Professional Documents
Culture Documents
Pharmacology Final Study Guide
Uploaded by
Anthony PalladenoCopyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Pharmacology Final Study Guide
Uploaded by
Anthony PalladenoCopyright:
Available Formats
1
Pharmacology PHARMACODYNAMICS AND KINETICS
PHARMACOLOGY A. Testing Sequence (FDA) 1. animal testing (LD50) 2. Phase I Clinical trials for safety 3. Phase II Clinical trials for effectiveness 4. Phase III expanded clinical trials (double blind) 5. Phase IV - post market surveillance report problems via web page II. Legislation A. Orphan Drug Act (1983) In response to under-treatment of rare diseases, the bill stimulated research of drug therapies for these diseases and added safety research. B. Controlled Substances Act (1970) 1. Added scheduling to controlled substances:
2. 3.
Nurse who gives controlled substance to someone other than prescribed commits federal crime. Unlabeled uses of drugs - After the FDA approves a drug for one use, an MD legally may prescribe it for any labeled or unlabeled indication. But the manufacturer cannot advertise it for an unlabeled use. And insurance companies may not pay for prescribed medications indicated for unlabeled uses.
Drugs bought via internet may be bogus OTC Drugs A legal loophole allows manufacturers to change the ingredients without changing the name. Ex: Maalox used to have Al and Mg hydroxides. Now there are many Maalox products, none of which have the original Al and Mg formula. Risks of OTC drug use: 1. Self-diagnosis (patients may use the drug to treat an improper self-diagnosis) 2. Potent drugs 3. Undesirable effects (Many side effects) 4. Drug interactions (Many pts dont report use) 5. Drug toxicity (Many pts overuse OTCs) OTC safety There is a low incidence of adverse effects and low potential for harm assuming proper instructions and warnings on label ASSUMING YOU FOLLOW INSTRUCTIONS (proper route, dose, administration)! OTC Effectiveness Drug, when taken properly, will provide relief of minor sxs or illness in a significant portion of the population. Components of an OTC drug label: Active ingredients/amount in each dosage unit Purpose Uses (indications) Specific warnings (when not to use, when to consult with physician or pharmacist, adverse effects, substances or activities to avoid) Dosage instructions (when, how, and how often to take)
2 Inactive ingredients (important for those with specific allergies
III. Sources of Drugs A. Plants 1. Alkaloids - act as alkali - react with acids to form salts which are soluble. Ends in "ine" - eg. caffeine, nicotine. 2. Glycosides Names usually end in in eg. Digoxin. Glycosides hydrolyze into organic molecules. 3. Gums - Plant exudates. 4. Resins - Semisolid or solid plant exudates that are insoluble in water; soluble in ETOH. 5. Oils - highly viscous oils that are insoluble in water. eg. peppermint oil, castor oil. B. Animals 1. Hormones 2. Enzymes 3. Sera - Fluids (serum) C. Minerals ie iron, iodine D. Recombinant DNA (Bacterial, viral, etc.) i.e. hepatitis vaccine, FeLeuk. Drug names: Chemical - 7-chloro-1,3-dihydro-1-methyl-5-phyenyl-2H-1,4-benzodiazepin-2-one Generic: diazepam Trade: valium Drugs that have similar characteristics are grouped as a class [eg blockers]. Can also group by therapeutic use [eg. antihypertensives = includes blockers, diuretics] GENERAL PRINCIPLES OF DRUG ACTION 1. 2. 3. Drugs do not create function. Drugs modify existing functions within the body. No drug has only one action. Therefore: there is no such thing as a benign drug. Drug action is determined by how the drug interacts with the body. DRUG FORMULATIONS 1. 2. 3. 4. 5. Compressed tablet - most common - thin coating to help swallow Sustained release - enteric coated, or beads, or drug embedded in a slowly eroding matrix - eg slow-k Repeat action tabs - initial dose in outer shell, second dose in inner shell Osmotic pump - tabs with semipermeable membrane covering which allows water to enter. Drug leaves through a small laser drilled hole. Eg acutrim Also chewable tabs, sl tabs, buccal tabs 6. Transdermal patches 7. Implants (eg. Norplant) 8. Polymers - use biodegradable polymers impregnated with drug - implant next to tumors. 9. Pacifiers and lollipops The dose of a medication is generally not the same via different routes! Especially when going from PO to parenteral. 1. Other drugs that need major dose adjustment (when changing routes) Enalapril [Vasotec] Diltiazem [Cardizem] Hydromorphone [Dilaudid] Labetalol [Normodyne] Levothyroxine Morphine Propranalol [Inderal] PHARMACOKINETICS Pharmacokinetics: The alteration of drugs in the body [absorption, distribution, metabolism, excretion] I. CELL MEMBRANES
3 A. proteins in the cell membrane can be: 1. functional eg enzymes 2. receptor sites 3. channels through which ions or molecules can pass certain drugs can open or close the channels, thus regulating flow of ions & molecules into or out of the cell. B. Movement across cell membranes 1. Passive transport (3) types: a. Diffusion - Major way to get drugs into bloodstream and cells. Direct movement of solute to area of lower concentration. No energy involved. Drug must be soluble and lack electric charge Convective absorption [filtration] - Drug moves through pores in membrane along with fluid. Driven by pressure gradient [either osmotic or hydrostatic] Also important in excretion.
b.
Carrier mediated diffusion [facilitated diffusion] - [minor role] - Drug binds to carrier protein on cell membrane to cross into the cell. 2. Active transport - Proteins on cell membrane pump the drug across against concentration gradient. Requires ATP. Important in excretion of drugs. 3. Pinocytosis - cell membrane engulfs the drug - [minor process] II. ABSORPTION Absorption: The process by which a drug moves across one or more cell membranes from its site of administration into the bloodstream. Factors influencing absorption 1. Route of administration - enteral, parenteral, topical, etc. affects rate of onset 2. Drug solubility A. In water - if po, the drug must dissolve in aqueous contents of GI tract. The faster this happens, the faster the drug will be absorbed. *Thus, liquid drugs are absorbed faster than pills. (suspensions are solid particles in a liquid) B. In lipids - essential for drug to diffuse across cell membranes [which are lipid-rich] such as in CNS - Blood Brain Barrier 3. pH and drug ionization Drug can be ionized or nonionized. Ionized molecules do not diffuse easily across lipid membranes and thus are poorly absorbed. Nonionized molecules are very lipid soluble and thus easily absorbed. Usually some molecules of a drug are ionized and some nonionized. pH is major factor which determines the amount of drug molecules that will be ionized or nonionized [and thus how easily absorbed] Most molecules of a basic drug will be nonionized in alkaline ph. Most molecules of an acidic drug will be nonionized in an acid ph. 4. Stability of drug in acid Some drugs are inactivated [all or partly], or precipitated by stomach acids and enzymes. Therefore, such drugs cannot be given PO, or are formulated with enteric coating so that the drug bypasses the stomach acid. 5. Local blood flow Anything that reduces blood flow slows absorption. PO - Strenuous exercise diverts blood from stomach which causes slowed absorption. Food stimulates blood flow to GI viscera & may increase absorption. IM - exercise increases absorption. Blood flow is also important in distribution. Ischemia results in decreased distribution. 6. GI motility (PO route) Increased motility less time for absorption less absorption.
c.
4 Decreased motility more time more absorption (can lead to toxicity) Bariatric surgery causes decreased absorption of fat soluble vitamins and Ca++. May need supplements. Also, extended release meds will spend less time in stomach and more in small intestine (affecting absorption) Intestine greater dose release. Liquid meds may be better as dont need time to dissolve before absorption. Calcium carbonate needs high acid environment for dissolution and absorption, Calcium citrate does not, so citrate is preferred. Avoid NSAIDS and bisphosphonates (fosamax) since smaller stomach size can increase ulceration risk. Surface area - Because of large surface area covered with villi, small intestine is where most drug absorption occurs [even acid drugs like ASA ] Pain and stress - Decrease absorption. Exact cause not known. Could be reduced GI motility, dec. Blood flow
7. 8.
III. DISTRIBUTION Distribution: Movement of drug from bloodstream across cell membrane to tissue. Generally quicker and easier than absorption. 1. Plasma protein binding Drugs in the bloodstream are either free or bound to plasma proteins [esp albumin] Only free molecules of drug can produce drug effects Only free drug molecules can be metabolized or excreted. Bound molecules are pharmacologically inactive. Chemical structure of the drug determines what percentage will be bound at any one time and how strong the bond is. Another factor is amount of albumin available. Fraction of total free molecules varies from drug to drug. Can range from nearly 0-nearly 100%. Eg. Acetaminophen is almost all free Gentamicin is 90% free Coumadin is only 1% free Plasma binding is: 1. Reversible - as free drug molecules are metabolized and excreted, they are replaced by previously bound molecules. This keeps relatively constant % free molecules 2. Nonspecific - proteins bind with many different drugs *Drugs will compete for binding sites. Stronger bonding drugs replace weaker. If drugs have same bond strength the one present in greatest concentration will win. Strong effect on drug concentrations! One drug can displace another from binding sites! Hypoalbuminemia - common in elderly & pregnant - can cause overdose effects. 1. Blood-brain barrier - Capillary endothelial cells in brain tissue more "tightly touching" than elsewhere. Makes it harder for drugs to cross. Drugs must be lipid soluble and not tightly protein bound to cross well [anesthetic gases, ETOH, anxiolytics, barbiturates] Antibiotics don't cross well. 2. Placental barrier - 2d capillary network. Not very efficient. Many drugs cross including ETOH can cross and cause teratogenic effects. 3. Storage or accumulation sites A. Fat - For lipid soluble drugs. Release from fat cells into bloodstream is slow and is initiated usually after administration is stopped. i.e. general anesthetics. B. Bone and teeth - for drugs which bind to calcium ions. C. Kidneys There is a large blood flow to the kidneys and they receive a lot of drug exposure. Many drugs can tax the kidneys. Important in heavy metal poisoning - Pb and Hg can reach toxic levels in kidneys. IV. BIOTRANSFORMATION [aka METABOLISM] Biotransformation: The chemical and/or biological changes in the drug within the body. a. Transforms parent drug into metabolites that usually have less pharmacologic activity. b. Transforms parent drug into metabolites that are more water soluble so they can be excreted. *Only free drug molecules can be metabolized. Major site: Liver Metabolism is divided into two types: Phase I Metabolism - Involves enzyme action by oxidation, reduction, or hydrolysis. Oxidation is the most common mechanism drug metabolism. Usually results in detoxification and subsequent elimination of the
5 drug or the activation of the prodrug. Phase II Metabolism - Mainly conjugation of endogenous substrates such as acetate, glucoronic acid, glutathione, glycine, or sulfate. This may happen with the parent molecule, an activated prodrug, or a metabolite after Phase I metabolism. Most drugs are active drugs in parent form and are metabolized into inactive or less active metabolites. Prodrugs are inactive in parent form and are metabolized into active drug. eg: levodopa dopamine. Some drugs are less active parent metabolized to more active drug. eg: codeine--->morphine Some drugs cannot be metabolized and pass through biotransformation unchanged. eg: aminoglycosides
1. 2. 3. 4.
A. Hepatic Drug Metabolism 1. Microsomal enzymes - Reside in the endoplasmic reticulum of hepatocytes. These enzymes metabolize drugs. Oxidation is the most common mechanism of metabolism. The microsomal enzymes of Cytochrome P450 (CYP) catalyze most of these oxidative reactions. There are at least 32 different forms of P450s in humans and they are the most important enzymes in drug metabolism. 2. First Pass Effect - PO drugs are absorbed into portal circulation from GI tract and reach the liver before entering the systemic circulation. Thus, drug is metabolized right away. Some drugs are so sensitive to first pass effect that they cannot be given PO. Overcome first pass by giving "loading doses" of drugs ---->enzymes become saturated with drug molecules and first pass effect decreases. B. Factors influencing hepatic metabolism 1. Age - Normal enzyme activity not reached until puberty and declines after age 60. *Young and Old more prone to drug accumulation. Doses need to be lower even if calculated on body weight 2. Nutrition - Serious nutritional deficiencies can cause an impaired enzyme system. 3. Disease - Any damage to liver cells or decreased blood flow to the liver can cause potential problems. 4. Hormones Decreased enzymes with deficiencies of: insulin thyroid corticosteroids Increased metabolism with hyperthyroidism Progesterone & estrogen fluctuations in pregnancy and menstrual cycle seem to have an effect 5. Drugs (& substances) that inhibit hepatic enzymes a. Some drugs compete for enzymes causing interactions b. Some drugs inhibit enzyme activity resulting in accumulation of concurrent drugs using the same pathway. c. Some substances suppress enzymes because they are toxic to liver cells. eg: ETOH, carbon tetrachloride. 6. Drugs that stimulate hepatic enzymes [inducers] a) Autoinduction: some drugs stimulate enzyme activity for their own metabolism resulting in less active drug in body. Autoinduction results in tolerance a decreased response to a dose of a drug that previously gave a greater response. b) Foreign induction - some drugs stimulate metabolism of other drugs (drug interaction). 7. Genetic factors Pharmacogenetics: the study of genetic factors responsible for variations in responses to drugs. There are at least 3 phenotypes: EMs = extensive metabolizers most of the population PMs = poor metabolizers or metabolize slowly. These people are prone to accumulation and increased adverse reactions. When given a prodrug, these people may have little or no clinical response. UEMs = ultraextensive metabolizers increased metabolism may result in subtherapeutic levels with regular doses. Some drugs are metabolized in similar manner through acetylation. Acetylation - addition of acetyl group. Some ethnic groups have better capability of acetylation. Orientals = rapid metab Middle-Eastern peoples = slow metab Native Americans = half fast, half slow 8. Environment eg. smoking causes metabolize theophylline faster than nonsmoker. C. Other Metabolism Sites lungs, GI mucosa, kidneys, blood. But these sites have a minor role V. EXCRETION [aka clearance]
6 Most drugs are excreted by the kidneys and eliminated in the urine. Drug with high clearance rate is removed quickly. Low clearance rate --> slow removal. Dialysis is alternate form of excretion. A. Glomerular Filtration Glomerular Filtration: The process by which small lipid-soluble drug molecules (or metabolites) diffuse from the bloodstream into what will become the urine. Driving force is glomerular filtration pressure which is determined by blood pressure. 1. Only drug molecules that are "free" will be filtered. 2. Nonionized molecules are more likely to be filtered. 3. Drugs & diseases that reduce glomerular filtration rate will decrease removal of drugs and vice versa. B. Tubular Secretion Tubular Secretion: Kidney tubules contain specialized "pumps" that secrete drug molecules into the urine. Requires ATP, but is very efficient. 1. Several pumps exist and some are very specialized. But many drugs are chemically similar enough to share the same pump. Such drugs compete for transport. *This can cause important drug-drug interactions. ie: probenecid competes for transport with methotrexate and this can cause toxicity (drug not eliminated exists in high levels) C. Tubular Reabsorption and Effects of urine pH Tubular Reabsorption: return of drug molecules from urine into blood. 1. Same factors influence tubular reabsorption as with primary drug absorption. 2. Nonionized and lipid soluble drugs will be reabsorbed a lot and thus not eliminated quickly. 3. Urine pH influences whether drug molecule is ionized or not. ie: ASA in normally acidic urine is nonionized, thus readily reabsorbed. One way to treat ASA overdose is to give something which increases urine pH to cause less reabsorption and more excretion [Na bicarb] D. Elimination via Feces 1. Some drugs are concentrated in bile, excreted into intestines and eliminated via feces. 2. Enterohepatic Recycling: Some such drugs can be reabsorbed from lower GI tract [just like tubular reabsorption]. Important in drug toxicity, reabsorption needs to be interrupted to stop the recycling. eg. dig tox - cholestyramine binds with digoxin in GI tract & increases excretion. E. Elimination via Lungs 1. Some drugs diffuse from bloodstream into alveoli. Usually major portion of the drug is eliminated via kidney. Other minor elimination can occur via sweat, tears, saliva, mother's milk. VI. TIME ASPECTS A. Oral Administration 1. Onset [aka latent period]: The time between the administration of a drug and the first appearance of its effects. Once this response occurs, its intensity increases greatly in a short time. 2. Peak action [time to peak effect]: Time from drug administration to the development of maximum effect. During this time drug is being absorbed and distributed faster than it is being eliminated. Once peak effect and concentration are reached, they begin to decline. 3. Duration of action: Time from appearance of response to disappearance of response. B. IV Administration Blood levels rise immediately, reach a peak, and decline. C. Plasma Half-Life Half-Life: The time needed for the plasma concentration of a drug to fall to 50% of its previous concentration. 1. *NOT dependent on route of administration. Usually a constant fraction eliminated with each life. 2. Most drugs are 97% eliminated after five half-lives. Also takes 5 half-lives to achieve steady state. 3. Implications for dosing schedules: longer half-life means less frequent doses are needed, but steady state takes longer to reach. D. Plateau Principle [aka Steady State] Plateau Principle: when a constant dose of a drug is given at regular intervals, the concentration of drug in the blood will eventually reach a constant level and remain there until something changes. 1. Since drug effect is related to blood level, once steady state is reached, response to drug will be relatively constant.
7 2. Drug blood level does fluctuate somewhat within the steady state. 3. Reason for consistent dosage schedules. 4. Ways to reach steady state quickly when drug has long half-life: a) Give first dose IV, then other doses po. b) Give loading dose, then maintenance doses. c) Give IV bolus, then slow IV drip. BIOAVAILABILITY Bioavailability: the extent to which a drug's active ingredient is absorbed & transported to its site of action. 1. Bioavailability is affected by: a. solubility b. crystalline structure c. particle size d. polarity 2. Bioavailability is important because different brands of same drug can have different bioavailability eg. Digoxin BLOOD CONCENTRATION LEVEL MEC = minimum effective concentration MTC = minimum toxic concentration (Lowest blood concentration at which adverse reactions usually occur.) Therapeutic Range is bordered at the low end by MEC and on top by MTC. Time during which drug concentration remains between these levels is duration. Peaks are drawn at the estimated peak of the drug to ensure therapeutic levels Troughs are drawn before administration of the next dose to protect against toxicity Both help achieve the steady state through proper assessment of drug half-life and therapeutic levels. PHARMACODYNAMICS Pharmacodynamics: effects of drugs on living tissues. How drugs exert their effects. [aka drug action] A. Drug-enzyme Interactions Enzymes are protein substances which act as catalyst. Sometimes the enzyme thinks the drug is its substrate. This interaction could be a source of a drug response. eg. neostigmine inhibits the enzyme acetylcholinesterase which causes acetylcholine B. Nutrient effect on cell function Vitamins and trace elements modify cell function. Excess amounts can lead to problems. C. Second Messengers 1. Second Messenger: a chemical synthesized as a result of the drug-receptor interaction. 2. Often the link between drug binding to a receptor and eventual response. ie: some drugs interact with receptors on muscle cell which activates an enzyme [adenylate cyclase] which increases formation of cyclic AMP which is the second messenger. cAMP increases the flow of Ca++ ions into the cell which initiates muscular contraction. D. Receptors 1. Many drugs interact with specific sites on cell's outer membrane. These sites are called receptors. Cells may have thousands of receptors. Ligands are endogenous substances [such as hormones, neurotransmitters] that interact with receptors to cause a response. 2. Receptors have shapes that are specific for particular drugs. Lock and Key 1) Drug molecules = keys. Receptor sites = locks. 2) Keys have shapes which fit the locks. Some keys fit exactly and turn the lock = agonists. Some keys fit in but don't turn the lock = antagonists. If antagonist key is in the lock, agonist cannot be inserted. Some keys are 'master keys' which fit many locks. 3. Receptors are, or are near, enzyme systems or ion channels that control some basic cellular process. E. RECEPTOR NUMBER AND RESPONSE 1. Up-regulation = increased # of receptors
8 2. eg: thyroid hormone increases # of some cardiac receptors Down-regulation = decreased # of receptors.
F. Agonists 1. Agonists: Drugs that bind to a receptor and stimulate it (produce an effect). 2. Many agonists are endogenous ie: neurotransmitter, hormones. Many drugs are chemically very similar to endogenous agonists. 3. Agonists must have affinity and efficacy. 4. Affinity: Agonists molecule can interact with, bind to, or occupy a specific receptor site. Drug-receptor interaction is not permanent, but is dynamic process of association and disassociation. Thus other substances can also bind with sites while agonist is around, and agonist can bind to lots of sites in a short time. 5. Efficacy: Ability of an agonist to cause a response. G. Antagonists [aka receptor blocker] 1. Antagonist: Drugs which bind to a receptor and prevent it from being stimulated by an agonist. [Affinity but no efficacy] 2. Antagonists do not create new effects. H. Types of Antagonism 1. Competitive antagonism [aka surmountable]: Agonist & antagonist compete for receptor sites. Antagonist keeps some agonist molecules from binding resulting in a diminished response. If the antagonism can be overcome by giving more agonist, the antagonism is competitive. Most common type of antagonism. a) Cell has spare receptors so enough are open to allow agonist to produce response if enough is given. b) Antagonist binding is also not permanent allowing time for agonist binding. 2. Noncompetitive antagonism: A blockade produced by antagonist CANNOT be overcome. Few clinical agents are noncompetitive. (eg. nerve gases) a) Binding is tight and for a much longer time, so agonists have little chance to bind. b) Antagonist may bind to receptor next to the agonist receptor and in the process, changes the shape of the agonist receptor so it no longer recognizes the agonist. 3. Biochemical antagonism: The process by which one drug decreases the amount of another drug that is available within the body decreasing agonist effect. *May be due to the ability of drug to decrease absorption, increase excretion, or alter metabolism of other drug. 4. Chemical antagonism: Inhibition or total loss of a drug's action as a result of its chemical interaction with another substance. 5. Physiologic antagonism: Two agonists act with different receptors and their effects cancel each other. F. Actions Not Using Specific Receptors 1. Direct physical or chemical action. Not on a cell ie: antacids = chemically neutralize stomach acid osmotic diuretics = physical action of increasing osmotic pressure. 2. Action on or in cells but no receptor. ie: general anesthetics alter electrical properties of nerve cells CA drugs alter metabolism of chemicals essential for cell function. Penicillin alters cell metabolism of bacterial cells Selective Toxicity - Ideal drug acts only on the system which you want to effect. Penicillin acts only on bacterial cells. Thus, low toxicity. However, CA drugs act on enzyme processes that occur in all cells --> high toxicity. Drug Potency = the relative amt of drug needed to produce desired response Drug Efficacy = relates to the maximal response of effect achieved when the dose-response curve reaches its plateau
II. FACTORS THAT ALTER DRUG RESPONSE [variation in response = drug polymorphism A. Gender 1. Pregnancy - uterine response to methergine 2. Males absorb IM's better than females 2d less fat in the muscles 3. Female has more fat and less body water than male. B. Genetics - Pharmacogenomics = study of the role of inherited and acquired genetic variation in drug response. 1. Some differences in sensitivity & resistance is usually due to differences in rate of acetylation 2. Idiosyncracy = genetically determined variability that falls outside the expected range of reaction.
9 Lack of enzymes or coenzymes can lead to drug toxicity or alter drug effect. eg: G6pd deficiency can cause hemolytic anemia if given drugs that need G6pd to metabolize [often found in Mediterranean and blacks.] Drugs: quinidine, quinine, sulfa, etc. 4. Specific known differences 1) ETOH - metabolized by the liver enzyme alcohol dehydrogenase in Caucasians. But in Asians ETOH is metabolized by aldehyde dehydrogenase - which works faster, often causing circulatory & unpleasant effects - ie. Facial flushing & palpitations. 2) Caffeine - excreted faster by Caucasians than Asians 3) Antihypertensives - blacks need higher doses of beta blockers than whites. Chinese men need about 2X the dose as white men. 4) Psychotropics - potential for unusually high plasma concentrations in Asian pts. 5) Eye color can be a factor - light eyes dilate wider in response to mydriatic drugs than dark eyes. 6) Warfarin genetic differences in CYP enzymes and in a specific Vit K subunit account for 30-40% of the variation in Coumadin dose needed to get correct INR. In 2010, FDA revised label on warfarin to provide genotype specific dose ranges. 7) Clopidogrel [Plavix] FDA warning (2010) that persons with a CYP variant had a low rate of metabolism for plavix and might need dose adjustment or another drug. 8) Anti-infectives may have serious side effects if given to patients with certain genetic differences. (eg hepatotoxicity with floxacillin, bad hypersensitivity to abacavir) C. Anti-cancer drugs have to consider to genomes pt and cancer. There are now many examples of pharmacogenetic tests paired with anticancer drugs that are considered part of routine care. 3. Pathophysiology 1. Presence of disease can affect drug action. ie: asa and fever 2. Renal disease causes altered excretion. Use creatinine clearance to assess GFR. Also, secondary effects due to anemia, protein and electrolyte imbalances, etc. 3. Liver disease causes altered metabolism. Also altered protein binding 4. Decreased CO leads to increase time for distribution. Especially in patients with shock which leads to decreased peripheral circulation and decreased distribution. 5. GI Disease Causes malabsorption. Especially if a lot of the small intestine has been removed. Hypo or hyper motility Drugs pass through without being absorbed, or are absorbed in high amounts. Decreased stomach acid production Decreased absorption of drugs needing acid environment. 6. Increased or decreased thyroid function Increased or decreased metabolism of drugs. Requires dose adjustment. Body Build 1. Directly influences drug dosage required. a. Muscle increased release of creatinine from muscle breakdown can cause mistakes in dosages that are based on creatinine clearance. b. Fat - important in fat soluble drugs - may need dose adjustment if the patient is significantly overweight. D. Diet 1. Presence of food in stomach can change absorption. 2. Maintain adequate protein intake support proper albumin levels used in plasma binding. 3. High protein and low carb diet tends to promote rapid metabolism. So eat green vegetables and charcoal broiled foods. 4. High protein or high fat diet may decrease biliary excretion. High fiber increases biliary excretion. 5. Obesity leads to more extensive distribution of lipid-soluble drugs and decreased drug bioavailability. Circadian Rhythms 1. Timing within rhythm influences drug action. Chronotherapeutics 1) Digoxin 2) Steroids for asthma work better when given at 3 pm (better to have the peak between 3 and 5 am when attacks are most frequent.) 3) H2 blockers at 7 pm with dinner are the best time. Circadian rhythm of stomach acid peaks in evening and later at night. E. Drug History 1. Abuse leads to alterations in drug action. 2. Alcoholism causes liver damage F. 1. 2. 3. 4. Psychosocial Economics Patient may not be able to buy the medications. Health beliefs, emotions, and compliance Placebo effect: ANY response related to drug administration that cannot be attributed to the pharmacodynamics of a drug. Cultural practices and beliefs
10 5. Self-medication G. Drug Administration Dosage schedule: QID should be q6h. *Drugs with long half-lives are not that critical. *Regular drug administration schedules help compliance. J. 1. 2. 3. Age Neonates: Immature organ systems, small body mass, low fat content, high water content, greater membrane permeability result in very different responses to drugs. Children under 12 - Metabolize some drugs in a way that yields unusual effects because of immature systems and functions. Elderly - Many physiologic changes at a time when more drugs are likely to be taken. Elderly have problems both from overprescribing and underprescribing. Studies have shown that beat blockers are underprescribed for elderly, even though they have been proven effective. Also, hormone therapy is underused by older women. Elderly are also more likely to have inadequate pain meds prescribed. a) Absorption - few significant differences. Slower but still as complete First pass elimination declines. May need smaller doses. b) Distribution - *Serum albumin decreases resulting in more free drug available. - Overall increase in fat and decrease in total body water causes changes in distribution (r/t volume distribution) c) Metabolism - Declines. Liver enzymes lose effectiveness. Hepatic blood flow decreases. d) Excretion - Reduced glomerular filtration rate. Decreased rate of excretion. Also, smaller renal reserve increases susceptibility to nephrotoxic effects of drugs. e) Altered tissue sensitivity - Certain receptors change which generates greatly enhanced effects of drugs. ie: barbiturates 1) receptors decrease in quantity and efficiency so elderly have a diminished response to adrenergics and an increased risk of toxicity with blockers. 2) Decreased dopamine in brain causes increased susceptibility to extrapyramidal effects 3) Decreased effectiveness of blood-brain barrier may cause high incidence of drug induced behavioral changes and accumulation of lipid soluble drugs. f) Hormonal changes - Many drugs act through hormonal mechanisms and thus may elicit altered responses because of reduced endocrine secretion as the aging process continues. (ie: increased susceptibility to DM generated by steroids.) g) Chronic disease states - Alters organ function and response to drugs. Also, change in body's response to disease states (eg temp & infection) h) Polypharmacy - Many prescribed drugs. Leads to greater chance of drug interactions. i) Behavioral changes - loss of memory, confusion can lead to incorrect dosages, etc. j) Sensory alterations - loss of hearing and vision breeds drug errors. k) Economics - drugs cost! More than 40% of all Medicare enrollees have no coverage for outpatient drugs. Give as few drugs as possible and in smallest doses possible.
Other Changes with the Elderly: Physiologic changes in elderly and pharmacokinetic/dynamic alterations Physiologic change Increased gastric pH Increased body fat Decreased body water Decreased serum albumin Decreased cardiac output Decreased renal blood flow Decreased GI blood flow Decreased liver mass and hepatic blood flow Receptor site change CNS changes Sensory changes Endocrine changes CV changes Pharmacokinetic/dynamic alteration Decreased absorption of drugs ionized at low pH Decreased fat soluble drug concentration Increased water soluble drug concentration Increased unbound drug Decreased metabolism & excretion Decreased excretion Decreased absorption of po drugs; decreased metabolism, excretion Decreased metabolism Increased or decreased drug activity Increased response to depressants More likely cognitive impairment Increased risk of drug induced glaucoma Increased resistance to insulin Decreased response to cardiac stimulants Decreased autonomic compensations
11 GI changes Reproductive Musculoskeletal More susceptible to drug induced constipation, etc More sensitive to drug SE affecting sexual function Increase weakness from muscle relaxants
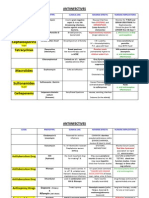
INAPPROPRIATE DRUGS FOR THE ELDERLY Sedative of Hypnotic Agents Long acting benzodiazepines (Valium, Librium, Dalmane) Associated with daytime sedation and [risk of falls Meprobamate (Equanil) - less safe than short acting benzodiazepines The barbiturates pentobarbital (Nembutal) and secobarbital (Seconal) benzodiazepines are safer for sedation and phenobarbital is preferred for seizures. Antidepressants Amitriptyline (Elavil) - has more orthostatic hypotension and anticholinergic effects than other antidepressants. NSAIDS Indomethacin (Indocin) - greater CNS toxicity than other NSAIDS Phenylbutazone (Azolid) - risk of bone marrow toxicity. Both of the above may be indicated for some conditions Oral Hypoglycemics chlorpropamide (Diabenase) - risk of SIADH Analgesics Propoxyphene (Darvon) - ineffective, low toxic-to-therapeutic ratio may B> CNS & cardiac toxicity. Pentazocine (Talwin) - overdose can B> seizures and cardiac toxicity Dementia Treatments Isoxsuprine (Vasodilan) and cyclandelate (Cyclan) - not effective Platelet inhibitors Dipyridamole (Persantine) - use OK only as adjunct to Coumadin for pts with artificial heart valves. Efficacy in other uses is doubted and can B> HA, dizziness and CNS disturbances. Muscle relaxants or antispasmodics cyclobenzaprine (Flexeril), methocarbamol (Robaxin), carisoprodol (Soma), orphenadrine (Flexon). The protential for CNS toxicity is greater than the potential for benefit. Antiemetics trimethobenzamide (Tigan) - less effective than other antiemetics and may cause EPS, drowsiness, diarrhea, and rash. Antihypertensives propanolol (Inderal), methyldopa (Aldomet), reserpine (Serpasil) - all have frequent CNS SE. but can be effective in some conditions. Therefore, these are not always contraindicated. If the pt is doing well on them, they may be continued, but with careful monitoring. Conclusion: Physicians prescribe potentially inappropriate medications for nearly a quarter of all older people living in the community, placing them at risk of drug adverse effects such as cognitive impairment and sedation. III. ADVERSE DRUG EFFECTS Incidence of serious (6.7%) and fatal (0.32%) Adverse Drug Reactions is extremely high. There is a problem with reporting as not everyone uses the same definition. Adverse drug reaction [WHO definition] = Any noxious, unintended, and undesired effect of a drug, which occurs at doses used in humans for prophylaxis, diagnosis, or therapy. This definition excludes therapeutic failures, intentional and accidental poisoning (ie an overdose), and drug abuse. This definition does not include adverse reactions due to errors in drug administration or noncompliance. Adverse drug events = any injury resulting from administration of a drug. This definition includes preventable events. Contraindications = Factors predisposing pts to predictable and serious adverse drug responses. (Can be absolute or relative) A. Basis for Adverse Effects 1. R/t patient factors - see previous discussion 2. Iatrogenic Factors r/t med errors and/or polypharmacy. 3. Pharmacologic Factors - increased or diminished effect. What is therapeutic effect [desired action] and side effect may be a matter of intent. B. Adverse Effects from Single Drug 1. Allergy: an immune response involving antigen-antibody reaction. Usually requires previous exposure; such is not always obvious; could be environmental to related chemical 2. Idiosyncratic reaction: Highly unusual and unpredictable. (Genetically determined) 3. Cumulative Effects: Increasing response to repeated doses of a drug that occurs when the rate of administration exceeds the
4. 5. 6. 7. 8. 9. 10.
12 rate of metabolism or excretion. As blood level rises, toxicity may occur. Toxicity: poisoning. May or may not be reversible. Tolerance: an increased dose of a drug is needed to cause a response equal to the response produced by a lower dose before tolerance developed. Usually occurs after prolonged administration. If it occurs after only one or two doses is called tachyphylaxis. Most common with CNS drugs. *Tolerance can develop to side effects and not therapeutic effect. Dependence: the need for continued administration of drug to prevent the appearance of a withdrawal syndrome. Can be physical (body adapts to the point where it cannot function without the drug) or psychological (more than a habit - a compulsion) Tissue damage - local or systemic. ie: gastric irritation from ASA. ototoxicity Carcinogenesis - from tobacco, asbestos etc. Teratogenesis - production of physical defects in the fetus. Mutagenesis - production of chromosomal abnormalities the manifest in offspring. Drug Fever a febrile response that coincides temporally with the administration of a drug and disappears after discontinuation of the offending agent. Very often misdiagnosed and underreported (approximately 3-5 % of AEs). In non-sensitized individuals receiving a drug for the first time, the onset of fever is highly variable and differs among drug classes, but most commonly appears after 710 days of drug administration and rapidly reverses after discontinuation of the drug.
Pregnancy Drug Categories Category A Adequate and well-controlled studies indicate no risk to the fetus in the first trimester of pregnancy and there is no evidence of risk in later trimesters. Animal reproduction studies indicate no risk to the fetus and there are no adequate, or well-controlled studies in pregnant women. OR Animal studies show adverse effect, but adequate & well-controlled studies in pregnant women have not demonstrated risk in any trimester. Animal reproduction studies have reported adverse effects on the fetus; and there are no adequate and wellcontrolled studies in humans, OR No animal studies have been done and there are no adequate and well-controlled studies in pregnant women. Positive human fetal risk has been reported in data from investigational or marketing experience, or human studies. However, potential benefit may, in selected cases, warrant the use of these drugs in pregnant women, if safer drugs are not available or are ineffective. Fetal abnormalities reported and positive evidence of fetal risk in humans is available from animal and/or human studies. The risks involved clearly outweigh the potential benefits. These drugs should not be used in pregnant women.
Category B
Category C
Category D
Category X
13
C. Adverse Effects From More than One Drug - Drug Interactions 1. Addition: when 2 drugs with the same mechanism of action are taken and the result is equal to the effects of either drug given alone in higher doses. [1+1=2]. eg. Tylenol 325 and codeine 30 given together as Cod #3. 2. Synergy: Two drugs have a greater combined effect than the sum of the separate action of each single drug [1+1=3] eg. ETOH and CNS depressants 3. Antagonism: combination of drugs produces less effect than that produced when either drug is given alone [2+2=1] eg. levodopa and B6 4. Alterations in absorption - one drug can change rate or extent of absorption of the other. If extent is changed - don't give together. 5. Alterations in distribution - changes in protein binding - eg Coumadin and ASA 6. Alterations in metab and excretion - barbiturates stimulate hepatic enzymes which increases metabolism and excretion of other drugs causing decreased therapeutic effects. If excretion alone is changed the alteration can lead to toxicity. D. Drug & Other Interactions 1. Lab tests Many drugs interact with diagnostics. ie: Fe --> false positive guiacs. Many drugs interfere with urine sugar tests. 2. Herbals see book 3. Food - again many possibilities. ie: minerals impairing absorption of fat soluble vitamins, Coumadin & green veggies, etc. 4. Grapefruit juice - can keep some drugs in the circulation longer by preventing them from being fully metabolized. Works by inhibiting enzyme Cytochrome P3A4 a CYP enzyme that breaks down drugs in the liver. The effect of grapefruit juice in the gut is long acting (up to 3 days) - so separating the timing of taking the drug and drinking the juice or even eating grapefruit will NOT be helpful. Affected drugs: Ca channel blockers (nifedipine, nimodipine, etc.) Sedatives (Halcion, versed, etc) Antihistamines (Seldane) Cyclosporine
14 Estrogen Lovastatin, etc. Midazolam, triazolam Etc. 5. Smoking causes decreased level of many drugs by stimulating enzymes which cause metabolism or excretion. ie: estrogens, vitamins, theophylline, flu vaccine, etc, etc.
ENDOCRINE DRUGS
DRUGS USED FOR PATIENTS WITH DIABETES MELLITUS I. INSULIN 1. Action: Same as physiologic insulin - facilitates the uptake and metabolism of glucose by insulin-dependent cells. Broken down by GI tract so cannot be given PO. Must be SQ. Regular insulin can also be given IV or infused directly into the peritoneal cavity. ACTION Rapid Rapid Rapid Short** Intermediate Long* Very Long* NAME Lispro [Humalog] Aspart [Novolog] Glulisine [Apidra] Regular NPH Detemir [Levemir Glargine [Lantus] ONSET 5 - 15 minutes 10-20 minutes 5 30 minutes 2-1 1-2 Gradual 1 hrs PEAK 1 1 hr 1 3 hrs 1 hr 2-4 6 - 14 6 8 hrs No peak DURATION 3 - 4 hrs 3 5 hrs 3 4 hrs 6 10 hrs 16-24 hrs Up to 24 hrs. 24 hrs
*Do not mix with any other insulin. ** Only type that can be given IV. Note: hypoglycemic episodes are most likely to occur at the time when the insulin peaks. A. available in: 1. U100 2. U500 [prescription needed] - for pts with insulin resistance *U100 = 100units/mL Rapid Acting: Because of rapid onset and peak, it more closely mimics the dynamics of plasma insulin response to a meal in non-diabetics. Thus, pt can take shot 5-10 minutes before eating (or when beginning to eat), instead of 30 minutes. Pt must eat promptly after injection [within 15 minutes] to avoid hypoglycemia. Should not use if have delayed or inconsistent gastric absorption because could hypoglycemia. B. Always use insulin syringe - no dead space. Regular syringes may trap as much as 10 u. C. Storage: 1. store open vials at controlled room temp 59-85F Good for about a month. 2. store extra vials in fridge. Do not freeze or heat. D. Absorption: 1. Most rapid and predictable absorption takes place in: a) abdomen 50% of dose in 87 minutes b) arms 141 minutes c) thighs 164 minutes d) buttocks 155 minutes
15 ADA recommends rotate sites within one anatomic region to lipodystrophy and variation in daily absorption. (only in piggy insulin) 2. Vigorous massage and exercise faster absorption. Take into account type of exercise pt plans to do after injection. Generalized heat & injecting more deeply faster absorption. 3. Blood Glucose Concentration - higher BG concentration = delay in peak and extended duration of regular insulin E. Types: Human insulin v. Pork insulin a) Advantages - purer, non-allergenic. Has faster & shorter action, so dose adjustment may be needed. F. Insulin Adjustment 1. Increased need: Body growth Hormonal changes [eg pregnancy] Increased food intake Stress Illness ** SMOKING DRASTICALLY IMPAIRS INSULIN ABSORPTION DUE TO VASOCONSTRICTION** 2. Decreased need: exercise decreased food intake some disease states [eg end stage renal disease] 3. Must adjust dose when traveling through time zones. Going EAST - decrease dose by fraction of the time you lose Going WEST - increase by fraction of time you gain G. Side Effects 1. Allergic Responses a) local - burning, stinging, itching, erythema b) systemic - urticaria 2. Insulin resistance develops IgG mediated antibodies to insulin. Pt needs high doses [>100u/day] RX: complex - may need special insulins 3. Lipodystrophy a) Atrophy b) Hypertrophy H. Drug/drug Interactions: 1. Drugs which cause hyperglycemia [need more insulin]: steroids oral contraceptives thyroid preparations 2. Drugs which cause hypoglycemia [need less insulin] ETOH anabolic steroids MAOI beta blockers theophylline salicylates 3. Many OTC drugs contain sugars or agents which may increase BS. I. Mixing 1. Withdraw short acting first. 2. Most solutions are stable. Can be stored in fridge for up to 3 months. Unrefrigerated solutions can be stored for up to a month under ideal conditions. Store mixed insulins with needle up to prevent clogging. 3. Regular insulin is compatible with all other insulins. 4. Mixed insulins equilibrate with time. The shorter acting insulin binds with the longer acting causing a different speed of action. Teach pt to give all mixed doses within the same time frame. Either always within 15 min or always longer than 15 min. **An exception is Regular/NPH mix - binds within 15 minutes (binding is not clinically significant). J. Administration
16 1. Do not aspirate 2. Pt may reuse syringes. 3. No need to use alcohol swabs (wtf, bs?) 4. Do not use if insulin is "frosted" Frosting indicates loss of potency. 5. Do not shake - excess agitation causes frosting 6. Rotate sites Noninsulin Polypeptide Analogues 1. *Pramlintide [Symlin] - comes in vials or injector pen a. Synthetic analogue of Amylin hormone released by pancreas after eating. Released along with insulin and is synergistic to insulin. Slows gastric emptying, suppresses release of glucagon, suppresses appetite because increases feeling of satiety. b. By injection only. c. Can be used for both type 1 & 2. But only for pts taking insulin. d. Given: Subcutaneous just before each meal. Use insulin syringes. Do NOT mix with insulin. Give in a different site. Usually reduce insulin dose at first. e. Can cause severe hypoglycemia - may happen within 3 hours of dose. (does not happen with Symlin alone, but with insulin it does). Other side effects include: N/V, HA, allergy, joint pain, cough. II. ORAL HYPOGLYCEMICS Primary failure = The patient does not respond to therapy. Occurs in 20% of pts. Not known why. Secondary failure = The patient responds for a time, then, for reasons not known, no longer responds. Occurs in 5-10%. About half of pts with secondary failure will respond to another drug. Sulfonylureas: A. Action: Stimulates the pancreas to produce more insulin. Increases sensitivity to insulin at the receptor. May increase the # of receptor sites for insulin & may potentiate insulin action on post-receptor phase. After a few months, insulin secretion levels drop to pretreatment levels, but blood sugar stays down (not permanent effect). B. Contraindications: 1. Allergy to sulfonamides 2. NPO patients 3. Pregnant or breast feeding patients 4. Impaired Hepatic or Renal function. C. Side Effects: Hypoglycemia may be long lasting. N/V, fullness, epigastric distress. Rash, photosensitivity. Agranulocytosis, hemolytic anemia, thrombocytopenia, cholestatic jaundice. C. Drugs: 1. *Chlorpropamide [Diabenase] - first generation not widely used anymore 2. Glyburide [Micronase; Diabeta] second generation 3. Glipizide [Glucotrol] second generation *Glimepiride [Amaryl] For Type II DM patients. Usually indicated as an adjunct to diet and exercise . Also, can be given in combination with insulin for patients whose hyperglycemia cant be controlled by diet, exercise, and oral meds. Advantages of second generation: More potent so need smaller doses Can be given once a day Fewer drug interactions D. Many drug/drug interactions are associated with Sulfonylureas of both generations. Diabenase + ETOH flushing, HA, light-headedness & wheezing, N/V. Taking an Aspirin one hour before alcohol use can slow the reaction. Cautioned use in patients with asthma. Biguanides: *Metformin [Glucophage] Action: Reduces glucose production by the liver and absorption in the intestine. Enhances uptake of use of glucose by peripheral tissues (helps tissues utilize insulin). Reduces glucose production in the liver, thus lowering demand for insulin. It does NOT stimulate insulin release mechanism of action is independent of insulin release. Indications: For use in pts with type 2 who cant manage BS with diet and exercise alone (with or without use of sulfonylureas).
17 Works particularly well in obese pts. Can promote weight loss. Side Effects: N/V/D/A, bloating, unpleasant or metallic taste. Uncoated pills have a smell of fish or dirty socks: hence nausea. Metformin does not cause hypoglycemia *Lactic acidosis - can result in death. Early symptoms of lactic acidosis: extreme weakness, fatigue, discomfort, myalgia, stomach discomfort, dizziness or lightheadedness, sudden slow or irregular pulse. Teach the patient to STOP drug and call MD. Lactic acidosis requires emergency treatment. Hemodialysis can help remove the drug. ETOH use increases risk for lactic acidosis. Contraindications: Renal disease or dysfunction. HF. Acute or chronic metabolic acidosis including diabetic ketoacidosis. Other: Taken BID [breakfast & dinner]. life is about 6 hrs. Meglitinides: Basic action of Meglitinides is stimulation of insulin release. 1. Repaglinide [Prandin] Action: Seems to preserve glucose-stimulated proinsulin (insulin precursor) biosynthesis in islet cells. Binds to beta cells. Stimulates insulin secretion via inhibition of potassium channels in beta cells. Very fast acting and quickly eliminated. life = less than 1 hr. life of glucose is very brief. Administered before meals. Optimal timing is 15 minutes ac, but can be taken anywhere between immediately before meals to 30 minutes before meals. *Skip the dose if patient misses a meal; add a dose if patient adds a meal. Eliminated mostly in feces. Useful for pts with renal disease (does not use renal elimination). 2. Nateglinide [Starlix] Dose: given TID (3x daily), 1-30 minutes ac. Allows for mealtime flexibility. Rapid and short-acting. Pt can skip pill if meal is missed. Nateglinide is excreted by kidney so caution with renal disease. Side effects of Meglitinides: Hypoglycemia is most common SE, but does not occur often. Also: joint pain, upper respiratory infections, and paresthesias. Thiazolidinediones (TZDs) Glitazones Indicated for Type II DM, who have to take insulin, but still have inadequately controlled blood sugar levels. May reduce or eliminate dependence on insulin. Action: Reverses insulin resistance at the cellular level by agonizing the receptors that regulate insulin uptake (improving the bodys ability to utilize insulin). Also decreases hepatic glucose output. Takes 3-4 months to get full effect. Excretion: via bile and kidney SE: infection, muscle pain, HA, edema, weight gain, increases in cholesterol. Potential hepatotoxicity, Can cause or worsen HF, Can increase the risk of fractures in women Thiazolidinedione Drugs: Pioglitazone [Actos] HF & MI Black Box warning Actos may cause resumption of ovulation in anovulatory pts (pre-menopausal) Rosiglitazone [Avandia] HF & MI Black Box warning Controversial medication, recent research has indicated higher risk of CV problems. Removed from market in Europe. Nursing Considerations: Can be taken without regard to meals. Liver function needs to be monitored. Monitor for signs of CV effects. -Glucosidase Inhibitors Action: competitive, reversible inhibition of pancreatic alpha-amylase, an enzyme which hydrolyzes complex carbohydrates to oligosaccharides. By inhibiting this enzyme, acarbose (drug) delays digestion of starches. This results in a smaller rise in blood glucose concentrations following meals. Acarbose also inhibits the metabolism of sucrose to glucose and fructose. Caution: With this drug, complex oral sugars wont reverse hypoglycemia when pt is taking acarbose! Must use IV sucrose/dextrose, or PO glucose! Side Effects: GI Symptoms: Intestinal gas, abdominal pain, distension, diarrhea, borborygmi.
18 *These GI symptoms usually decrease over time. GI symptoms will get worse if pt does not eat correct diet. Also can get elevated liver enzymes. Dose: Taken TID - with first bite of each main meal. Omit dose if pt misses a meal. A-Glucosidase Inhibitors: Acarbose [Precose] Pregnancy Category B Miglitol [Glyset] Incretin Therapy Incretins are hormones released by the small intestine upon food consumption. There are (2) major incretins: Gastric inhibitory peptide [GIP] and Glucagon-like peptide [GLP-1]. Effects of Incretins: 1. Increase insulin secretion 2. Decrease glucagon secretion 3. Delay gastric emptying 4. Increase feeling of satiety Incretin therapy works well in lowering blood glucose levels and have few side effects. They do not cause hypoglycemia when used alone. Incretin Mimetic: Exenatide [Byetta] a. Action: GLP-1 receptor agonist. b. Used only for Type II DM patients whose insulin levels are not controlled with other meds. c. Given SQ BID (2x daily) within one hour before breakfast and dinner. d. Comes in a pen e. Can cause hypoglycemia when used with sulfonylureas, NOT when used alone. Other side Effects: N/V, allergy, HA, dyspepsia, GERD, restlessness, and jittery feeling. f. Has been implicated in acute pancreatitis & kidney failure Liraglutide [Victoza] a. Action: GLP-1 receptor agonist b. Injection once a day c. Reduces HbA1C levels. d. Low risk of hypoglycemia e. Aids in weight loss f. Rat studies indicate possible link with thyroid C cell tumors, but these types of cancer occur so infrequently in people that a human study is impossible. DPP-4 Inhibitors aka Incretin enhancers Action: Prevents breakdown of incretins by inhibiting the enzyme that breaks them down and thus increase amount of insulin released after meals. Very small hypoglycemia risk because they work only in the presence high serum glucose levels (when used alone). Sitagliptin [Januvia] (Janumet fixed combination of Januvia and Metformin) a. PO. Once daily. b. Works only when BS is elevated. c. Increases satiety d. SE: HA, diarrhea, nasophyryngitis. e. Interactions: cocoa and rosemary may decrease therapeutic effect. Saxagliptin [Onglyza] a. SE: URI, UTI, HA, allergic-like reactions such as rash and hives Selective sodium-glucose cotransporter inhibitors (drug is still in development) Action: prevents reabsorption of glucose in the kidneys and promotes excretion of glucose in the urine. Thus reducing blood sugar. Works in a non-insulin dependent manner. Dapagliflozin is the SGLT2 inhibitor with the most clinical data available to date, with other SGLT2 inhibitors currently in the developmental pipeline. Dapagliflozin has demonstrated sustained, dose-dependent glucosuria over 24 hours with once-daily dosing in clinical trials. SE: increased risk of UTI and genital infections (r/t excess sugar in the urine). III. Glucagon 1. Action: increases BS through glycogenolysis and gluconeogenesis Except during meals and extended fasting, glucagon is responsible for hepatic glucose production. Glucagon also
19 increases the breakdown of protein and fat, which provides additional fuel for cellular metabolism. 2. Given SQ, IM, or IV. Cannot be taken PO. 3. Interactions: increases oral anticoagulant effects. Inhibited by beta blockers which can also increase heart and BP effects. 4. *Glucagon is NOT effective in poorly nourished or starving pts. If pt has no glycogen stored in the liver, glycogenolysis cannot occur even with glucagon. 5. SE: Nausea and vomiting (rare). Hyperglycemia. Temporary (or) BP.
DRUGS USED FOR PATIENTS WITH THYROID DISORDERS
I. THYROID AGENTS 1. Action of thyroid agents are the same as natural hormones: Increased metabolic rate, stimulates heart function and increases CO. Increased: body temp, blood volume, growth, and overall cellular growth. Increased oxygen consumption. [Thyroid agents may also increase the hearts sensitivity to catecholamines and increase the number of beta receptors in the heart] 2. Uses: Replacement therapy 3. SE: (symptoms of hyperthyroidism): cardiac dysrhythmias; palpitations, diaphoresis, tachycardia, etc. 4. Interactions: Increased effect of Coumadin, etc. Increased BG, so DM pts may need more insulin. 5. Drugs: Synthroid [levothyroxine or T4] - first choice drug. Cytomel [liothyronine or T3] - Rapid onset and short duration of action makes it the choice drug for rapid effect. Thyrolar [Liotrix] T3 and T4 6. Nursing considerations: Caution use in patients who are elderly or have a history of heart disease. Thyroid Agents may aggravate angina and lead to MI. Do not stop abruptly! Can result in myxedema coma. Watch for signs of hyperthyroidism [overdose] : fatigue, breathlessness, heat intolerance, HA, palpitations, nervousness II. Antithyroid drugs: Action: inhibits hormone production by reducing the combination of iodide and tyrosine, and the coupling of MIT and DIT. Also has immunosuppressant effects. Iodine acts by overloading the thyroid with iodine to stop the production of thyroid hormone. However, this effect is only temporary [a few days]. Indications: treatment for Graves disease (hyperthyroidism) (may cause remission). Also used preop to achieve euthyroid state. Side Effects: Liver and Bone marrow toxicity. Potentially fatal granulocytopenia [usually appears after 4-8 weeks of treatment. Early sign is a sore throat or fever.] Allergy [usually during first 3 weeks] HA, vertigo, neuritis, paresthesias. Brassy taste and burning sensation in mouth, increased salivation. Potassium Iodide (SSKI) can discolor teeth Drugs: PTU [propylthiouracil] Does not affect any thyroid hormone already present in the body. Only prevents new formation, so response may take several weeks. Contraindicated in pregnancy. Tapazole [methimazole] - Contraindicated in third trimester of pregnancy. Potassium Iodide [Lugols solution, SSKI] - Used to prepare the thyroid gland for surgery by reducing thyroid vascularity. Also used for prophylaxis of radiation exposure to protect the thyroid (taken before or within 3 hours of exposure). Radioactive iodine - To destroy part of the thyroid gland. Nursing considerations: Check WBC Assess for symptoms of hypothyroidism: depression, cold intolerance, non-pitting edema, etc. Other Steroids Corticosteroids:
20 Effects of corticosteroids: 1. Anti-inflammatory 2. Suppression of the immune response 3. Suppression of the allergic response 4. Reduction in cell reproduction Route: Corticosteroids are well absorbed PO, but also can be given by many different routes. Other routes besides PO and IV limit systemic absorption, but can be useful in certain situations. Corticosteroids are highly plasma bound. Also, crosses placenta and breast milk. Adverse effects of corticosteroids when taken long term: 1. **Cushings syndrome** which harbors the same adverse effects as chronic corticosteroid treatment. Symptoms: adrenal atrophy, osteoporosis, HTN, increased susceptibility to infection, delayed wound healing, acne, peptic ulcers, obesity, moon face, buffalo hump, behavioral changes, etc 2. Cataracts and glaucoma 3. Metabolic changes a. High serum glucose (BG) b. Electrolyte imbalances i. Hypocalcemia (Ca++) ii. Hypokalemia (K+) iii. Hypernatremia (Na+) c. Fluid retention d. Weight gain e. Hypertension f. Edema 4. Corticosteroids can mask signs of infection! Mineralocorticoids: Fludrocortisone: Action: Same action as aldosterone. Promotes Na+ and water reabsorption and K+ excretion. Uses: Treat Addisons disease and salt-losing adrenogenital syndrome. SE: Fluid retention, edema, HTN, HF, symptoms of hypokalemia.
ACE INHIBITORS
Outcomes for patients with HF are improved greatly in combination therapy of ACE Inhibitors, digoxin, and diuretics. Action: ACE inhibitors interfere with the renin-angiotensin-aldosterone system, by inhibiting the enzyme ACE that converts Angiotensin I to Angiotensin II. This inhibits aldosterone release by the adrenal cortex, preventing sodium and water retention. Also reduces peripheral arterial resistance without affecting the heart rate and CO. Result is BP reduction. *ACE inhibitors prevent Na+ and water reabsorption in the kidney, but K+ is reabsorbed in higher than normal amounts, so K+ levels need to be monitored. *ACE inhibitors prevent breakdown of bradykinin (a vasodilating substance) which results in vasodilation, decreased afterload, and decreased BP. Indications: Hypertension, HF, Acute MI, and for patients at high risk for CV events. Diabetic nephropathy and other kidney diseases ACE Inhibitors are the drug of choice for HF patients with high BP.
Side Effects: HA, dry nonproductive cough, rash, pruritus first dose hypotension, dizziness, fatigue, syncope Dysgeusia (change in taste), mood changes Anemia, neutropenia, thrombocytosis, agranulocytosis Hyperkalemia, transient elevations of kidney function tests
21 Angioedema: If drug is not stopped when angioedema develops, the patient is at increased risk of further episodes with serious morbidity [intubation]. Risk of angioedema is 5X higher in blacks than whites. Visceral Angioedema (rare): localized edema and capillary permeability in the gut pain, N/V, diarrhea. Interactions: NSAIDS, diuretics, and other antihypertensives. Drugs: Captopril [Capoten] - Short half-life, so good for titrating an acutely ill patient. Give captopril on empty stomach. Enalapril [Vasotec] - PO, IV Prodrug. Ramipril [Altace] Effective. Also reduced the new development of DM by 30%, the first drug to be effective in this role. Fosinopril [Monopril] Lisinopril [Zestril] Benazepril [Lotensin] Nursing considerations: Get baseline pulse and BP prior to administration. Monitor for hypotension during administration. monitor liver function, renal function, and potassium levels every month for the first three months of administration. If angioedema occurs: Stop administering the drug and call the MD. The patient may need emergency treatment.
DIURETICS
DIURETICS Loop Diuretics (The most potent of all diuretics) Action: Inhibits Na+ and Cl- reabsorption in the renal tubules by direct action on the ascending Loop of Henle. Also inhibits Na+, Cl-, and water reabsorption in the proximal tubule. Increases the concentrations of renal prostaglandins to increase dilation of blood vessels in the kidneys and lungs. Indications: Edema associated with HF, liver, and kidney disease. Hypertension. Hypercalcemia. Side Effects: Volume depletion [especially in elderly], orthostatic hypotension, electrolyte disturbances, impaired glucose tolerance, blood dyscracias, Steven-Johnson syndrome. Tinnitus, transient deafness. Neurotoxic and nephrotoxic effects. Interactions: Additive neurotoxic and nephrotoxic effects Increases serum uric acid, glucose, and AST and ALT levels. Digoxin NSAIDs interact with loop diuretics and cause less diuresis Drugs: Furosemide [Lasix] - Related to sulfa drugs. PO or IV. Diuresis causes loss of magnesium and calcium. Bumetanide [bumex] Ethacrynate [Edecrin] Can cause irreversible ototoxicity Torsemide [Demadex] Nursing considerations: Give IV slowly, over four minutes. *Fast administration can cause transient tinnitus or deafness. Store in light resistant containers Potassium supplements are often needed due to losses. Thiazides Action: sulfonamide drugs that inhibit tubular reabsorption of Na+ and Cl- ions in the loop of Henle and distal tubule. Thus, water, Na+, and Cl- are excreted. Potassium is also excreted. Also may increase GFR. Initially, the decrease in blood volume decreases CO, but this eventually stabilizes. These drugs are most effective after 3-4 weeks of treatment. Indications: Hypertension, edema, hypercalciuria, diabetes insipidus, HF, and cirrhosis. Side Effects: orthostatic hypotension, hyponatremia, hypokalemia, glucose intolerance, GI, rash, HA, impotence, deceased libido. Interactions: Digoxin: can promote digoxin toxicity. Oral hypoglycemics: reduces effects of oral hypoglycemics. Monitor BG. Bile acid sequestrants: separate administration of these two classes
22 Drugs: Hydrochlorothiazide [HCTZ, Hydro-Diuiril, Esidrix] Exhibits a diuretic ceiling effect at approximately 50 mg. Chlorothiazide [Diuril] Chlorthalidone [Hygroton] Indapamide [Lozol] Nursing considerations: Check K+ and assess for symptoms of hypokalemia Give K+ supplements as needed Check blood glucose Weigh daily Orthostatic hypotension patient teaching Administer in the morning *Check for sulfonamide allergy Potassium sparing Diuretics Na+ ion channel inhibitors Action: Directly acts on distal renal tubules to inhibit Na+ reabsorption in order to promote excretion of Na+ and water, and retention of K+ Drugs: Amiloride [Midamor] - Usually used with loop or thiazide diuretics for CHF. Triamterene [Dyrenium] Aldosterone Antagonists (also potassium sparing) Action: Prevents aldosterone from binding with receptors. Drugs: Spironolactone [Aldactone] - used for ascites. *Also, used for kids with CHF. Eplerenone [Inspra]
Overall Mechanism of Action (Aldosterone Antagonists): Work in collecting ducts and distal convoluted tubules Interfere with sodium-potassium exchange Competitively bind to aldosterone receptors Block the reabsorption of sodium and water usually induced by aldosterone Potassium Sparing Diuretics (General) Indications: Hypertension. Often used in conjunction with other diuretics to prevent K+ loss. Side Effects: Hyperkalemia, anemia, dizziness, orthostatic hypotension, sore throat, dry mouth, N/V, kidney stones, impotence, irregular menses, hirsutism Interactions: Increased Lithium toxicity ACE inhibitors and K+ supplements can cause hyperkalemia Licorice Nursing considerations: Check for symptoms of hyperkalemia Give with food or milk to ease GI stuff Osmotic Diuretics Action: Increases the osmolality of the plasma, glomerular filtrate, and tubular fluid. Pulls fluid from extravascular spaces into vascular and then to tubules. Osmotic diuretics are inert and resistant to extensive metabolism. Effects: a. reduced cellular edema b. increased urine production c. rapid excretion of water, Na+, other electrolytes, and toxic substances d. reduces intraocular pressure
23 Indications: increased ICP, cerebral edema, acute renal failure, and to reduce toxins at toxic levels in the blood. Side Effects: convulsions, thrombophlebitis, pulmonary congestion, chest pains, tachycardia, HA, blurred vision, chills, fever, rhinitis Interactions: none Drugs: Mannitol [Osmitrol] - IV (only) Glycerin - PO Urea [Ureaphil] Nursing considerations: Check urine output hourly Crystallizes at low temperatures. Dissolve by warming in hot-water bath and shake until room temperature. Rate of IV administration is very important (can cause severe shifts in F/E balance if given too quickly) Carbonic anhydrase inhibitors (also a sulfonamide) Action: Inhibits carbonic anhydrase an enzyme needed in sodium reabsorption (enzyme allows Na+ and H+ binding) . With inhibition of carbonic anhydrase and less hydrogen available for exchange, there is increased excretion of Na, water, K+, and bicarbonate. Works in proximal tubule Decreases formation of aqueous humor (eye fluid) **Carbonic anhydrase inhibitors are less potent than loops or thiazides, and are only effective for 2-4 days. Indications: *Glaucoma, *pre-op eye surgery, edema, epilepsy (absence seizures), high-altitude sickness, and also for excretion of drugs (produces alkaline urine which can help excrete acidic drugs) Diamox is used for edema from HF if other diuretics are not effective. Side Effects: Metabolic acidosis, photosensitivity, paresthesia, urticaria, drowsiness, anorexia, hematuria, melena. Interactions: Digoxin toxicity due to hypokalemia Drugs: Acetazolamide [Diamox] - PO, IV Methazolamide [Neptazane] Mainly for glaucoma
ANTI VIRALS
ANTIVIRAL AGENTS A. Action: Antivirals work by interfering with viral replication. DRUGS FOR NON HIV VIRUSES B. Drugs 1. Acyclovir [Zovirax] - used for herpes simplex I & II, varicella-zoster, and herpes zoster. Action: Nucleoside Analog mimics one of the substances needed for viral DNA replication. Virus thus cannot reproduce. Effect: Decreases the duration & severity of HSV attacks. (not a prophylactic) Route: PO or IV, topical SE: Local tissue irritation and damage, HA, N/V/D. May cause reversible renal impairment with IV route. 2. Gancyclovir [Cytovene] Treatment for CMV (cytomegalovirus) retinitis 3. Valacyclovir [Valtrex] herpes etc. 4. Docosanol [Abreva] OTC topical medication for cold sores. Topical with no systemic absorption. 5. Cidofovir [Vistide] Used for treatment of CMV retinitis in AIDS patients. 6. Famciclovir [Famvir] genital herpes and shingles. 7. Foscarnet [Foscavir] IV CMV & herpes C. Drug interactions several - including cytotoxic agents. E. Interventions: watch for therapeutic and adverse effects. Gancyclovir: Advise the patient of childbearing age to use contraception during and for at least 3 months after treatment because it may cause fetal mutations. Also, dont breast feed while on it.
24 ANTI-VIRALS FOR FLU 1. Amantadine [Symmetrel] - Used for influenza A virus in high risk groups. Must be given before attack or within 48 hrs. Can be given with flu shot to protect pt while immunity is developing. (also used for Parkinson's disease - antidyskinetic) a. Antiviral action: May prevent uncoating of virus and thus inhibit replication b. Anti-parkinsons action: releases dopamine and norepi from storage site. c. Adverse effects: Nausea, nervousness, depression, anxiety, insomnia, fatigue, problems concentrating. Previous psych or abuse disorders can become worse. Seizures in pts with disorder. 2.Rimantadine [Flumadine] a. like symmetrel. b. SE: NV, abd pain. 3.Zanamivir [Relenza] selective neuraminidase inhibitor Action: inhibits viral surface enzyme (neuraminidase aka sialidase) thus inhibiting viral replication. Effect: reduces time to symptom relief by about 1-2 days. Route: Inhalant use BID for 5 days. Need to start treatment within two days of onset of symptoms. SE: very few. 4.Oseltamivir [Tamiflu] Neuraminidase inhibitor Effect: Reduces time to symptom relief by about 1.3 days. Route: PO. Taken within 2 days of symptom onset. Taken BID x 5 days. SE: N/V Drugs used as part of HAART A. Nucleoside Reverse transcriptase inhibitors (aka NRTIs). Also, Nucleotide Reverse Transcriptase Inhibitors (NtRTIs) a. Reverse transcriptase is an enzyme the virus requires for DNA synthesis which is not found in human cells. b. The drug mimics the nucleoside effectively inhibiting replication. c. One of the classes always used in HAART d. These are prodrugs e. General SE: i. NVD, HA, and fatigue during the first few weeks. ii. Toxic to mitochondria (Mitochondrial toxicity) inhibits gamma-polymerase needed for DNA in mitochondria which can cause lactic acidosis & severe hepatomegaly with steatosis syndrome. 1. More common in women and with liver damage to start with. Syndrome can cause increased liver enzymes, fatty liver, and possible liver failure. 2. Symptoms: nausea, myalgia, and RUQ pain. iii. Mitochondrial toxicity also causes lipodystrophy. In lipodystrophy, the face, arms, and legs lose fat and increased amounts of fat are deposited on the abdomen, breasts, and base of neck (buffalo hump). f. NRTI Drugs: 1. Zidovudine [AZT, Retrovir] - For AIDS. Helps control opportunistic infections like PCP. Current dosing is q12h Interactions: many! Including: ASA and Tylenol Adverse Effects: N/V/D/A, dyspepsia, changes in taste, headache, dizziness, fever, rash, listlessness (loss of interest and vigor), myalgia, skin rashes, agitation, restlessness, insomnia, , diaphoresis, dyspnea. Potential nephrotoxicity. Can cause granulocytopenia, and anemia. Interventions: Take ATC. Does not reduce risk of passing virus to others. Dont use OTC drugs before checking with HCP first. Resistance develops in 3-6 mo if used alone. abacavir [Ziagen] emtricitabine [Emtriva] lamivudine [Epivir] stavudine [Zerit] tenofovir [Viread]
2. 3. 4. 5. 6.
B. NonNucleoside Reverse Transcriptase inhibitors [NNRTIs] a. Inhibit reverse transcriptase by binding close to it and changing its shape (does NOT mimic the enzyme). b. SE: Rash (can be Steven Johnson but rarely); can affect liver.
c.
25 Drugs: 1. Efavirenz [Sustiva] i. Once daily dosage ii. High fat meals can increase absorption by up to 50% which can lead to toxicity. take on empty stomach iii. Side effects at the beginning of treatment: sleep disorders, nightmares, dizziness, decreased ability to concentrate, delusions. These slowly go away in about a month. Approximately of pts experience these. iv. Teratogenic 2. Delavirdine [Rescriptor] 3. Nevirapine [Viramune] 4. Etravirine [Intelence]
C. Protease inhibitors Drug works by inhibiting protease. Introduced in 1995 and revolutionized HIV treatment. a. General SE: GI stuff. Lipodystrophy, cholesterol, maybe hyperglycemia and diabetes. b. Kaletra [Lopinavir and Ritonavir in combination therapy] i. Approved in 2000. ii. Ritonavir inhibits the breakdown of Lopinavir so much more is available. Much higher blood levels! iii. PO, Take once or twice daily iv. *Drug of choice for first line treatment v. Interacts with St. Johns wort which decreases antiviral levels. c. Saquinavir [Invirase] Approved by FDA in only 97 days! Should be used in conjunction with AZT, etc. d. Nelfinavir [Viracept] SE: Severe diarrhea (most common), nausea, flatulence, rash, anemia, leukopenia. Interactions: decreased oral contraceptive effectiveness. e. Ritonavir [Norvir] most likely to cause SE and toxicity problems. Used to boost blood levels of others inhibits CYP 450 so others stay at higher levels. SE: N/V/D/A, HA, fatigue, taste disturbances, circumoral paresthesia. Diarrhea often severe enough to noncompliance. f. Indinavir [Crixivan] - relatively safe and well tolerated. give with high fat foods to increase absorption. Most impt SE is nephrolithiasis. Pts must drink large amts of fluids throughout the day. If stones develop, tx with hydration and analgesics - do not stop indinavir. Q 8 hr dosing g. Atazanavir [Reyataz] less effect on lipid levels h. Darunavir [Prezista] i. Fosamprenavir [Lexiva] j. Tipranavir [Aptivus] D. Fusion Inhibitors a. Interferes with fusion of viral and cellular membranes which blocks the virus from getting into the host cell. 1. Enfuvirtide [Fuzeon] 2003 a. Given SC, BID b. Has no adverse effects on liver c. In the beginning of treatment, the patient will almost always experience injection site reactions: pain, pruritus, erythema, cysts, cellulitis. d. Other side effects: NVD and fatigue e. Increased risk of pneumonia E. Integrase inhibitors 2007 a. Without the enzyme integrase, HIV cant insert viral DNA into the human chromosome. 1. Raltegravir [Isentress] PO. a. HA, GI stuff F. CCR5 inhibitors a. CCR5 is a human cell receptor that HIV uses to enter the cell. Blocking entry into CCR5 reduces viral load. b. Maraviroc [Selzentry] PO i. SE: Abdominal pain, cough, dizziness, fever, rash, URI, musculoskeletal problems. Liver toxicity. Increased risk of MI.
26
ANTI-PARKINSONS DRUGS
DRUGS FOR PARKINSONS: Normally in the body there is a homeostatic balance of acetylcholine and dopamine. A decrease in dopamine causes a subsequent increase in acetylcholine. Decreasing elevated levels of acetylcholine back to normal levels can bring dopamine levels back up. Also, increasing dopamine levels causes acetylcholine levels to decrease. ANTICHOLINERGICS AKA cholinergic blocking agents, parasympatholytics, or antimuscarinics. (Have been used for >150 years) Action: Blocks the action of acetylcholine at the muscarinic receptors in the parasympathetic nervous system. Competitive antagonists which compete with acetylcholine at the muscarinic receptor site resulting in inhibition of nerve transmission. Therapeutic Effects: Mydriasis (pupillary dilation) and Cycloplegia (paralysis of ciliary muscle of the eye [loss of accommodation]) Decreased GI motility, decreased bladder contraction, decreased secretions, decreased bronchial secretions Increased HR Decreased sweating. Indications: Decrease muscle rigidity and tremors. Tx heart block and sinus bradycardia Tx bronchospasm Tx ulcers, IBD, and GI hypersecretory states Tx pancreatitis Also used to control EPS Can produce a little improvement in functional capacity. Usefulness is limited by the side effects associated with anticholinergics and they become less effective with continued use. Cautions: Elderly can respond to usual doses, but they get many side effects: agitation, sleepiness, altered thought processes, memory problems, paradoxical excitability, confusion, hallucinations. Anticholinergics precipitate glaucoma r/t mydriasis. Causes decreased GI motility and GU function so use cautiously in patients with GI disorders and those susceptible to urinary retention or BPH. Increased HR, so use carefully in patients with CV disease. Careful with COPD pts, can dry secretions and create mucus plugs. Administration: *Start with low doses and build up gradually. Also stop treatment the same way. Give before meals [30-60min] to maximize absorption. Do not give if antacids or antidiarrheal have been taken within 1 hour. Anticholinergic Drugs: 1. Benztropine [Cogentin] Suppresses tremors and rigidity. PO, IM, IV SE: drowsiness, confusion, constipation , N/V, blurred vision, mydriasis, photophobia, dry skin, urinary retention, decreased sweating. Anticholinergic Overdose symptoms: respiratory depression, circulatory collapse, shock, coma . (Antidote = Physostigmine) 2. Trihexyphenidyl [Artane] - same as Cogentin. In older males, may cause prostatic hyperplasia. DOPAMINE INCREASERS DRUGS THAT INCREASE BRAIN DOPAMINE LEVELS: 1. Levodopa [L-Dopa] Action: A small percentage of administered L-Dopa crosses blood-brain barrier intact. In the brain, the L-Dopa is decarboxylated to dopamine, replacing missing brain dopamine and balancing dopamine-acetylcholine concentrations. Usually takes 2-3 weeks to get effect (sometimes much longer). Side Effects: Anxiety, nervousness, confusion, nightmares, tremors and involuntary movements, insomnia Dystonias head bobbing, jerking movements
27 o requires lowering of dose Flushed skin, dark urine, or sweat. Depression, mood changes, increased aggressiveness, o Psychosis occurs in about 20% of pts on L-dopa Irregular heart beat, orthostatic hypotension Severe nausea and vomiting HA *Not recommended for kids, pregnant women, or patients with skin lesions or malignant melanoma. Interventions: Give before meals because food impedes drugs action. Orthostatic hypotension can be severe. Call MD if symptoms of L-Dopa OD occur: involuntary muscle twitching and winking. L-Dopa must be discontinued at least two weeks before giving any MAOIs. Must have 12 hours between levodopa dose and start of carbidopa-levodopa combo pill. Dietary counseling: Proteins may be metabolized into amino acids, which compete with levodopa for transport to the brain, making the response to levodopa unpredictable. Divide protein intake evenly throughout day. Vitamin compounds and foods high in pyridoxine such as: pork, beef, liver, bananas, ham, and egg yolks; may decrease the effects of L-Dopa and should be avoided. Take high fiber and high fluid intake to minimize SE of constipation. LevoDopa ON-OFF SYNDROME - Occurs after long term treatment (2 years or more). Patient fluctuates from being symptom free on to demonstrating full blown Parkinsons symptoms off during therapy. May last from a few minutes to hours and may be secondary to: a decrease in delivery of dopamine centrally, an alteration in sensitivity of the dopamine receptors, variation in amount and rate of drug absorption, a dopamine metabolite interference, or a combination of effects. Treatment: 1) Give L-Dopa more frequently 2) Add bromocriptine 3) Give a new drug apomorphine HCL [Apokyn] approved as an orphan drug to treat off syndrome. Wearing off effect Seen at end of duration as serum level may fall below therapeutic levels. Tx: more frequent dosing. 2. Levodopa-carbidopa [Sinemet]: a. Carbidopa is a decarboxylase inhibitor. It competes with the enzyme dopa decarboxylase, thus retarding the peripheral breakdown of L-dopa (thus, minimizing SE like N/V). b. Carbidopa does not cross blood-brain barrier and does not interfere with the intracerebral transformation of l-dopa to dopamine. Because of the peripheral action there are much less side effects. c. Combining the two drugs allows the use of much lower doses of L-dopa. d. No pyridoxine interactions e. Because more L-dopa gets into the brain, CNS side effects are increased such as: involuntary movements, eyelid spasms, and mental changes. Parcopa = levodopa and carbidopa a dissolving tablet Stalevo = levodopa, carbidopa and entacapone.
3. 4.
DOPAMINE AGONISTS Dopamine agonists are used alone in mild disease or in conjunction with L-dopa in advanced disease. Even when used long term, they have less wearing off effect and less dystonias. Can cause more orthostatic hypotension, hallucinations, and sudden attacks of sleep. No dietary restrictions. Two classes of dopamine agonists: Non-ergot alkaloids and Ergot alkaloids Non-ergot Alkaloids: 1. Pramipexole [Mirapex] a. Used alone early on and with ldopa later on. b. Also used for restless leg syndrome c. Agonizes dopamine receptors at both presynaptic and postsynaptic sites
28 Side effects: i. Hallucinations, dizziness, drowsiness, nausea. ii. Orthostatic hypotension (>50% or pts) iii. Sleep attacks iv. Blood dyscracias Apomorphine [Apokyn] a. SC injection b. Not for scheduled use just a dose for off episodes c. Does not bind to morphine receptors no analgesia d. Side effects: i. Sleep attacks ii. Circulatory failure iii. Severe N/V use Tigan for 3 days prior to injection iv. Orthostatic hypotension, anorexia, agitation, erections Ropinirole [Requip] - (also for restless leg syndrome) a. Side effects: i. Syncope, drowsiness, fatigue d.
2.
3.
Ergot Alkaloids: 1. Bromocriptine [Parlodel] - Has many other uses also. a. Side effects: i. Seizures, shock, MI. ii. Psych reactions confusion, hallucinations, paranoia, nightmares Other drugs for PD: 1. Amantadine [Symmetrel] a. Action: releases dopamine from neuronal storage sites. Blocks uptake of dopamine into presynaptic neurons, thus permitting peripheral and central accumulation of dopamine. b. Indications: used as an antidyskinetic and also as an antiviral. c. Effectiveness is usually limited to about 6 - 12 months because functioning nerves decrease as disease progresses. d. Side effects: impaired concentration, dizziness, increased irritability, nervousness, blurred vision, hallucinations, mood changes. N/V/A, constipation, HA, dry mouth. Purple-red skin spots. e. Can cause edema, CHF, psych illness, and increase the severity of seizures. 2. Catechol-O-methyltransferase [COMT] inhibitors COMT inhibitors enhance the effectiveness of levodopa by blocking COMT, one of the main enzymes responsible for breakdown of levodopa in the bloodstream a it reaches the brain. By preventing breakdown of levodopa in peripheral tissues, more is available for the brain. Their entire effect is from the increase in L-dopa in the brain. Drugs: 1. Tolcapone [Tasmar] - Pregnancy category C may cause liver failure. 2. Entacapone [Comtan] - Pregnancy category D. Side Effects: Dyskinesia (due to higher levels of dopamine), N/V, orthostatic hypotension, psych sxs, urine discoloration. 3. MAO-B Inhibitors a. MAO-B inactivates dopamine. MAO-B inhibitors inhibit MAO-B, effectively increasing dopamine levels. b. Selegiline [Eldepryl] - PO, disintegrating tab, patch c. Rasagiline [Azilect] PO d. Side effects: i. Orthostatic hypotension, dyskinesias, confusion , N/V ii. HA, arthralgia, dyspepsia e. Dont need tyramine restriction unless high doses used.
You might also like
- PharmacologyDocument21 pagesPharmacologyMaridel Estioco100% (3)
- Drugs MnemonicsDocument6 pagesDrugs MnemonicsDarrylJavier100% (1)
- Drugs WorksheetDocument16 pagesDrugs Worksheetninja-2001No ratings yet
- Complete Drug GuideDocument225 pagesComplete Drug GuideJessica 'Baker' IsaacsNo ratings yet
- Drug Outline: Autonomic Nervous System Drug Class Drug OtherDocument4 pagesDrug Outline: Autonomic Nervous System Drug Class Drug OtherCess Lagera YbanezNo ratings yet
- Pharmacology MnemonicsDocument24 pagesPharmacology MnemonicsMrs3carpediem0% (1)
- Common Drugs ChartDocument15 pagesCommon Drugs Chartforminsko100% (1)
- Pharmacology Cheat Sheet - Generic Drug Stems - NurseslabsDocument12 pagesPharmacology Cheat Sheet - Generic Drug Stems - NurseslabsKc Mea Paran BorjaNo ratings yet
- Learning Packet in Level 1-NCM 106 NURSING PHARMACOLOGY: College of Nursing School Year 2020-2021Document15 pagesLearning Packet in Level 1-NCM 106 NURSING PHARMACOLOGY: College of Nursing School Year 2020-2021Nur Sanaani100% (1)
- Nursing Pharmacology Drug Study GuideDocument15 pagesNursing Pharmacology Drug Study GuideChelsea SmithNo ratings yet
- Cholinergics and Cholinergic BlockersDocument5 pagesCholinergics and Cholinergic Blockersapi-3739910100% (3)
- Antiinfectives Drug TableDocument5 pagesAntiinfectives Drug Tablecdp1587100% (3)
- Pharmacology ChartDocument6 pagesPharmacology ChartPaula67% (3)
- 4x6 Module 6 Drug CardsDocument10 pages4x6 Module 6 Drug CardsQueennitaNo ratings yet
- Pharmacology Nursing ReviewDocument19 pagesPharmacology Nursing Reviewp_dawg50% (2)
- Nursing Pharmacology Perfusion Study GuideDocument9 pagesNursing Pharmacology Perfusion Study GuideChelsea SmithNo ratings yet
- Pharmacology MnemonicsDocument17 pagesPharmacology MnemonicsJuvenis SampangNo ratings yet
- Pharmacology Question BankDocument24 pagesPharmacology Question BankSiri SriNo ratings yet
- Drug ChartDocument8 pagesDrug Chartstudentalwaysstudy100% (1)
- Pharmacology Test 1Document39 pagesPharmacology Test 1Niki BolinNo ratings yet
- Cholinergic DrugsDocument11 pagesCholinergic Drugsshivanshpande100% (1)
- Exam Cram Cheet SheetDocument2 pagesExam Cram Cheet SheetSheila Stenson-Roberts100% (1)
- NCLEX Review: Pharmacology Charlene Natale, BSN, RNDocument43 pagesNCLEX Review: Pharmacology Charlene Natale, BSN, RNMenly Susada100% (1)
- 13 How To Survive - PharmacologyDocument34 pages13 How To Survive - Pharmacologysophiesurvivalguides100% (1)
- NCLEX Pharmacology LPDocument53 pagesNCLEX Pharmacology LPSara Pirman100% (1)
- Pharmacology of Cardiac Diseases MINEDocument3 pagesPharmacology of Cardiac Diseases MINEMitu Miressa تNo ratings yet
- Pharmacology Clear and Simple A Guide To Drug Classifications and Dosage Calculations 2nd Edition Watkins Solutions ManualDocument4 pagesPharmacology Clear and Simple A Guide To Drug Classifications and Dosage Calculations 2nd Edition Watkins Solutions ManualJamesJoFrancis100% (1)
- Pharmacology Chart 3Document2 pagesPharmacology Chart 3Omar ClorNo ratings yet
- Pharmacy MnenomicsDocument12 pagesPharmacy MnenomicsNaresh BabuNo ratings yet
- Medical Surgical NotesDocument18 pagesMedical Surgical NotesshalomNo ratings yet
- Pharmacology Practice Test For NclexDocument10 pagesPharmacology Practice Test For NclexKira99% (96)
- Drug Cards 1Document20 pagesDrug Cards 1Keying Chen100% (1)
- Drug Interactions: What Is An Interaction?Document4 pagesDrug Interactions: What Is An Interaction?Leyla MajundaNo ratings yet
- Drug SuffixesDocument3 pagesDrug SuffixesjeromeasuncionNo ratings yet
- Hmg-Coa Reductase Inhibitors (Statins) : Side Effects, Contraindications, InteractionsDocument6 pagesHmg-Coa Reductase Inhibitors (Statins) : Side Effects, Contraindications, Interactionswaste78No ratings yet
- Mnemonics For NursesDocument29 pagesMnemonics For Nursesashdmb217100% (2)
- Pharmacology Notes: EliminationDocument14 pagesPharmacology Notes: EliminationHaifa ibrahimNo ratings yet
- Cholinergic Drug MnemonicsDocument1 pageCholinergic Drug Mnemonicssunshine151100% (1)
- Pharmacology Mnemonics PDFDocument27 pagesPharmacology Mnemonics PDFHasanAli100% (2)
- Cardiovascular Pharmacology OutlineDocument11 pagesCardiovascular Pharmacology OutlineLhay de OcampoNo ratings yet
- Antidiarrheal DrugsDocument4 pagesAntidiarrheal DrugsNadhirah ZulkifliNo ratings yet
- PHARM ATI ReviewDocument76 pagesPHARM ATI Reviewth233100% (1)
- Basic Principles of PharmacologyDocument13 pagesBasic Principles of Pharmacologyemmanuel100% (1)
- Anti-Infectives and AntibioticsDocument38 pagesAnti-Infectives and AntibioticsKarel Lu0% (1)
- Clinical Physiology and Pharmacology: The EssentialsFrom EverandClinical Physiology and Pharmacology: The EssentialsRating: 4 out of 5 stars4/5 (1)
- Review PharmacologyDocument137 pagesReview PharmacologyGeronimo GonzalezNo ratings yet
- Pharm ExamDocument293 pagesPharm ExamTrish HồNo ratings yet
- Pharmacology ReviewDocument100 pagesPharmacology Reviewjulialeo0% (2)
- Printable Drug Template CardDocument2 pagesPrintable Drug Template CardJennifer LeNo ratings yet
- Cholinergic and AnticholinergicDocument77 pagesCholinergic and Anticholinergicsweta sumanNo ratings yet
- EndocrinologyDocument46 pagesEndocrinology[161]Shuaib AktherNo ratings yet
- Drugs PharmacologyDocument75 pagesDrugs Pharmacologyapi-25987870100% (16)
- COMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideFrom EverandCOMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideNo ratings yet
- NURSING CARE OF ADULTS II: Passbooks Study GuideFrom EverandNURSING CARE OF ADULTS II: Passbooks Study GuideNo ratings yet
- Mechanisms of Drug Toxicity: Proceedings of the Third International Pharmacological MeetingFrom EverandMechanisms of Drug Toxicity: Proceedings of the Third International Pharmacological MeetingH. RaškováNo ratings yet
- NURSING CARE OF ADULTS I: Passbooks Study GuideFrom EverandNURSING CARE OF ADULTS I: Passbooks Study GuideNo ratings yet
- Dimensional Analysis For Nursing StudentsFrom EverandDimensional Analysis For Nursing StudentsNo ratings yet
- Basic Clinical Pharmacology 15Th Edition Bertram G Katzung Full ChapterDocument51 pagesBasic Clinical Pharmacology 15Th Edition Bertram G Katzung Full Chapterbenita.grimm191100% (5)
- Anzca MCQ Saqs Viva Question Bank Pharmacology Including StatisticsDocument62 pagesAnzca MCQ Saqs Viva Question Bank Pharmacology Including Statisticsالعراقي الصامدNo ratings yet
- General Principles of Pharmacology: Dr. GoverdhanDocument42 pagesGeneral Principles of Pharmacology: Dr. GoverdhanGoverdhan PeddireddyNo ratings yet
- U1P4 Experiments On Guinea Pig IleumDocument14 pagesU1P4 Experiments On Guinea Pig IleumMatt StowNo ratings yet
- Basic Principles of Pharmacology Handout PDFDocument111 pagesBasic Principles of Pharmacology Handout PDFRazel Kinette AzotesNo ratings yet
- Pharmacology For Nursing. Richard A. LehneDocument62 pagesPharmacology For Nursing. Richard A. LehneJC Ortiz-Carrillo50% (2)
- Chap 4 PrepU QuestionsDocument8 pagesChap 4 PrepU Questionsscorpioaj133No ratings yet
- 1 DDDDocument32 pages1 DDDivan abuyuanNo ratings yet
- Fentanyl Analouge SynthDocument11 pagesFentanyl Analouge SynthamesffNo ratings yet
- PHARMACOLOGY PrelimDocument26 pagesPHARMACOLOGY PrelimCrystal MiranaNo ratings yet
- Pharmacokinetics Lecture NotesDocument4 pagesPharmacokinetics Lecture NotesfaithsheepNo ratings yet
- Medicinal Chemistry-I: Dr. Firoj Ahmed Professor Department of Pharmaceutical Chemistry University of DhakaDocument91 pagesMedicinal Chemistry-I: Dr. Firoj Ahmed Professor Department of Pharmaceutical Chemistry University of DhakaRishtaul Alam100% (1)
- Oman Pharmacist Licensing Exam McqsDocument186 pagesOman Pharmacist Licensing Exam McqsMuhammad Amin100% (5)
- Transes PharmacodynamicsDocument36 pagesTranses PharmacodynamicsGwyneth Koleen Lopez100% (1)
- Mechanism of Action of QuetiapineDocument4 pagesMechanism of Action of QuetiapineThoha AlbaarNo ratings yet
- Biochemical Pharmacology - Lecture Notes, Study Material and Important Questions, AnswersDocument17 pagesBiochemical Pharmacology - Lecture Notes, Study Material and Important Questions, AnswersM.V. TVNo ratings yet
- AV Y TẾ 2Document27 pagesAV Y TẾ 2Đạt Bùi TiếnNo ratings yet
- Introduction To Medicinal Chemistry 1431 PDFDocument230 pagesIntroduction To Medicinal Chemistry 1431 PDFjames mellaleievNo ratings yet
- LIGAND - Receptors Concept FKG 2012 Univ YarsiDocument29 pagesLIGAND - Receptors Concept FKG 2012 Univ Yarsidayanara_245104654No ratings yet
- Drug Development and EvaluationDocument25 pagesDrug Development and EvaluationArlises SinagaNo ratings yet
- Principle of Organic Medicine Chemistry-RamaraoDocument331 pagesPrinciple of Organic Medicine Chemistry-RamaraoRevathiNo ratings yet
- Cat Remembered Questions Part 2Document69 pagesCat Remembered Questions Part 2soyrube86% (7)
- Pharmacology Ain Shams 123 - Compress 1Document552 pagesPharmacology Ain Shams 123 - Compress 1ahmed hoty100% (1)
- 3 - PharmacodynamicsDocument4 pages3 - PharmacodynamicsLloyd Selorio ArboledaNo ratings yet
- E.g., Phenylephrine Is Full Agonist at Alpha-Adrenoceptors. E.g., Aripipraxole Is Partial Antagonist at Selected Dopamine ReceptorsDocument1 pageE.g., Phenylephrine Is Full Agonist at Alpha-Adrenoceptors. E.g., Aripipraxole Is Partial Antagonist at Selected Dopamine ReceptorsSafura IjazNo ratings yet
- Hogan Lovells, The AKA's Law Firm Legal Brief Letter Regarding Kratom Scheduling Docket No. DEA-442Document35 pagesHogan Lovells, The AKA's Law Firm Legal Brief Letter Regarding Kratom Scheduling Docket No. DEA-442pogue972100% (1)
- MCQ PharmacologyDocument278 pagesMCQ PharmacologyNader Almaswary0% (1)
- Clinical Pharmacology For LUSUMA NotesDocument110 pagesClinical Pharmacology For LUSUMA NotesTausif Huq100% (1)
- Mini GsDocument26 pagesMini GsOlivia LuciannoNo ratings yet