You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Pharmaceutical Distribution Business PlanDocument5 pagesPharmaceutical Distribution Business Planmolla fentaye84% (19)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- 4 Hypovolemic ShockDocument21 pages4 Hypovolemic Shocksayednour100% (4)
- Answer Manufacturing Exam 1 - Module 5Document5 pagesAnswer Manufacturing Exam 1 - Module 5andit12180% (1)
- OxyContin TitrationDocument2 pagesOxyContin TitrationguntherfurlongNo ratings yet
- Fluid Electrolytes and Acid Base BalanceDocument108 pagesFluid Electrolytes and Acid Base BalancesayednourNo ratings yet
- Basics of Laser Orthopedic ViewDocument24 pagesBasics of Laser Orthopedic ViewsayednourNo ratings yet
- Assessment of Suitability For Lung Resection: Gerard Gould FRCA Adrian Pearce FRCADocument4 pagesAssessment of Suitability For Lung Resection: Gerard Gould FRCA Adrian Pearce FRCAsayednourNo ratings yet
- An Overview of Therapeutic Plasma ExchangeDocument65 pagesAn Overview of Therapeutic Plasma ExchangesayednourNo ratings yet
- General Anesthesia For Cesarean SectionDocument33 pagesGeneral Anesthesia For Cesarean Sectionsayednour100% (2)
- Anesthesia in The FutureDocument11 pagesAnesthesia in The FuturesayednourNo ratings yet
- AnestheticsDocument34 pagesAnestheticssayednourNo ratings yet
- 1 Plasmapheresis - 1Document61 pages1 Plasmapheresis - 1sayednour100% (1)
- Plasma Exchange For Heparin-Induced Thrombocytopenia: Is There Enough Evidence?Document4 pagesPlasma Exchange For Heparin-Induced Thrombocytopenia: Is There Enough Evidence?sayednourNo ratings yet
- Adrenal CrisisDocument27 pagesAdrenal CrisissayednourNo ratings yet
- 166 Serotonin SyndromeDocument5 pages166 Serotonin SyndromesayednourNo ratings yet
- 185 Anaesthesia in Pregnancy For Non Obstetric SurgeryDocument9 pages185 Anaesthesia in Pregnancy For Non Obstetric SurgeryaangrohmananiaNo ratings yet
- Cohort StudyDocument31 pagesCohort Studysayednour50% (2)
- Nitric Oxide An Overview: Salwa Hassan Teama M.D. NCI. Cairo UniversityDocument31 pagesNitric Oxide An Overview: Salwa Hassan Teama M.D. NCI. Cairo Universitysayednour100% (1)
- Review Mechanisms of Glucocorticoid-Induced Myopathy: O Schakman, H Gilson and J P ThissenDocument10 pagesReview Mechanisms of Glucocorticoid-Induced Myopathy: O Schakman, H Gilson and J P ThissensayednourNo ratings yet
- Developmental Genetics and Pharmacogeneticsdoc4301Document8 pagesDevelopmental Genetics and Pharmacogeneticsdoc4301sayednourNo ratings yet
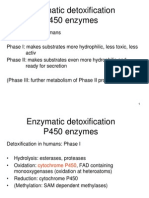
- Enzymatic Detoxification P450 EnzymesDocument22 pagesEnzymatic Detoxification P450 EnzymessayednourNo ratings yet
- Tony Chang, MD Tuesday Conference September 6, 2005Document75 pagesTony Chang, MD Tuesday Conference September 6, 2005sayednourNo ratings yet
- 8 Plasma Derivatives ProductsDocument12 pages8 Plasma Derivatives ProductssayednourNo ratings yet
- Data Item MasterDocument34 pagesData Item MasterDiniarti ApotekerNo ratings yet
- Clinical Pharma ExamDocument4 pagesClinical Pharma Examnancy voraNo ratings yet
- Burkholderia Cepacia Complex: Characteristics, Products Risks and Testing RequirementsDocument17 pagesBurkholderia Cepacia Complex: Characteristics, Products Risks and Testing RequirementsTim Sandle100% (1)
- Practice Guidelines: Enteral Nutrition Delivery For The Adult PatientDocument15 pagesPractice Guidelines: Enteral Nutrition Delivery For The Adult Patientdamondouglas100% (1)
- Pharma Companies 5Document8 pagesPharma Companies 5Devesh JhaNo ratings yet
- List of Pharmaceutical Companies in PuneDocument5 pagesList of Pharmaceutical Companies in PuneMuhammad SalmanNo ratings yet
- Ats SorowakoDocument12 pagesAts SorowakoFirmanNo ratings yet
- Chemical and Therapeutic IncompatibilitiesDocument34 pagesChemical and Therapeutic IncompatibilitiesAlyssa Marie Petonio BialaNo ratings yet
- Aldactone SpironlactoneDocument1 pageAldactone SpironlactoneCassie100% (1)
- ArcsDocument39 pagesArcsSharmaine PostradoNo ratings yet
- Stokon Vs Detil PenjualanDocument240 pagesStokon Vs Detil Penjualanasthenia8No ratings yet
- Posology and Dosage RegimenDocument24 pagesPosology and Dosage RegimenpmilyNo ratings yet
- Review Article On E-PharmacyDocument12 pagesReview Article On E-PharmacyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Uniformity Dosage Unit USPDocument4 pagesUniformity Dosage Unit USPwike marelitaNo ratings yet
- ASSAY METHOD DEVELOPMENT AND VALIDATION FOR THE ESTIMATION OF SOLIFENACIN SUCCINATE IN TABLETS BY UV SPECTROPHOTOMETRY N.J.R. Hepsebah, A. Ashok KumarDocument6 pagesASSAY METHOD DEVELOPMENT AND VALIDATION FOR THE ESTIMATION OF SOLIFENACIN SUCCINATE IN TABLETS BY UV SPECTROPHOTOMETRY N.J.R. Hepsebah, A. Ashok KumariajpsNo ratings yet
- Protein Binding of Drug: Page - 1 CMR College of Pharmacy, 2013Document18 pagesProtein Binding of Drug: Page - 1 CMR College of Pharmacy, 2013REDDYGAARI ABBAYINo ratings yet
- Comparative Study of Epidural Fentanyl and Buprenorphine For Post Operative Analgesia in Lower Abdominal and Lower Limb SurgeriesDocument8 pagesComparative Study of Epidural Fentanyl and Buprenorphine For Post Operative Analgesia in Lower Abdominal and Lower Limb SurgeriesIOSRjournalNo ratings yet
- Vicks B (Case)Document2 pagesVicks B (Case)Sana KhanNo ratings yet
- Validation Guide July2013Document37 pagesValidation Guide July2013Herdiwan NovindraNo ratings yet
- English Annual Report 2021-22Document172 pagesEnglish Annual Report 2021-22Ashish SharmaNo ratings yet
- Intermediate of OmeprazoleDocument4 pagesIntermediate of Omeprazolekanji63No ratings yet
- Live With: Dr. Fred BaughmanDocument16 pagesLive With: Dr. Fred BaughmanGerardo LagunesNo ratings yet
- SPJ ObatDocument10 pagesSPJ Obatdedi darmawanNo ratings yet
- Abdullahi V Pfizer PaperDocument2 pagesAbdullahi V Pfizer PaperTeam2KissNo ratings yet
- Pharmacy Service VA Design Guide: Final DraftDocument75 pagesPharmacy Service VA Design Guide: Final DraftAhmad Gamal Elden MAhanyNo ratings yet
- Development and Validation of UV-Spectrophotometric Method For Simultaneous Estimation of Amlodipine Besylate and Hydrochlorothiazide in Combined Dosage Form Including Stability StudyDocument7 pagesDevelopment and Validation of UV-Spectrophotometric Method For Simultaneous Estimation of Amlodipine Besylate and Hydrochlorothiazide in Combined Dosage Form Including Stability StudySukmana Laksana SaputraNo ratings yet
- DyspepsiaDocument8 pagesDyspepsiaaspNo ratings yet