You might also like
- Breaking the Chains of Diabetes. A Comprehensive Guide to Understanding and Managing Diabetes NaturallyFrom EverandBreaking the Chains of Diabetes. A Comprehensive Guide to Understanding and Managing Diabetes NaturallyNo ratings yet
- A Guide to Diabetes: Symptoms; Causes; Treatment; PreventionFrom EverandA Guide to Diabetes: Symptoms; Causes; Treatment; PreventionNo ratings yet
- Dianosis Dan Klasifikasi DMDocument8 pagesDianosis Dan Klasifikasi DMFatkhul Ali ImronNo ratings yet
- Diagnosis and Classification of Diabetes 2013Document8 pagesDiagnosis and Classification of Diabetes 2013Armando ATNo ratings yet
- Diagnosis and Classi Fication of Diabetes Mellitus: Merican Iabetes SsociationDocument8 pagesDiagnosis and Classi Fication of Diabetes Mellitus: Merican Iabetes SsociationSmeu MirelaNo ratings yet
- Diabetes MelitusDocument8 pagesDiabetes MelituswahyunhyNo ratings yet
- Diagnosis and Classi Fication of Diabetes Mellitus: Merican Iabetes SsociationDocument8 pagesDiagnosis and Classi Fication of Diabetes Mellitus: Merican Iabetes SsociationQori AdawiyahNo ratings yet
- Diagnosis and Classification of Diabetes Mellitus: Merican Iabetes SsociationDocument6 pagesDiagnosis and Classification of Diabetes Mellitus: Merican Iabetes SsociationEvhy Noviana NingsiNo ratings yet
- Classification of Diabetes Mellitus and Other Categories of Glucose RegulationDocument15 pagesClassification of Diabetes Mellitus and Other Categories of Glucose RegulationbreilanoNo ratings yet
- Diabetes MellitusDocument38 pagesDiabetes Mellitusمیاں منیب احمدNo ratings yet
- ZDC 10110000 S 62Document8 pagesZDC 10110000 S 62Hanim MafulahNo ratings yet
- Pancreatic Gland Disorders CompleteDocument58 pagesPancreatic Gland Disorders CompletejawadNo ratings yet
- Diabetes MelitusDocument44 pagesDiabetes MelitusDwi Novianti SugihartiNo ratings yet
- Review of Diabetes Mellitus: Loo Hariyanto Raharjo, DR., Msi. Ketua Program Studi Pendidikan Dokter Fk-UwksDocument51 pagesReview of Diabetes Mellitus: Loo Hariyanto Raharjo, DR., Msi. Ketua Program Studi Pendidikan Dokter Fk-UwksBerlia NarayaniNo ratings yet
- Dr. Pragasam Viswanathan Professor, SBSTDocument43 pagesDr. Pragasam Viswanathan Professor, SBSTMaru Mengesha Worku 18BBT0285No ratings yet
- Definition and Diagnostic Criteria For Diabetes Mellitus and Other Categories of Glucose IntoleranceDocument4 pagesDefinition and Diagnostic Criteria For Diabetes Mellitus and Other Categories of Glucose Intolerancevai2No ratings yet
- Pedoman Diet Diabetes MelitusDocument45 pagesPedoman Diet Diabetes Melitus51limasatuNo ratings yet
- Physiology and Causes of DiabatesDocument7 pagesPhysiology and Causes of DiabatesasaadsarfrazNo ratings yet
- DefinitionDocument6 pagesDefinitionChana 'eLecter' ChuLumNo ratings yet
- Diabetes Mellitus Is A Group of Metabolic Diseases Characterized byDocument67 pagesDiabetes Mellitus Is A Group of Metabolic Diseases Characterized byBivek TimalsinaNo ratings yet
- Supplementary Information To Chapter 24: Review: Diabetes MellitusDocument11 pagesSupplementary Information To Chapter 24: Review: Diabetes MellitusAaron JoseNo ratings yet
- Diagnosis Inggris PDFDocument10 pagesDiagnosis Inggris PDFMuhammad AbiyasaNo ratings yet
- Diabetes in PregnancyDocument14 pagesDiabetes in Pregnancywalaaahmed213No ratings yet
- Diabetes PDFDocument8 pagesDiabetes PDFFelipe SalinasNo ratings yet
- DM ThyroidDocument184 pagesDM ThyroidtentenNo ratings yet
- Diabetes Mellitus Type 2Document16 pagesDiabetes Mellitus Type 2MTs MIFDANo ratings yet
- Diabetic PatientDocument16 pagesDiabetic PatientGabii OrdoñezNo ratings yet
- Type 2 Diabetes MellitusDocument19 pagesType 2 Diabetes MellitusFelipe Senn Guerrero100% (2)
- Bka Case FinalDocument26 pagesBka Case FinalJayson SorianoNo ratings yet
- Diabetes 2016Document54 pagesDiabetes 2016JesseniaChaupisZevallosNo ratings yet
- Diabetes MellitusDocument43 pagesDiabetes MellitusCece RereNo ratings yet
- Diabetes Mellitus: Group 3ADocument8 pagesDiabetes Mellitus: Group 3AAradhanaRamchandaniNo ratings yet
- Diabetes MellitusDocument19 pagesDiabetes MellitusHaleelu Abdul JaleelNo ratings yet
- Clinical Management of Diabetes in The Elderly: Practical PointersDocument4 pagesClinical Management of Diabetes in The Elderly: Practical Pointersannaafia69969No ratings yet
- Diabetes MellitusDocument110 pagesDiabetes MellitusToluwani Lade-ige100% (1)
- Type 1 Diabetes Mellitus: PathoDocument6 pagesType 1 Diabetes Mellitus: PathoMary JoyceNo ratings yet
- Diabetes Mellitus 1Document19 pagesDiabetes Mellitus 1shamma shahulhameedNo ratings yet
- Diagnosis and Classification of Diabetes Mellitus (DR - Boby)Document19 pagesDiagnosis and Classification of Diabetes Mellitus (DR - Boby)Boby Veland ArdiansyahNo ratings yet
- Diabetes Mellitus - SlidesDocument28 pagesDiabetes Mellitus - SlidesReem ShamasNo ratings yet
- Diabetus MillitusDocument66 pagesDiabetus MillitusNur IswantoNo ratings yet
- Diabetes 1Document22 pagesDiabetes 1aparna shamaNo ratings yet
- Dissertation Diabetes Mellitus Type 2Document5 pagesDissertation Diabetes Mellitus Type 2Syracuse100% (1)
- IntroductionDocument22 pagesIntroductionjayrana40No ratings yet
- Anesthesiology Case PresDocument26 pagesAnesthesiology Case PresNasrah N. MusaNo ratings yet
- Diabetes: Oral Health TopicsDocument9 pagesDiabetes: Oral Health TopicsAndrei StamateNo ratings yet
- Diabetes MellitusDocument79 pagesDiabetes Mellituskhalid saifur rahman khanNo ratings yet
- Dr. Rasha Salama: PHD Public Health, Suez Canal University, Egypt Diabetes MSC, Cardiff University, United KingdomDocument37 pagesDr. Rasha Salama: PHD Public Health, Suez Canal University, Egypt Diabetes MSC, Cardiff University, United Kingdomdwi istutikNo ratings yet
- Dibetes FinalDocument50 pagesDibetes FinalPiyusha SharmaNo ratings yet
- Diabetes MellitusDocument21 pagesDiabetes MellitusJuri GallosNo ratings yet
- Diabetes Mellitus Diabetes Mellitus, Often Simply Diabetes, Is A Syndrome Characterized by DisorderedDocument8 pagesDiabetes Mellitus Diabetes Mellitus, Often Simply Diabetes, Is A Syndrome Characterized by DisorderedRachel Ann BatayolaNo ratings yet
- Session 27 Diabetes M - 1Document47 pagesSession 27 Diabetes M - 1Kuchby MskudeNo ratings yet
- Nursing Care Plans For Diabetes MellitusDocument12 pagesNursing Care Plans For Diabetes MellitusPuteri AzmanNo ratings yet
- Diabetes MiellitusDocument14 pagesDiabetes MiellitusMha Mencoba BerubahNo ratings yet
- 2 Diabetes Mellitus and DiagnosticDocument33 pages2 Diabetes Mellitus and DiagnosticSifa RismawatiNo ratings yet
- Type 2 Diabetes Cookbook for Beginners: Mastering Balanced, Low-Sugar Eating for Enhanced Well-being and Effective Diabetes Control [V EDITION]From EverandType 2 Diabetes Cookbook for Beginners: Mastering Balanced, Low-Sugar Eating for Enhanced Well-being and Effective Diabetes Control [V EDITION]Rating: 5 out of 5 stars5/5 (7)
- Conquering Diabetes: Fenugreek Success in Regulating Blood Sugar LevelsFrom EverandConquering Diabetes: Fenugreek Success in Regulating Blood Sugar LevelsNo ratings yet
- Ultimate Diet Plan for Diabetic Patients: Revolutionizing Diabetic NutritionFrom EverandUltimate Diet Plan for Diabetic Patients: Revolutionizing Diabetic NutritionNo ratings yet
- 09.Third-Party Reimbursement For Diabetes Care, Self-Management Education, and Supplies PDFDocument2 pages09.Third-Party Reimbursement For Diabetes Care, Self-Management Education, and Supplies PDFEliuth ZamoraNo ratings yet
- 08.diabetes and Employment PDFDocument5 pages08.diabetes and Employment PDFEliuth ZamoraNo ratings yet
- 12.technical Reviews PDFDocument1 page12.technical Reviews PDFEliuth Zamora0% (1)
- 03.executive Summary Standards of Medical Care in Diabetes 2009 PDFDocument7 pages03.executive Summary Standards of Medical Care in Diabetes 2009 PDFEliuth ZamoraNo ratings yet
- DMIIDocument5 pagesDMIIpalma_oscar3153No ratings yet
- Standards of Medical Care in Diabetes 2009Document49 pagesStandards of Medical Care in Diabetes 2009Teoh CYunNo ratings yet
- 07.diabetes Management in Correctional Institutions PDFDocument7 pages07.diabetes Management in Correctional Institutions PDFEliuth ZamoraNo ratings yet
- S01Document2 pagesS01Hossam AlhossainyNo ratings yet
- 10.position Statements PDFDocument1 page10.position Statements PDFEliuth ZamoraNo ratings yet
- Mittee ReportsDocument2 pagesMittee ReportsEliuth ZamoraNo ratings yet
- ADA - Clinical Practice Recommendations-2009Document3 pagesADA - Clinical Practice Recommendations-2009sgamit1962No ratings yet
- 11.national Standards For Diabetes Self-Management Education PDFDocument8 pages11.national Standards For Diabetes Self-Management Education PDFEliuth Zamora100% (1)
- Overdose Tricyclic Agents PDFDocument6 pagesOverdose Tricyclic Agents PDFEliuth ZamoraNo ratings yet
- Amitriptilina Overdose PDFDocument3 pagesAmitriptilina Overdose PDFEliuth ZamoraNo ratings yet
- Lipid Rescue For Intoxication by Tca PDFDocument3 pagesLipid Rescue For Intoxication by Tca PDFEliuth ZamoraNo ratings yet
- Organophosphorus Poisoning PDFDocument5 pagesOrganophosphorus Poisoning PDFEliuth Zamora100% (1)
- Management of Preterm LaborDocument2 pagesManagement of Preterm LaborpolygoneNo ratings yet
- Mycotoxin in Food Supply Chain (Peanuts)Document2 pagesMycotoxin in Food Supply Chain (Peanuts)Ghanthimathi GvsNo ratings yet
- Ras Shastra PPT 6Document10 pagesRas Shastra PPT 6Soham BhureNo ratings yet
- Carboset CA-600 - CST600 - CO - enDocument3 pagesCarboset CA-600 - CST600 - CO - enNilsNo ratings yet
- Parche CRP 65 - Ficha Técnica - en InglesDocument2 pagesParche CRP 65 - Ficha Técnica - en IngleserwinvillarNo ratings yet
- Big 9 Master SoalDocument6 pagesBig 9 Master Soallilik masrukhahNo ratings yet
- Oil ShaleDocument13 pagesOil Shalergopi_83No ratings yet
- Guides To The Freshwater Invertebrates of Southern Africa Volume 2 - Crustacea IDocument136 pagesGuides To The Freshwater Invertebrates of Southern Africa Volume 2 - Crustacea IdaggaboomNo ratings yet
- Science 9 Q4 SML17 V2Document15 pagesScience 9 Q4 SML17 V2HotdogNo ratings yet
- Ec Declaration of Conformity: W1/35 KEV KIRK - Protective Gloves - Cathegory IIDocument3 pagesEc Declaration of Conformity: W1/35 KEV KIRK - Protective Gloves - Cathegory IICrystal HooverNo ratings yet
- Case Study of Milk ProductionDocument46 pagesCase Study of Milk Productionmian21100% (2)
- Registration Statement (For Single Proprietor)Document2 pagesRegistration Statement (For Single Proprietor)Sherwin SalanayNo ratings yet
- Maintenance Instructions, Parts Identification & Seal Kits For Series 2H / 2HD / 2HB & 3H / 3HD / 3HBDocument10 pagesMaintenance Instructions, Parts Identification & Seal Kits For Series 2H / 2HD / 2HB & 3H / 3HD / 3HBAtaa AssaadNo ratings yet
- Characteristics of Testable HypothesesDocument30 pagesCharacteristics of Testable HypothesesMarivic Diano67% (3)
- Null 6 PDFDocument1 pageNull 6 PDFSimbarashe ChikariNo ratings yet
- Chia (Salvia Hispanica L.) Oil Stability Study of The Effect of NaturDocument7 pagesChia (Salvia Hispanica L.) Oil Stability Study of The Effect of NaturInta Nur IlmiNo ratings yet
- Starkville Dispatch Eedition 9-10-20Document12 pagesStarkville Dispatch Eedition 9-10-20The DispatchNo ratings yet
- 2020 ROTH IRA 229664667 Form 5498Document2 pages2020 ROTH IRA 229664667 Form 5498hk100% (1)
- EIL Document On Motor, PanelDocument62 pagesEIL Document On Motor, PanelArindam Samanta100% (1)
- Iomm VFD-3 030112Document100 pagesIomm VFD-3 030112Alexander100% (1)
- HVAC (Heating, Ventilation and Air Conditioning) : SRS PrecautionsDocument1 pageHVAC (Heating, Ventilation and Air Conditioning) : SRS PrecautionssoftallNo ratings yet
- Present Continuous Exercises Test 1 - Positive Statements ExerciseDocument2 pagesPresent Continuous Exercises Test 1 - Positive Statements Exerciseangel omar peraltaNo ratings yet
- DT 2107Document1 pageDT 2107Richard PeriyanayagamNo ratings yet
- Lesson 1 - Intro To Highway EngineeringDocument15 pagesLesson 1 - Intro To Highway EngineeringSaoirseNo ratings yet
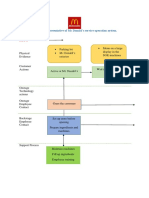
- Blueprint Huynh My Ky Duyen 2022 McDonald'sDocument2 pagesBlueprint Huynh My Ky Duyen 2022 McDonald'sHuỳnh Mỹ Kỳ DuyênNo ratings yet
- FEM 3004 - Lab 10 Part 2editedDocument26 pagesFEM 3004 - Lab 10 Part 2editedAINA NADHIRAH BINTI A ROZEY / UPMNo ratings yet
- Review - Practical Accounting 1Document2 pagesReview - Practical Accounting 1Kath LeynesNo ratings yet
- REV Description Appr'D CHK'D Prep'D: Tolerances (Unless Otherwise Stated) - (In)Document2 pagesREV Description Appr'D CHK'D Prep'D: Tolerances (Unless Otherwise Stated) - (In)Bacano CapoeiraNo ratings yet
- Drug-Nutrient Interaction in Prescriptions ForDocument7 pagesDrug-Nutrient Interaction in Prescriptions ForRafika DitaNo ratings yet
- Health Promotion Officers - CPD Booklet Schedule PDFDocument5 pagesHealth Promotion Officers - CPD Booklet Schedule PDFcharles KadzongaukamaNo ratings yet
























































![Type 2 Diabetes Cookbook for Beginners: Mastering Balanced, Low-Sugar Eating for Enhanced Well-being and Effective Diabetes Control [V EDITION]](https://imgv2-1-f.scribdassets.com/img/word_document/616633879/149x198/173640cf06/1710278044?v=1)