You might also like
- Drug StudyDocument10 pagesDrug StudyRye IbarraNo ratings yet
- Drug StudyDocument8 pagesDrug Studysarah1217No ratings yet
- Complete Drugs StudyDocument13 pagesComplete Drugs StudyPeace Andong PerochoNo ratings yet
- Paracetamol and Levofloxacin Drug StudyDocument9 pagesParacetamol and Levofloxacin Drug StudyKevin Sam AguirreNo ratings yet
- ADALIMUMAB (Humira)Document4 pagesADALIMUMAB (Humira)GLen CaniedoNo ratings yet
- Drug StudyDocument11 pagesDrug StudyKaloy KamaoNo ratings yet
- Drug Analysis: Submitted By: GALICINAO, Gretta Shalou GDocument9 pagesDrug Analysis: Submitted By: GALICINAO, Gretta Shalou GggalicinaoNo ratings yet
- Drug StudyDocument7 pagesDrug StudysarahtotNo ratings yet
- Drug Study 68-75Document8 pagesDrug Study 68-75joshua_santiago_5No ratings yet
- Drug StudyDocument6 pagesDrug StudyNajmah Saaban100% (1)
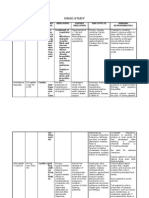
- Drug Name Action Indication Contraindication Adverse Effects Nursing ResponsibilitiesDocument5 pagesDrug Name Action Indication Contraindication Adverse Effects Nursing ResponsibilitiesJanry-Mae Escobar TumanengNo ratings yet
- Methotrexate Guide for Rheumatoid Arthritis & CancerDocument5 pagesMethotrexate Guide for Rheumatoid Arthritis & CancerDea Sabelle CastroNo ratings yet
- Drug Study 408Document13 pagesDrug Study 408Jheryck SabadaoNo ratings yet
- Drug Study GabrielaDocument4 pagesDrug Study GabrielaNimrodNo ratings yet
- Drug Study Clindamycin, Ipatropium BromideDocument8 pagesDrug Study Clindamycin, Ipatropium Bromidepaupaulala100% (2)
- Respiratory Medications ReviewDocument4 pagesRespiratory Medications ReviewKevin VillaranteNo ratings yet
- Calcium Carbonate for Bone HealthDocument14 pagesCalcium Carbonate for Bone HealthBianca Freya Porral85% (13)
- Drug Action Indication Adverse Effects Contraindications Nursing Considerations Ketorolac TromethamineDocument8 pagesDrug Action Indication Adverse Effects Contraindications Nursing Considerations Ketorolac TromethamineAiryn CanonNo ratings yet
- Name of Drug Route/Dose Mechanism of Action Indication Side Effects/Adverse Reactions Nursing ResponsibilitiesDocument9 pagesName of Drug Route/Dose Mechanism of Action Indication Side Effects/Adverse Reactions Nursing ResponsibilitiespauchanmnlNo ratings yet
- Drug StudyDocument6 pagesDrug StudyFloramae Celine BosqueNo ratings yet
- Nicardipine (: ClassificationDocument14 pagesNicardipine (: ClassificationWilliam CiferNo ratings yet
- Metformin Hydrochloride PDFDocument4 pagesMetformin Hydrochloride PDFHannaNo ratings yet
- MOXIFLOXACIN MonographDocument3 pagesMOXIFLOXACIN Monographfayrouz fathiNo ratings yet
- Drug 25Document17 pagesDrug 25carol_gigliotti24100% (1)
- Drug StudyDocument8 pagesDrug StudyAysaaa DCNo ratings yet
- Ventolin Nebulizer for Bronchospasm ReliefDocument10 pagesVentolin Nebulizer for Bronchospasm ReliefmidskiescreamzNo ratings yet
- Drug StudyDocument3 pagesDrug Studyanon_11638632No ratings yet
- Drug StudyDocument10 pagesDrug StudyFranco ObedozaNo ratings yet
- Anti-inflammatory corticosteroid hydrocortisone generic and brand names, dosage, classification, actions, indications, contraindications and side effectsDocument6 pagesAnti-inflammatory corticosteroid hydrocortisone generic and brand names, dosage, classification, actions, indications, contraindications and side effectstrinaLCNo ratings yet
- Drug Cefaclor IsoxsuprineDocument6 pagesDrug Cefaclor IsoxsuprineJelly Ong 王金玉No ratings yet
- Drug Study: Acetylcysteine, Amlodipine, Atorvastatin, Clonidine & MoreDocument12 pagesDrug Study: Acetylcysteine, Amlodipine, Atorvastatin, Clonidine & MoreMarvin V ParahinogNo ratings yet
- Drug Study QiDocument6 pagesDrug Study QiKevin Sam AguirreNo ratings yet
- Drug Study HydralazineDocument10 pagesDrug Study HydralazineLuige AvilaNo ratings yet
- Drug Study Cap RHPDocument7 pagesDrug Study Cap RHPJan DeeNo ratings yet
- Drug Study for Hepatic Abscess PatientDocument3 pagesDrug Study for Hepatic Abscess PatientEric EvangelistaNo ratings yet
- Drug StudyDocument7 pagesDrug StudyDiana Laura LeiNo ratings yet
- Chew, swallow or crush mebendazole tabletsDocument6 pagesChew, swallow or crush mebendazole tabletsDenvicNo ratings yet
- MEDICATION: Garamycin, Garamycin Ophthalmic, Genoptic Classifications: Antiinfective Aminoglycoside Antibiotic ActionDocument4 pagesMEDICATION: Garamycin, Garamycin Ophthalmic, Genoptic Classifications: Antiinfective Aminoglycoside Antibiotic ActionLea Mae HandayanNo ratings yet
- Drug StudyDocument5 pagesDrug StudyCrystal Joy MisaNo ratings yet
- LIVOLIN FORTE ACTIONS AND USESDocument5 pagesLIVOLIN FORTE ACTIONS AND USESDick Morgan FerrerNo ratings yet
- Drug Study CompilationDocument9 pagesDrug Study CompilationRene John FranciscoNo ratings yet
- TB medications overviewDocument7 pagesTB medications overviewANNIE SHINE MAGSACAYNo ratings yet
- Paracetamol Antipyretic and Analgesic GuideDocument7 pagesParacetamol Antipyretic and Analgesic GuideAnne Monique Moran OngjocoNo ratings yet
- Drug RationaleDocument77 pagesDrug RationaleYolanda WilliamsNo ratings yet
- Drug StudyDocument11 pagesDrug StudyNedemar OcampoNo ratings yet
- Drug StudyDocument9 pagesDrug StudyOdarp PradzNo ratings yet
- Drug Study - CaseDocument9 pagesDrug Study - CaseMay EvelynNo ratings yet
- Amikacin antibiotic for urinary tract infectionsDocument17 pagesAmikacin antibiotic for urinary tract infectionsMc Crister SilangNo ratings yet
- Name of DrugDocument17 pagesName of DrugAllan DiazNo ratings yet
- Drug StuyJJASGHDocument7 pagesDrug StuyJJASGHJan Pierre RodriguezNo ratings yet
- Fluorouracil Drug StudyDocument8 pagesFluorouracil Drug StudyAlexandrea MayNo ratings yet
- FLUOROURACIL Drug StudyDocument8 pagesFLUOROURACIL Drug StudyAlexandrea MayNo ratings yet
- ETHAMBUTOLDocument2 pagesETHAMBUTOLXerxes DejitoNo ratings yet
- Legaspi Course Task 2Document7 pagesLegaspi Course Task 2FATIMA AIRA LEGASPINo ratings yet
- 8copd DrugtabncpDocument18 pages8copd DrugtabncpMaristelaMolinaNo ratings yet
- Lisinopril PDFDocument3 pagesLisinopril PDFHannaNo ratings yet
- Adult: PO HTN Initial: 50-100 Mg/day in Single or Divided Doses Increase SlowlyDocument3 pagesAdult: PO HTN Initial: 50-100 Mg/day in Single or Divided Doses Increase SlowlyJoanna Marie Lumbre BalbiranNo ratings yet
- Naplex Complete Study Outline A Topic-Wise Approach DiabetesFrom EverandNaplex Complete Study Outline A Topic-Wise Approach DiabetesRating: 4 out of 5 stars4/5 (2)
- JoyDocument1 pageJoyLyn ConsingNo ratings yet
- NLE ReviewerDocument246 pagesNLE Reviewerblazegomez99% (69)
- NURSING RESEARCH Nursing Research - Kerlinger - The Systematic, EmpiricalDocument32 pagesNURSING RESEARCH Nursing Research - Kerlinger - The Systematic, Empiricalrizaustria100% (3)
- Drugs For Liver CirrhosisDocument7 pagesDrugs For Liver CirrhosisLyn ConsingNo ratings yet
- Psych NursingDocument28 pagesPsych NursingLyn ConsingNo ratings yet
- MenstruationDocument25 pagesMenstruationLyn ConsingNo ratings yet
- Communicable Dse ReviewerDocument13 pagesCommunicable Dse ReviewerRichard Ines Valino100% (29)
- Maternity Nursing Edited Royal PentagonDocument49 pagesMaternity Nursing Edited Royal PentagonRichard Ines Valino95% (38)
- Psych NursingDocument28 pagesPsych NursingLyn ConsingNo ratings yet
- Maternity NursingDocument23 pagesMaternity NursingLyn ConsingNo ratings yet
- Medicare Proposes Small Payment Increases for Outpatient Departments, ASCsDocument2 pagesMedicare Proposes Small Payment Increases for Outpatient Departments, ASCsLyn ConsingNo ratings yet
- Certificate of AttendanceDocument1 pageCertificate of AttendanceLyn ConsingNo ratings yet
- Case Study FormatDocument2 pagesCase Study Formatalieze11100% (1)
- Salbutamol Drug Study Generic Name: Brand NameDocument4 pagesSalbutamol Drug Study Generic Name: Brand NameLyn ConsingNo ratings yet
- Formal Place SettingDocument8 pagesFormal Place SettingLyn Consing100% (1)
- Anti TuberculosisagentsDocument24 pagesAnti TuberculosisagentsLyn ConsingNo ratings yet
- Anti TuberculosisagentsDocument24 pagesAnti TuberculosisagentsLyn ConsingNo ratings yet
- URLDocument21 pagesURLLyn Consing100% (3)
- Seven principles of good practice in health educationDocument7 pagesSeven principles of good practice in health educationLyn ConsingNo ratings yet
- URL and HTMLDocument4 pagesURL and HTMLLyn ConsingNo ratings yet
- EquipmentsDocument1 pageEquipmentsLyn ConsingNo ratings yet
- EquipmentsDocument1 pageEquipmentsLyn ConsingNo ratings yet
- Individual Performance Commitment and Review Form (Ipcrf) : Mfos Kras Objectives Timeline Weight Per KRADocument4 pagesIndividual Performance Commitment and Review Form (Ipcrf) : Mfos Kras Objectives Timeline Weight Per KRAChris21JinkyNo ratings yet
- Legends and Lairs - Elemental Lore PDFDocument66 pagesLegends and Lairs - Elemental Lore PDFAlexis LoboNo ratings yet
- Indian Standard: Pla Ing and Design of Drainage IN Irrigation Projects - GuidelinesDocument7 pagesIndian Standard: Pla Ing and Design of Drainage IN Irrigation Projects - GuidelinesGolak PattanaikNo ratings yet
- Peran Dan Tugas Receptionist Pada Pt. Serim Indonesia: Disadur Oleh: Dra. Nani Nuraini Sarah MsiDocument19 pagesPeran Dan Tugas Receptionist Pada Pt. Serim Indonesia: Disadur Oleh: Dra. Nani Nuraini Sarah MsiCynthia HtbNo ratings yet
- TJUSAMO 2013-2014 Modular ArithmeticDocument4 pagesTJUSAMO 2013-2014 Modular ArithmeticChanthana ChongchareonNo ratings yet
- Dep 32.32.00.11-Custody Transfer Measurement Systems For LiquidDocument69 pagesDep 32.32.00.11-Custody Transfer Measurement Systems For LiquidDAYONo ratings yet
- Oxygen Cost and Energy Expenditure of RunningDocument7 pagesOxygen Cost and Energy Expenditure of Runningnb22714No ratings yet
- SBI Sample PaperDocument283 pagesSBI Sample Paperbeintouch1430% (1)
- SNC 2p1 Course Overview 2015Document2 pagesSNC 2p1 Course Overview 2015api-212901753No ratings yet
- Special Power of Attorney: Benedict Joseph M. CruzDocument1 pageSpecial Power of Attorney: Benedict Joseph M. CruzJson GalvezNo ratings yet
- United States Bankruptcy Court Southern District of New YorkDocument21 pagesUnited States Bankruptcy Court Southern District of New YorkChapter 11 DocketsNo ratings yet
- Eye Bags ReliefDocument27 pagesEye Bags ReliefNatsu DragneelNo ratings yet
- H I ĐĂNG Assigment 3 1641Document17 pagesH I ĐĂNG Assigment 3 1641Huynh Ngoc Hai Dang (FGW DN)No ratings yet
- Bula Defense M14 Operator's ManualDocument32 pagesBula Defense M14 Operator's ManualmeNo ratings yet
- HVAC Master Validation PlanDocument51 pagesHVAC Master Validation Plannavas197293% (30)
- ERIKS Dynamic SealsDocument28 pagesERIKS Dynamic Sealsdd82ddNo ratings yet
- Case Study IndieDocument6 pagesCase Study IndieDaniel YohannesNo ratings yet
- Pemaknaan School Well-Being Pada Siswa SMP: Indigenous ResearchDocument16 pagesPemaknaan School Well-Being Pada Siswa SMP: Indigenous ResearchAri HendriawanNo ratings yet
- Todo Matic PDFDocument12 pagesTodo Matic PDFSharrife JNo ratings yet
- Kaydon Dry Gas SealDocument12 pagesKaydon Dry Gas Sealxsi666No ratings yet
- DOE Tank Safety Workshop Presentation on Hydrogen Tank TestingDocument36 pagesDOE Tank Safety Workshop Presentation on Hydrogen Tank TestingAlex AbakumovNo ratings yet
- Sinclair User 1 Apr 1982Document68 pagesSinclair User 1 Apr 1982JasonWhite99No ratings yet
- Factors of Active Citizenship EducationDocument2 pagesFactors of Active Citizenship EducationmauïNo ratings yet
- Ratio Analysis of PIADocument16 pagesRatio Analysis of PIAMalik Saad Noman100% (5)
- Unit 14 Ergonomics Design: AND ProductDocument24 pagesUnit 14 Ergonomics Design: AND ProductRämêşh KątúřiNo ratings yet
- Get Oracle Order DetailsDocument4 pagesGet Oracle Order Detailssiva_lordNo ratings yet
- Managerial EconomicsDocument3 pagesManagerial EconomicsGuruKPONo ratings yet
- Key Fact Sheet (HBL FreedomAccount) - July 2019 PDFDocument1 pageKey Fact Sheet (HBL FreedomAccount) - July 2019 PDFBaD cHaUhDrYNo ratings yet
- Audi Q5: First Generation (Typ 8R 2008-2017)Document19 pagesAudi Q5: First Generation (Typ 8R 2008-2017)roberto100% (1)
- Srimanta Sankaradeva Universityof Health SciencesDocument3 pagesSrimanta Sankaradeva Universityof Health SciencesTemple RunNo ratings yet