualNo ratings yet
- 66 Allery and OrthodonticDocument5 pages66 Allery and OrthodonticShruthi KamarajNo ratings yet
- Prevalence and Diagnosis of Food Allergy in Children (Sri LankaDocument5 pagesPrevalence and Diagnosis of Food Allergy in Children (Sri LankaPutri Alif PermatasariNo ratings yet
- Allergic Rhinitis Diagnosis TreatmentDocument2 pagesAllergic Rhinitis Diagnosis TreatmentDengz MendozaNo ratings yet
- Tata Laksana Rinitis Alergi Pada Dewasa FINALDocument27 pagesTata Laksana Rinitis Alergi Pada Dewasa FINALNikko Khairul DafaNo ratings yet