You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Group Imago and The Stages of Group DevelopmentDocument16 pagesGroup Imago and The Stages of Group DevelopmentNarcis Nagy100% (3)
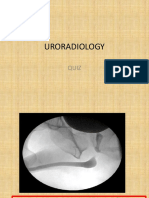
- Uroradiology Quiz 1Document2 pagesUroradiology Quiz 1chimbimbNo ratings yet
- Serrapeptase - The Miracle Enzyme Which Can Save Your LifeDocument53 pagesSerrapeptase - The Miracle Enzyme Which Can Save Your LifeRoger-Peter Weizenegger100% (7)
- Part A. Reading Comprehension: Attitude Therapy Misleading Recognize Refuse EstablishmentDocument2 pagesPart A. Reading Comprehension: Attitude Therapy Misleading Recognize Refuse EstablishmentCarol80% (5)
- Pathophysiology of Urinary ObstructionDocument32 pagesPathophysiology of Urinary ObstructionchimbimbNo ratings yet
- 20 UrolithiasisDocument38 pages20 UrolithiasisHelda W HadiNo ratings yet
- Ams 12 27581Document11 pagesAms 12 27581fkNo ratings yet
- Penile CancerDocument22 pagesPenile CancerchimbimbNo ratings yet
- A Practical Approach To IntersexDocument15 pagesA Practical Approach To IntersexchimbimbNo ratings yet
- Penile CancerDocument22 pagesPenile CancerchimbimbNo ratings yet
- Penile CancerDocument22 pagesPenile CancerchimbimbNo ratings yet
- Surgery For Wilms TumourDocument7 pagesSurgery For Wilms TumourchimbimbNo ratings yet
- Chapter 4 Wilms Tumor and Its Management in A Surgical AspectDocument10 pagesChapter 4 Wilms Tumor and Its Management in A Surgical AspectchimbimbNo ratings yet
- Disorder of Sexual DifferentiationDocument8 pagesDisorder of Sexual DifferentiationchimbimbNo ratings yet
- ABCs of Medical Management of Stones PDFDocument22 pagesABCs of Medical Management of Stones PDFchimbimbNo ratings yet
- Acid-Base Balance 2Document62 pagesAcid-Base Balance 2chimbimbNo ratings yet
- WHO MC - Manual - 2018 PDFDocument403 pagesWHO MC - Manual - 2018 PDFchimbimbNo ratings yet
- Prostate Cancer 5th YearDocument35 pagesProstate Cancer 5th YearchimbimbNo ratings yet
- Urology X Rays For 5thyearDocument36 pagesUrology X Rays For 5thyearchimbimbNo ratings yet
- Urinary Lithiasis: DR Mukosai Urological SurgeonDocument25 pagesUrinary Lithiasis: DR Mukosai Urological SurgeonchimbimbNo ratings yet
- 7th Year Urinary Stone QuestionsDocument3 pages7th Year Urinary Stone QuestionschimbimbNo ratings yet
- Benign Prostatic Hyperplasia (BPH)Document22 pagesBenign Prostatic Hyperplasia (BPH)chimbimbNo ratings yet
- Benign Prostatic Hyperplasia (BPH)Document22 pagesBenign Prostatic Hyperplasia (BPH)chimbimbNo ratings yet
- Bladder Stone Case ReportDocument5 pagesBladder Stone Case ReportchimbimbNo ratings yet
- Secondary Hormone Therapy For CRPCDocument4 pagesSecondary Hormone Therapy For CRPCchimbimbNo ratings yet
- ABC of BurnsDocument37 pagesABC of Burnsiraklisd100% (2)
- Asymptomatic Microhematuria PDFDocument1 pageAsymptomatic Microhematuria PDFchimbimbNo ratings yet
- OAB GuidelineDocument36 pagesOAB GuidelinechimbimbNo ratings yet
- Penile Cancer Case Series ReportDocument7 pagesPenile Cancer Case Series ReportchimbimbNo ratings yet
- Imaging For Urethral CalculusDocument19 pagesImaging For Urethral Calculuschimbimb100% (1)
- Ultrasound Exam in The Practice of UrologyDocument12 pagesUltrasound Exam in The Practice of UrologychimbimbNo ratings yet
- The Management of Bladder Cancer Diagnosis and TreatmentDocument51 pagesThe Management of Bladder Cancer Diagnosis and TreatmentchimbimbNo ratings yet
- BCG in CaBladder PDFDocument7 pagesBCG in CaBladder PDFchimbimbNo ratings yet
- Stugeron ForteDocument4 pagesStugeron ForteJemsMei Comparativo MensuradoNo ratings yet
- Philhealth Cf4 2017-2018Document8 pagesPhilhealth Cf4 2017-2018Julius Yves Dulfo BagacayNo ratings yet
- Enraf-Nonius Manumed Exercise enDocument6 pagesEnraf-Nonius Manumed Exercise enjoseprudencio8848No ratings yet
- Foods That Kill CandidaDocument3 pagesFoods That Kill Candidasexy_rusian100% (1)
- Peripheral Vascular DiseaseDocument53 pagesPeripheral Vascular DiseaseShenbagam Mahalingam100% (1)
- Counseling PhilosophyDocument7 pagesCounseling Philosophyapi-403911586No ratings yet
- Boils and Carbuncles: (Mayo Clinic)Document15 pagesBoils and Carbuncles: (Mayo Clinic)Jimmy ThomasNo ratings yet
- Nursing Process of A Client With CholelithiasisDocument21 pagesNursing Process of A Client With Cholelithiasisapi-3822508100% (6)
- Heavy HandsDocument8 pagesHeavy HandsPicklehead McSpazatronNo ratings yet
- NCP 1Document4 pagesNCP 1Ke EjieNo ratings yet
- Dexmedetomidine Vs Propofol - RCT - Merry Andriany 406162043Document7 pagesDexmedetomidine Vs Propofol - RCT - Merry Andriany 406162043Merry AndrianyNo ratings yet
- Daftar Harga PT Bernofarm (RS Medirossa)Document3 pagesDaftar Harga PT Bernofarm (RS Medirossa)Syaofi SofiNo ratings yet
- MSDS - SiliconeFluid200 350Document7 pagesMSDS - SiliconeFluid200 350Rafael Saldanha LopesNo ratings yet
- Pyogenic MeningitisDocument20 pagesPyogenic MeningitisClever BarbieNo ratings yet
- Waste Management ProcedureDocument3 pagesWaste Management ProcedureBoby ThomasNo ratings yet
- European Waste Catalogue AND Hazardous Waste List: Valid From 1 January 2002Document49 pagesEuropean Waste Catalogue AND Hazardous Waste List: Valid From 1 January 2002Mark VellaNo ratings yet
- Smart Syringe Pumps For Drug Infusion During DentalDocument9 pagesSmart Syringe Pumps For Drug Infusion During DentalAshit GandhiNo ratings yet
- Preop ProofsDocument14 pagesPreop ProofsJanhvi AswaniNo ratings yet
- Drug StudyDocument3 pagesDrug StudyKheem MoralesNo ratings yet
- Sports PhysicalDocument4 pagesSports Physicalapi-209628543No ratings yet
- Night FeverDocument5 pagesNight FeverdewioktaNo ratings yet
- Osu Vegetable Seed TreatmentDocument5 pagesOsu Vegetable Seed TreatmentGman007No ratings yet
- BSHM 55 - Lesson 9 & 10Document9 pagesBSHM 55 - Lesson 9 & 10Yisu HimaaNo ratings yet
- Hernia+scrotal MassDocument82 pagesHernia+scrotal MassJJ JirapathNo ratings yet
- Greys - anatomy.S02E25. 17 Seconds - SRTDocument55 pagesGreys - anatomy.S02E25. 17 Seconds - SRTYing Xuan EngNo ratings yet
- Cancer ReishiDocument15 pagesCancer Reishijunver100% (1)
- Wikipedia - Couvelaire Uterus - Wikipedia, The Free EncyclopediaDocument2 pagesWikipedia - Couvelaire Uterus - Wikipedia, The Free EncyclopediaPabloGBNo ratings yet