You might also like
- Avicenna ADocument17 pagesAvicenna ADeepu VijayaBhanuNo ratings yet
- PhylosophyDocument20 pagesPhylosophyDeepu VijayaBhanuNo ratings yet
- Teacher Role - M.SCDocument9 pagesTeacher Role - M.SCDeepu VijayaBhanuNo ratings yet
- Discipline - M.SCDocument17 pagesDiscipline - M.SCDeepu VijayaBhanuNo ratings yet
- Menstrual Irreglarities 2Document19 pagesMenstrual Irreglarities 2Deepu VijayaBhanuNo ratings yet
- ArdsDocument29 pagesArdsDeepu VijayaBhanuNo ratings yet
- LeptospirosisDocument9 pagesLeptospirosisDeepu VijayaBhanuNo ratings yet
- Discipline - M.SCDocument17 pagesDiscipline - M.SCDeepu VijayaBhanuNo ratings yet
- Source of Infections 1. Endogenous SourceDocument6 pagesSource of Infections 1. Endogenous SourceDeepu VijayaBhanuNo ratings yet
- Critical ThinkingDocument32 pagesCritical ThinkingDeepu VijayaBhanuNo ratings yet
- Student WelfareDocument2 pagesStudent WelfareDeepu VijayaBhanu100% (1)
- Public Relations M.SCDocument9 pagesPublic Relations M.SCDeepu VijayaBhanuNo ratings yet
- BudgetDocument12 pagesBudgetDeepu VijayaBhanu100% (1)
- Adminis-Responsibility For CurriculamDocument12 pagesAdminis-Responsibility For CurriculamDeepu VijayaBhanuNo ratings yet
- Inservice EducationDocument7 pagesInservice EducationDeepu VijayaBhanu97% (30)
- GuidanceDocument13 pagesGuidanceDeepu VijayaBhanuNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Precautionary and Sanitary Practices in Handling FoodDocument31 pagesPrecautionary and Sanitary Practices in Handling FoodBrenNan ChannelNo ratings yet
- Ilovepdf Merged PDFDocument134 pagesIlovepdf Merged PDFhelalNo ratings yet
- Bulacan State University College of Nursing City of Malolos, BulacanDocument2 pagesBulacan State University College of Nursing City of Malolos, BulacanVIRGINIA M. SANTOSNo ratings yet
- Top 50 Global Stem Cell InfluencersDocument25 pagesTop 50 Global Stem Cell InfluencersranasoftNo ratings yet
- Nervous System Brain Retina - QDocument70 pagesNervous System Brain Retina - QVarshLokNo ratings yet
- CHAPTER 11: The History and Physical Examination: An Evidence Based ApproachDocument5 pagesCHAPTER 11: The History and Physical Examination: An Evidence Based ApproachReda SoNo ratings yet
- Katrina D. Varon Bs-Nursing 2Document13 pagesKatrina D. Varon Bs-Nursing 2Marc FresNo ratings yet
- Preventive Resin Restorations: Review ArticlesDocument3 pagesPreventive Resin Restorations: Review ArticlesClaypella MaskNo ratings yet
- Can I Get That in WritingDocument4 pagesCan I Get That in WritingNorische100% (1)
- The Tragedy of Schizophrenia Without PsychotherapyDocument30 pagesThe Tragedy of Schizophrenia Without PsychotherapyRachel AHNo ratings yet
- Sept 3 2017Document7 pagesSept 3 2017Reda SoNo ratings yet
- Psychopharma NotesDocument3 pagesPsychopharma Noteszh4hft6pnzNo ratings yet
- Post Natal ExercisesDocument7 pagesPost Natal ExercisesEvie Dolpin BlueNo ratings yet
- Ast (Sgot) ColorDocument2 pagesAst (Sgot) ColorShribagla MukhiNo ratings yet
- Note Regarding Retiring DoctorsDocument3 pagesNote Regarding Retiring DoctorsnamankumaragrawalNo ratings yet
- Perbedaan Kadar Hbsag Sampel Serum Dan Plasma Metode Clia Pada PendonorDocument7 pagesPerbedaan Kadar Hbsag Sampel Serum Dan Plasma Metode Clia Pada PendonorAAK DHGRiski MaulanaNo ratings yet
- Kainan University ApplicationDocument25 pagesKainan University ApplicationGeraldine RiveraNo ratings yet
- Kansas Foodborne Illness ManualDocument186 pagesKansas Foodborne Illness ManualLeo M. Pedro Jr.No ratings yet
- Menstrual DisordersDocument45 pagesMenstrual DisordersMegat Mohd Azman Adzmi100% (1)
- Status of DNB Seats - Bulletin - StatewiseSpecialitywise - WU26022009Document142 pagesStatus of DNB Seats - Bulletin - StatewiseSpecialitywise - WU26022009raghavagummadiNo ratings yet
- Dental AssistantDocument2 pagesDental Assistantapi-78993102No ratings yet
- Coliform Analysis in Wastewater 2012Document24 pagesColiform Analysis in Wastewater 2012engrbvgNo ratings yet
- Daftar ObatDocument1 pageDaftar ObatPramukadua DepokNo ratings yet
- HistoryDocument47 pagesHistoryRajesh IthaNo ratings yet
- Mendiguchia 2012 Rectus Femoris Muscle Injuries in Football-A Clinically Relevant Review of Mechanisms of Injury, Risk Factors and Preventive Strategies PDFDocument11 pagesMendiguchia 2012 Rectus Femoris Muscle Injuries in Football-A Clinically Relevant Review of Mechanisms of Injury, Risk Factors and Preventive Strategies PDFJuan PalomoNo ratings yet
- Animal Welfare Board of India v. A Nagaraja & Ors PDFDocument117 pagesAnimal Welfare Board of India v. A Nagaraja & Ors PDFBar & Bench100% (1)
- S/N Description UnitDocument16 pagesS/N Description UnitPeccamb SurgicalNo ratings yet
- Computer Addiction Power Point PresentationDocument24 pagesComputer Addiction Power Point PresentationGee A50% (4)
- Vital Signs Vital Signs: Importance: ImportanceDocument6 pagesVital Signs Vital Signs: Importance: ImportanceTyron KristianNo ratings yet
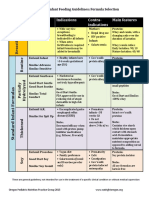
- Formula Selection OPNPGDocument2 pagesFormula Selection OPNPGRina PratiwiNo ratings yet