You might also like
- Report On Induced Abortion - Methods of Termination of Pregnancy Till 12 Wks of Gestation, Pre Abortion CounselingDocument4 pagesReport On Induced Abortion - Methods of Termination of Pregnancy Till 12 Wks of Gestation, Pre Abortion CounselingAdnan Akram, MD (Latvia)No ratings yet
- Infection During PregnancyDocument35 pagesInfection During PregnancyHusnawaty Dayu100% (2)
- Unit 3 Study GuideDocument10 pagesUnit 3 Study GuideangieswensonNo ratings yet
- Raheel OSCE Notes January 2023Document453 pagesRaheel OSCE Notes January 2023KamleshKumar100% (1)
- MAALOX (Drug Study)Document3 pagesMAALOX (Drug Study)Kian HerreraNo ratings yet
- Book Herbal Medication Herb Charts - Priest and PriestDocument27 pagesBook Herbal Medication Herb Charts - Priest and PriestAlejandra Guerrero100% (2)
- Gonorrhea and SyphilisDocument55 pagesGonorrhea and Syphilisjoshy221196No ratings yet
- Sexually Transmitted Infections and PregnancyDocument19 pagesSexually Transmitted Infections and PregnancyBeyins TiuNo ratings yet
- Slide 1 STIDocument50 pagesSlide 1 STIMatth N. ErejerNo ratings yet
- Sexually Transmitted DiseasesDocument17 pagesSexually Transmitted DiseasesChrystele Ann Ramilo100% (1)
- Torch Infection in Pregnancy: Neha Barari Assistant Professor SNSRDocument44 pagesTorch Infection in Pregnancy: Neha Barari Assistant Professor SNSRBhawna JoshiNo ratings yet
- Sexually Transmitted InfectionDocument11 pagesSexually Transmitted Infectionmark OrpillaNo ratings yet
- Gynaecology: Gum, Fertility, Contraception, and UrogynaecologyDocument46 pagesGynaecology: Gum, Fertility, Contraception, and UrogynaecologyOccamsRazorNo ratings yet
- PWH - NotesDocument140 pagesPWH - NotesjNo ratings yet
- 10 - Torch Pads KehamilanDocument43 pages10 - Torch Pads KehamilanMuhammad LutfiNo ratings yet
- Chapter 44 STIDocument5 pagesChapter 44 STIRebeccaNo ratings yet
- Vulvovaginal Infections, Cervicitis and Bartholin's Cyst: Suparna Chhibber, MDDocument44 pagesVulvovaginal Infections, Cervicitis and Bartholin's Cyst: Suparna Chhibber, MDTeguh Imana NugrahaNo ratings yet
- Tuberculosis in Obstetrics and GynecologyDocument42 pagesTuberculosis in Obstetrics and GynecologyameenNo ratings yet
- Sexually Transmitted DiseaseDocument3 pagesSexually Transmitted DiseaseBrianna ValerioNo ratings yet
- Reproductive Tract InformationDocument14 pagesReproductive Tract InformationGonçalo BaptistaNo ratings yet
- Torch Infection: Reporter: Zhao Meiling (Alice) Date: April.10.2019Document35 pagesTorch Infection: Reporter: Zhao Meiling (Alice) Date: April.10.2019Hilary WangNo ratings yet
- TORCH Infections: ICU NursingDocument27 pagesTORCH Infections: ICU NursingLouis Carlos Roderos0% (1)
- Infeksi in Pregnancy and PuerperiumDocument35 pagesInfeksi in Pregnancy and PuerperiumGerarld Immanuel KairupanNo ratings yet
- STD Family Medicine-WPS OfficeDocument25 pagesSTD Family Medicine-WPS OfficeJs JsNo ratings yet
- 3.torch InfectionsDocument15 pages3.torch InfectionsKuleshwar SahuNo ratings yet
- Nursing Care in Clients With General Disturbance inDocument48 pagesNursing Care in Clients With General Disturbance inJADE MAIKHA A. MIERGASNo ratings yet
- Approach To Vaginal Discharge: DR Faisal Al Hadad Consultant of Family Medicine & Occupational Health PSMMCDocument16 pagesApproach To Vaginal Discharge: DR Faisal Al Hadad Consultant of Family Medicine & Occupational Health PSMMCSupekshya ShresthaNo ratings yet
- Gynecology Notes Legal Issues and EthicsDocument19 pagesGynecology Notes Legal Issues and EthicsUsm LeeNo ratings yet
- Flagellates-2 by DR Gallardo: - MetronidazoleDocument7 pagesFlagellates-2 by DR Gallardo: - MetronidazoleJayricDepalobosNo ratings yet
- Lec.12 Genital Tract Infection (Part 1)Document26 pagesLec.12 Genital Tract Infection (Part 1)شريف محمد حسين شريف يوسفNo ratings yet
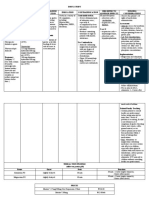
- Synonyms Causative Agents Incubatiob Period Mode of Transmission Signs and Symptoms Period of Communicability Diagnostic Test Medical Management Nursing Management ComplicationsDocument13 pagesSynonyms Causative Agents Incubatiob Period Mode of Transmission Signs and Symptoms Period of Communicability Diagnostic Test Medical Management Nursing Management ComplicationsYnah DominiqueNo ratings yet
- Definition-: Pelvic Inflammatory Disease (PID) Is A Sexually Transmitted Inflammatory Condition of TheDocument7 pagesDefinition-: Pelvic Inflammatory Disease (PID) Is A Sexually Transmitted Inflammatory Condition of TheanweshaNo ratings yet
- 10 TrichomonasDocument22 pages10 TrichomonasBoateng DerrickNo ratings yet
- Gynecological Disorders in Pregnanacy FinalDocument62 pagesGynecological Disorders in Pregnanacy Finalsanthiyasandy100% (2)
- Approach To Vaginal Discharge: DR Faisal Al Hadad Consultant of Family Medicine & Occupational Health PSMMCDocument16 pagesApproach To Vaginal Discharge: DR Faisal Al Hadad Consultant of Family Medicine & Occupational Health PSMMCSupekshya ShresthaNo ratings yet
- Miscarriage (Abortion)Document28 pagesMiscarriage (Abortion)readsa722No ratings yet
- Sexual Transmitted DiseaseDocument109 pagesSexual Transmitted DiseaseFRANCISCO, QUENNIE MARIE D.No ratings yet
- Common Complications of PregnancyDocument34 pagesCommon Complications of PregnancyiwennieNo ratings yet
- Communicable Diseases Affecting The Reproductive SystemDocument49 pagesCommunicable Diseases Affecting The Reproductive SystemJR Rolf NeuqeletNo ratings yet
- Upper Genital Tract Infection (PID)Document24 pagesUpper Genital Tract Infection (PID)Tofitofi TofiNo ratings yet
- Reproductive Tract Infections, Sexual Transmitted Diseases, and HIV in ObstetricDocument58 pagesReproductive Tract Infections, Sexual Transmitted Diseases, and HIV in ObstetricAbdulrahman NajiNo ratings yet
- Trichomonas VaginalsDocument15 pagesTrichomonas VaginalsDaniel AtiehNo ratings yet
- Infection in PregnancyDocument5 pagesInfection in PregnancyWasem A. JabbarNo ratings yet
- Dr. Dalia El-Shafei: Assistant Professor, Community Medicine Department, Zagazig UniversityDocument51 pagesDr. Dalia El-Shafei: Assistant Professor, Community Medicine Department, Zagazig UniversityArpit MahoreNo ratings yet
- Reproductive Tract InfectionsDocument46 pagesReproductive Tract Infectionskb100% (1)
- Tricho MoniasisDocument38 pagesTricho MoniasisAkhmad Ikhwan BaidlowiNo ratings yet
- Preinatal InfectionDocument33 pagesPreinatal Infectionاحمد احمدNo ratings yet
- Infection in Pregnancy ' JESDocument59 pagesInfection in Pregnancy ' JESmember12dNo ratings yet
- Infectious Diseases in PregnancyDocument8 pagesInfectious Diseases in PregnancyPabinaNo ratings yet
- Prom Preterm and PosttermDocument127 pagesProm Preterm and PosttermgibreilNo ratings yet
- Lower Genital Tract Infections & Sexually Transmitted DiseasesDocument38 pagesLower Genital Tract Infections & Sexually Transmitted Diseasesraed faisalNo ratings yet
- Case StudyDocument5 pagesCase StudyDeo Micah GoNo ratings yet
- 54.vaginal DischargeDocument40 pages54.vaginal DischargebenNo ratings yet
- PID & Ectopic PregnancyDocument23 pagesPID & Ectopic Pregnancy會 Ṧwahsa 會No ratings yet
- Pelvic Inflammatory DiseaseDocument25 pagesPelvic Inflammatory DiseasedeepaNo ratings yet
- Sexually Transmitted Disease STDDocument47 pagesSexually Transmitted Disease STDSurya DoleyNo ratings yet
- Pid 180131145647 1Document41 pagesPid 180131145647 1Smriti GroverNo ratings yet
- 24.11.09 PPT On Intrauterine InfectionDocument57 pages24.11.09 PPT On Intrauterine InfectionDhara Meena90% (10)
- Lection 8 SyphilisDocument39 pagesLection 8 SyphilisAtawna AtefNo ratings yet
- CASE REPORT - Syphilis in PregnancyDocument28 pagesCASE REPORT - Syphilis in PregnancymuhammadrubaiNo ratings yet
- Congenital Toxoplasmosis Treatment: D. Serranti, D. Buonsenso, P. ValentiniDocument6 pagesCongenital Toxoplasmosis Treatment: D. Serranti, D. Buonsenso, P. ValentiniAndra KurniantoNo ratings yet
- Clinical Teaching 4PEUPERAL SEPSISDocument5 pagesClinical Teaching 4PEUPERAL SEPSISAjit M Prasad Prasad100% (1)
- Vulvovaginitis: by James Holencik, DODocument70 pagesVulvovaginitis: by James Holencik, DOSyarifa YuliaNo ratings yet
- Guide to Pediatric Urology and Surgery in Clinical PracticeFrom EverandGuide to Pediatric Urology and Surgery in Clinical PracticeNo ratings yet
- Report On Etiology, Epidemiology, Clinic, DD, Treatment, Profilaxis of Typhoid Fever & ParathyphoidDocument3 pagesReport On Etiology, Epidemiology, Clinic, DD, Treatment, Profilaxis of Typhoid Fever & ParathyphoidAdnan Akram, MD (Latvia)No ratings yet
- Report On Etiology Pa Tho Genesis Treatment Principles of Food PoisoningDocument3 pagesReport On Etiology Pa Tho Genesis Treatment Principles of Food PoisoningAdnan Akram, MD (Latvia)No ratings yet
- Report On Etiological Structure and Epidemiology of The Acute Intestinal Infections. Pa Tho Genesis of Diarrohea Caused by Infectious Agents.Document3 pagesReport On Etiological Structure and Epidemiology of The Acute Intestinal Infections. Pa Tho Genesis of Diarrohea Caused by Infectious Agents.Adnan Akram, MD (Latvia)No ratings yet
- Report On Ethiology, Epidemiology, Pathogenesis, Clinical Features and The Treatment Principles of Cholera. Dehydration - Rehydration.Document2 pagesReport On Ethiology, Epidemiology, Pathogenesis, Clinical Features and The Treatment Principles of Cholera. Dehydration - Rehydration.Adnan Akram, MD (Latvia)No ratings yet
- The Infectious ProcessDocument4 pagesThe Infectious ProcessAdnan Akram, MD (Latvia)100% (1)
- 04.concept of Plant DiseaseDocument34 pages04.concept of Plant DiseaseLei Ann PunlaNo ratings yet
- Sign, Sypmtoms and Tretment of PosioningDocument18 pagesSign, Sypmtoms and Tretment of PosioningmaryamNo ratings yet
- 11-Acid-Base BalanceDocument28 pages11-Acid-Base BalanceKathlene BarasiNo ratings yet
- Case Study of PNEUMONIADocument12 pagesCase Study of PNEUMONIAAriaNo ratings yet
- COVID-19 - Evidence Over Hysteria - Zero HedgeDocument38 pagesCOVID-19 - Evidence Over Hysteria - Zero HedgeFabiana BNo ratings yet
- Bone GraftsDocument5 pagesBone GraftsNEPDOC OFFICIALNo ratings yet
- Care Plan Concept Map - RFIDocument1 pageCare Plan Concept Map - RFIsaraNo ratings yet
- Migraine Headaceh Treated With FamciclovirDocument2 pagesMigraine Headaceh Treated With FamciclovirReani ZulfaNo ratings yet
- Wksiteposter - en OSHADocument1 pageWksiteposter - en OSHARaúlNo ratings yet
- Acetaminophen - ParacetamolDocument3 pagesAcetaminophen - Paracetamolammar amerNo ratings yet
- Carpal Tunnel SyndromeDocument25 pagesCarpal Tunnel SyndromeFranky Sukwendy100% (1)
- Hypertension in Pregnancy - DerianDocument59 pagesHypertension in Pregnancy - Deriankevin jonathanNo ratings yet
- Pelvic Inflammatory DiseaseDocument48 pagesPelvic Inflammatory DiseaseAnonymouscatNo ratings yet
- Pertussis (Whooping Cough)Document14 pagesPertussis (Whooping Cough)CHALIE MEQUNo ratings yet
- MCQ Social MedicineDocument56 pagesMCQ Social MedicineKowsalya SelvarajNo ratings yet
- A Nationwide Population-Based Study On The Incidence of Parapharyngeal and Retropharyngeal Abscess-A 10-Year StudyDocument7 pagesA Nationwide Population-Based Study On The Incidence of Parapharyngeal and Retropharyngeal Abscess-A 10-Year StudyfayzaNo ratings yet
- 4c Aguilar Gasmen Quitoriano Rabena Valeros Viado VillalobosDocument19 pages4c Aguilar Gasmen Quitoriano Rabena Valeros Viado VillalobosBitz Basos ViadoNo ratings yet
- PANCE Quick HittersDocument5 pagesPANCE Quick HittersAndy BowmanNo ratings yet
- Anal and Perianal ConditionsDocument58 pagesAnal and Perianal ConditionsYonas YemidiralemNo ratings yet
- Brain and Bannisters Clinical Neurology Oxford Medical Publications by Roger Bannister PDFDocument7 pagesBrain and Bannisters Clinical Neurology Oxford Medical Publications by Roger Bannister PDFBennat RajNo ratings yet
- Dialog AnamnesisDocument2 pagesDialog AnamnesisMona Ahmd100% (1)
- Sepsis and Septic ShockDocument14 pagesSepsis and Septic ShockWaleedNo ratings yet
- Classification: Blood Sugar Insulin Hormone Pancreas HyperglycemiaDocument20 pagesClassification: Blood Sugar Insulin Hormone Pancreas Hyperglycemiabammu21No ratings yet
- Fibrous Tumors: Pgi Pauline BaluisDocument69 pagesFibrous Tumors: Pgi Pauline BaluisPahw BaluisNo ratings yet
- History Taking in OptometryDocument8 pagesHistory Taking in Optometrybhuvana100% (1)
- DepakoteDocument2 pagesDepakotedana100% (1)
- LESSON-4-SYSTEMIC-MYCOSIS - Donasco HandoutsDocument8 pagesLESSON-4-SYSTEMIC-MYCOSIS - Donasco HandoutsKhay Mae DonascoNo ratings yet