You might also like
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Arterial PressureDocument7 pagesArterial PressureAmalina ZolkefleeNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Cardiac Conducting System in Health and DiseaseDocument5 pagesCardiac Conducting System in Health and DiseaseAmalina ZolkefleeNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Microscopic Structures of Cardiac CellDocument9 pagesMicroscopic Structures of Cardiac CellAmalina ZolkefleeNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Anatomy of Urinary Bladder and UrethraDocument16 pagesAnatomy of Urinary Bladder and UrethraAmalina ZolkefleeNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Blood CapillariesDocument7 pagesBlood CapillariesAmalina ZolkefleeNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Water, Fluid, Spaces and CompartmentsDocument15 pagesWater, Fluid, Spaces and CompartmentsAmalina ZolkefleeNo ratings yet
- Vessels ResistanceDocument10 pagesVessels ResistanceAmalina ZolkefleeNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Mouth, Larynx and TracheaDocument23 pagesMouth, Larynx and TracheaAmalina ZolkefleeNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Coronary CirculationDocument12 pagesThe Coronary CirculationAmalina ZolkefleeNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- 15-Urinary System Function and DevelopmentDocument3 pages15-Urinary System Function and DevelopmentMerryl BastilloNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- Normal Development of The Urogenital SystemDocument69 pagesNormal Development of The Urogenital SystembonziebuddyNo ratings yet
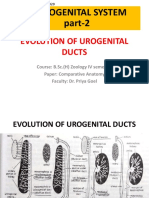
- Evolution of Urogenital Ducts Part-2 27.03.2020Document10 pagesEvolution of Urogenital Ducts Part-2 27.03.2020Sonali SahooNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- ICAR JRF/SRF Exam Question Bank for Veterinary StudentsDocument281 pagesICAR JRF/SRF Exam Question Bank for Veterinary StudentsHarish ShindeNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Embryology of The Renal SystemDocument8 pagesEmbryology of The Renal SystemStd DlshsiNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Embryology Notes emDocument25 pagesEmbryology Notes emAnonymous IwWT90VyNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Breast Anatomy and Development GuideDocument8 pagesBreast Anatomy and Development Guidekamie155No ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Embryolog Y By: Dr. Thaaer Mohammed Daher Alsaad M.B.Ch.B. (MBBS) F.I.B.M.S. (PHD) Senior Lecturer ISM MSUDocument97 pagesEmbryolog Y By: Dr. Thaaer Mohammed Daher Alsaad M.B.Ch.B. (MBBS) F.I.B.M.S. (PHD) Senior Lecturer ISM MSUSandipan MandalNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Development of Urogenital SystemDocument31 pagesDevelopment of Urogenital SystemPraney SlathiaNo ratings yet
- Exercise 8 Pig Embryo (Posterior Sections)Document16 pagesExercise 8 Pig Embryo (Posterior Sections)Gail AmuraoNo ratings yet
- Embryology of Urogenital SystemDocument42 pagesEmbryology of Urogenital SystemAngetile Kasanga100% (1)
- Development of The Urinary Organs (3rd - 4th Week)Document16 pagesDevelopment of The Urinary Organs (3rd - 4th Week)ridhaNo ratings yet
- Excretory System and OsmoregulationDocument10 pagesExcretory System and OsmoregulationShaira CogollodoNo ratings yet
- Urinogenital System in EnglisDocument27 pagesUrinogenital System in EnglisYogaPradiptaNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Vet Andrology and AI Dr. Pradeep Kumar PDFDocument146 pagesVet Andrology and AI Dr. Pradeep Kumar PDFDinesh PathakNo ratings yet
- AndrologyDocument93 pagesAndrologyhari krishnaa athotaNo ratings yet
- Evolution of KidneyDocument127 pagesEvolution of Kidneyanon_9692255300% (1)
- Aja 17 749Document7 pagesAja 17 749Eletícia SousaNo ratings yet
- Chapter 23 Kidneys and UretersDocument71 pagesChapter 23 Kidneys and UretersMACON824No ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Urinogenital SystemDocument11 pagesUrinogenital SystemAkinsola AyomidotunNo ratings yet
- MANISH - KANTI - BISWASUrino-genital System2020-05-04note Kidneyfinal 4-5-20Document11 pagesMANISH - KANTI - BISWASUrino-genital System2020-05-04note Kidneyfinal 4-5-20ShangNo ratings yet
- Development Urinary SystemDocument33 pagesDevelopment Urinary Systempavi7muruganathan75% (4)
- DEVELOPMENT OF PIG EMBRYODocument4 pagesDEVELOPMENT OF PIG EMBRYOAstrid AmadorNo ratings yet
- Chondrichthyes Excretory 2Document9 pagesChondrichthyes Excretory 2german guazaNo ratings yet
- Anatomy EponymsDocument12 pagesAnatomy EponymsAbialbon PaulNo ratings yet
- BIO 342 Comparative Vertebrate Anatomy Lecture Notes 10 - Urogenital SystemDocument4 pagesBIO 342 Comparative Vertebrate Anatomy Lecture Notes 10 - Urogenital SystemKatrina Lee GaganNo ratings yet
- Assignment 1 - InfertilityDocument41 pagesAssignment 1 - InfertilityRenu Ravina ChandNo ratings yet
- Labman Gus FinalDocument113 pagesLabman Gus FinalBryan CaldwellNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)