You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Social and Political StratificationDocument59 pagesSocial and Political StratificationJoshkorro Geronimo100% (1)
- Challenges in Managing Employee DiversityDocument12 pagesChallenges in Managing Employee DiversityKavyaNo ratings yet
- Understanding Social Problems 10th Edition Ebook PDF VersionDocument61 pagesUnderstanding Social Problems 10th Edition Ebook PDF Versionjames.crandle290100% (34)
- By Heidi Box: Human Trafficking and Minorities: Vulnerability Compounded by DiscriminationDocument11 pagesBy Heidi Box: Human Trafficking and Minorities: Vulnerability Compounded by DiscriminationFrank BlakNo ratings yet
- FINAL For PUBLICATION Haringey Health Intelligence Data ReportDocument43 pagesFINAL For PUBLICATION Haringey Health Intelligence Data ReportMen's Health ForumNo ratings yet
- Men's Health Literature Review Dec2013 FINALDocument30 pagesMen's Health Literature Review Dec2013 FINALMen's Health ForumNo ratings yet
- MHF Cancer Saving Lives 2013 LRDocument58 pagesMHF Cancer Saving Lives 2013 LRMen's Health ForumNo ratings yet
- DWilkins Cancer APPG0 Mar14Document14 pagesDWilkins Cancer APPG0 Mar14Men's Health ForumNo ratings yet
- Tracey Cox 30-08-13Document4 pagesTracey Cox 30-08-13Men's Health ForumNo ratings yet
- Slide Deck MHW2013 V2reducedDocument19 pagesSlide Deck MHW2013 V2reducedMen's Health ForumNo ratings yet
- Ethical Policy - Revised2010.finalDocument3 pagesEthical Policy - Revised2010.finalMen's Health ForumNo ratings yet
- Ethical Policy - Revised2010.finalDocument3 pagesEthical Policy - Revised2010.finalMen's Health ForumNo ratings yet
- MHF Relate TryToSeeDocument26 pagesMHF Relate TryToSeeMen's Health ForumNo ratings yet
- MHF Cancer Saving Lives 2013 LRDocument58 pagesMHF Cancer Saving Lives 2013 LRMen's Health ForumNo ratings yet
- MH F Ethical PolicyDocument3 pagesMH F Ethical PolicyMen's Health ForumNo ratings yet
- Ethical Policy - Revised2010.finalDocument3 pagesEthical Policy - Revised2010.finalMen's Health ForumNo ratings yet
- Cancer Men Jan13Document6 pagesCancer Men Jan13Men's Health ForumNo ratings yet
- Examplepdf 4Document1 pageExamplepdf 4Men's Health ForumNo ratings yet
- Examplepdf 4Document1 pageExamplepdf 4Men's Health ForumNo ratings yet
- Examplepdf 4Document1 pageExamplepdf 4Men's Health ForumNo ratings yet
- Test DocumentDocument1 pageTest DocumentMen's Health ForumNo ratings yet
- Test DocumentDocument1 pageTest DocumentMen's Health ForumNo ratings yet
- Examplepdf 4Document1 pageExamplepdf 4Men's Health ForumNo ratings yet
- Examplepdf 4Document1 pageExamplepdf 4Men's Health ForumNo ratings yet
- Examplepdf 4Document1 pageExamplepdf 4Men's Health ForumNo ratings yet
- Test DocumentDocument1 pageTest DocumentMen's Health ForumNo ratings yet
- Test DocumentDocument1 pageTest DocumentMen's Health ForumNo ratings yet
- Examplepdf 4Document1 pageExamplepdf 4Men's Health ForumNo ratings yet
- Test DocumentDocument1 pageTest DocumentMen's Health ForumNo ratings yet
- Test DocumentDocument1 pageTest DocumentMen's Health ForumNo ratings yet
- Test DocumentDocument1 pageTest DocumentMen's Health ForumNo ratings yet
- Test DocumentDocument1 pageTest DocumentMen's Health ForumNo ratings yet
- Test DocumentDocument1 pageTest DocumentMen's Health ForumNo ratings yet
- Reaction Paper.Document2 pagesReaction Paper.Freylene SuyatNo ratings yet
- (Palgrave Socio-Legal Studies) Dave Cowan, Helen Carr, Alison Wallace - Ownership, Narrative, Things-Palgrave Macmillan UK (2018)Document243 pages(Palgrave Socio-Legal Studies) Dave Cowan, Helen Carr, Alison Wallace - Ownership, Narrative, Things-Palgrave Macmillan UK (2018)josezawadskyNo ratings yet
- Q2 SHS Understanding MelcDocument1 pageQ2 SHS Understanding MelcLeonilo C. Dumaguing Jr.No ratings yet
- Be FITbookDocument116 pagesBe FITbookmalvoNo ratings yet
- The Ideology of Colorblindness and White Supremacy: Guinier, L. & Torres, G. Martinez, EDocument18 pagesThe Ideology of Colorblindness and White Supremacy: Guinier, L. & Torres, G. Martinez, Eiam172No ratings yet
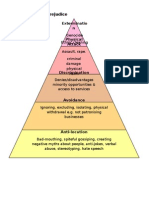
- Allports Scale of PrejudiceDocument1 pageAllports Scale of PrejudicebmckNo ratings yet
- A Critique of Catharine MacKinnons Sex-Based Theory of RapeDocument40 pagesA Critique of Catharine MacKinnons Sex-Based Theory of RapeShivank SinghNo ratings yet
- Gender and Food SystemsDocument23 pagesGender and Food SystemsAmbica SumbriaNo ratings yet
- Poverty Usa Webquest2Document3 pagesPoverty Usa Webquest2NickNo ratings yet
- Peace and Gender EqualityDocument2 pagesPeace and Gender EqualityKaila Clarisse CortezNo ratings yet
- Peace Report 2006-1Document66 pagesPeace Report 2006-1api-243171238No ratings yet
- Race and Ethnicity in The United States 8th Edition Schaefer Test BankDocument19 pagesRace and Ethnicity in The United States 8th Edition Schaefer Test Bankmrcharlesjohnsonfkwdxotzqc100% (32)
- RL 371 2019 Dor - 0Document49 pagesRL 371 2019 Dor - 0Srijil CM100% (1)
- Marco Scotini: Le Monde Est À NousDocument5 pagesMarco Scotini: Le Monde Est À NousLuciana BerneriNo ratings yet
- 11 - Ucsp Q2 - Modue 11 - Types of InequalityDocument18 pages11 - Ucsp Q2 - Modue 11 - Types of InequalityMichelleJewel MananghayaNo ratings yet
- Phelan Et Al. - 2010 - Social Conditions As Fundamental Causes of Health - 1Document13 pagesPhelan Et Al. - 2010 - Social Conditions As Fundamental Causes of Health - 1208322 Popoola Ibrahim INDUSTRIALNo ratings yet
- Springer Book Baisotti-VommaroDocument277 pagesSpringer Book Baisotti-VommaroGabriel LevitaNo ratings yet
- Haryana Government: Family Id EdishaDocument1 pageHaryana Government: Family Id EdishaSumit PalNo ratings yet
- (SV) The Best Place To Be A WomanDocument14 pages(SV) The Best Place To Be A Womanmarie lucasNo ratings yet
- Sample Diversity and Inclusion Questions For Employee SurveysDocument5 pagesSample Diversity and Inclusion Questions For Employee Surveysdr. samar SabraNo ratings yet
- Discrimination Against Whites by The NHS Sept 21Document7 pagesDiscrimination Against Whites by The NHS Sept 21Pria 72No ratings yet
- Sociology SyllabusDocument23 pagesSociology SyllabusSophia MK100% (1)
- Section I: A. Demographic Characteristics of Respondents. Table-1 N 30Document8 pagesSection I: A. Demographic Characteristics of Respondents. Table-1 N 30Srikutty DevuNo ratings yet
- Hesmondhalgh, Why Music Matters NotesDocument7 pagesHesmondhalgh, Why Music Matters NotesRichard ClareNo ratings yet
- Family Law AssignmentDocument2 pagesFamily Law AssignmentAnanthi NarayananNo ratings yet
- Does Education Promote Social Mobility - SupportDocument4 pagesDoes Education Promote Social Mobility - SupportLiew Shu EnNo ratings yet