You might also like
- 2 HSE-PlanDocument40 pages2 HSE-Plan09tlionNo ratings yet
- Maraba Al Iraq Al Khadraa: Emergency Drill ReportDocument3 pagesMaraba Al Iraq Al Khadraa: Emergency Drill Reportfdfddf dfsdfNo ratings yet
- Shiva Enterprises: Accident & Incident LogDocument1 pageShiva Enterprises: Accident & Incident LogRahul KumarNo ratings yet
- General Safety Inspection ChecklistDocument1 pageGeneral Safety Inspection ChecklistAyşe BalamirNo ratings yet
- Site Clinic ChecklistDocument1 pageSite Clinic ChecklistEldhose Varghese100% (1)
- Section A - Identifying: Note in Case of Personal Accident Fill Up Form TOM/FO/028Document2 pagesSection A - Identifying: Note in Case of Personal Accident Fill Up Form TOM/FO/028jorge walliser martinNo ratings yet
- Monthly First Aid Log Sheet BlankDocument1 pageMonthly First Aid Log Sheet BlankJunard Lu HapNo ratings yet
- FINAL Shivani Confined Space PermitDocument1 pageFINAL Shivani Confined Space PermitVimal SinghNo ratings yet
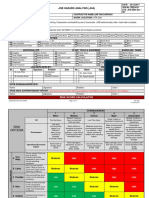
- JHA For Hill Cutting Activities.R.01Document8 pagesJHA For Hill Cutting Activities.R.01SreekumarNo ratings yet
- HSE Manual Documentation PDFDocument9 pagesHSE Manual Documentation PDFemeka2012No ratings yet
- Form-58 Confined Space Entry LogDocument1 pageForm-58 Confined Space Entry LogRajesh Kumar SinghNo ratings yet
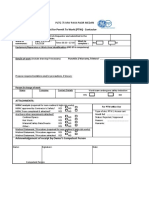
- SH-F43 - PTW Format - R02Document2 pagesSH-F43 - PTW Format - R02vini100% (1)
- Note Emshe - Hazard Identification ControlDocument38 pagesNote Emshe - Hazard Identification ControlMel Yusoff100% (1)
- TMT90 - HSE Corrective Action Plan WICR 61Document5 pagesTMT90 - HSE Corrective Action Plan WICR 61Abn BK100% (2)
- Safety Committee Meeting Minutes TemplateDocument3 pagesSafety Committee Meeting Minutes TemplateKashémNo ratings yet
- HSE FRM-32 Incident Investigation ReportDocument4 pagesHSE FRM-32 Incident Investigation ReportPerwez21No ratings yet
- F-49 Full Body Harness Inspection ChecklistDocument1 pageF-49 Full Body Harness Inspection ChecklistSKH Culture100% (1)
- 09-Safety Training Attendance SheetDocument1 page09-Safety Training Attendance SheetSainu Kalathingal0% (1)
- Monthly Safety Statisics ReportDocument1 pageMonthly Safety Statisics ReportTayyab Mayo100% (1)
- F 016 Accommodation Inspection ChecklistDocument4 pagesF 016 Accommodation Inspection Checklistngomsia parfaitNo ratings yet
- Emergency Response Plan Tank Cleaning: - Safety & SPV - Safety & Ert PTDocument3 pagesEmergency Response Plan Tank Cleaning: - Safety & SPV - Safety & Ert PTSyifa Ula HamidyaNo ratings yet
- PPE Issue ReordDocument1 pagePPE Issue ReordHuman ResourcesNo ratings yet
- Site Access Request Form (ACBA - 0105 (BGW00174) )Document1 pageSite Access Request Form (ACBA - 0105 (BGW00174) )Maijul Islam Sarkar JituNo ratings yet
- Jha - Forklift OperationalDocument14 pagesJha - Forklift OperationalAliff ApamNo ratings yet
- Confined Space Entry Risk AssessmentDocument9 pagesConfined Space Entry Risk Assessmentkoketso0% (1)
- PARCO Project HSE Closing ReportDocument22 pagesPARCO Project HSE Closing ReportHabib UllahNo ratings yet
- HLG HSE SPI FM 051A Rev 00 Lifting Equipment Audit ChecklistDocument1 pageHLG HSE SPI FM 051A Rev 00 Lifting Equipment Audit ChecklistLemuel Petronio100% (3)
- JHA 004 - Machine Excavaton, Backfill and Compaction Work - REV000 (For Sir)Document7 pagesJHA 004 - Machine Excavaton, Backfill and Compaction Work - REV000 (For Sir)Venkadesh Periathambi100% (1)
- HSE Statistic Trend Analysis Project 760Document18 pagesHSE Statistic Trend Analysis Project 760AbeAu NewNo ratings yet
- Jobsite Safety Checklist Long Ver 1Document5 pagesJobsite Safety Checklist Long Ver 1Usman ShahidNo ratings yet
- Form Report Safety CampaignDocument1 pageForm Report Safety CampaignErlan Gus HermawanNo ratings yet
- Daily Tool Box MeetingDocument1 pageDaily Tool Box MeetingVipul ShankarNo ratings yet
- Chemical Manifest and Hazardous Chemical Substance List KathuDocument13 pagesChemical Manifest and Hazardous Chemical Substance List KathuVictorNo ratings yet
- Scaffolding Risk AssesmentDocument12 pagesScaffolding Risk Assesmentsubhaschandra100% (1)
- Vendor Information Form 2Document1 pageVendor Information Form 2umeshd_9114923No ratings yet
- General Site Safety - SignDocument1 pageGeneral Site Safety - SignVũ GiangNo ratings yet
- Construction Site Inspection Check List ALMCDocument2 pagesConstruction Site Inspection Check List ALMCAmeerHamzaWarraichNo ratings yet
- HSE-000-For-0005 Preliminary Incident Report FormDocument1 pageHSE-000-For-0005 Preliminary Incident Report Formernesto100% (2)
- New Monthly SHE ReportsDocument21 pagesNew Monthly SHE ReportsGIRI BISWAS100% (1)
- HSE 09 Hotwork PermitDocument1 pageHSE 09 Hotwork PermitBa N Nhim100% (1)
- Incident Safety Officer Skill SheetsDocument5 pagesIncident Safety Officer Skill SheetssofyansofyanNo ratings yet
- Form - 32 - Health RegisterDocument1 pageForm - 32 - Health Registerhdpanchal86No ratings yet
- Loto FormDocument9 pagesLoto FormJoey GNo ratings yet
- HSE Presentation TemplateDocument10 pagesHSE Presentation TemplatejeffreyNo ratings yet
- Worker Orientation Checklist EnglishDocument1 pageWorker Orientation Checklist EnglishSayed DarwishNo ratings yet
- Emergency PlanDocument1 pageEmergency Planapi-285003764No ratings yet
- Injury Incident Report FormDocument3 pagesInjury Incident Report FormDave Joseph Conde100% (1)
- Request For Permit To Work (PTW) - Contactor Application: PLTG 75 MW Paya Pasir MedanDocument2 pagesRequest For Permit To Work (PTW) - Contactor Application: PLTG 75 MW Paya Pasir MedanDimas Dwi SwarnaNo ratings yet
- Tool Box Training-EnglishDocument8 pagesTool Box Training-Englishraj KumarNo ratings yet
- 2 03 Health and Safety Emergency Plan GuidelinesDocument10 pages2 03 Health and Safety Emergency Plan GuidelinesEng Muhammad MarzoukNo ratings yet
- BSA Alert 13.69 Fall of Materials From ScaffoldingDocument1 pageBSA Alert 13.69 Fall of Materials From ScaffoldingsubhanmusadiqNo ratings yet
- HSE Induction - Attendance FormDocument1 pageHSE Induction - Attendance FormSyed Mohammad NeezarNo ratings yet
- Alfanar Co. Sub-Contractor: Weekly Safety ReportDocument3 pagesAlfanar Co. Sub-Contractor: Weekly Safety ReportSarmad Hussain67% (3)
- Effluent Discharge Mock Emergency and Evalaution ReportDocument3 pagesEffluent Discharge Mock Emergency and Evalaution Reportremember0% (1)
- Hse Enforcement Report - May 24, 2014Document4 pagesHse Enforcement Report - May 24, 2014yelsa otrebla100% (1)
- 26 - HSE-Road Safety and Vehicles OperationDocument7 pages26 - HSE-Road Safety and Vehicles OperationP Eng Suraj SinghNo ratings yet
- HSE-PRO-03-INR 0.3 - Incident ReportDocument2 pagesHSE-PRO-03-INR 0.3 - Incident ReportSoufian BahmadNo ratings yet
- Incident and Accident Form: UI-61917-PGCC-HSSE-IAF 3.1Document4 pagesIncident and Accident Form: UI-61917-PGCC-HSSE-IAF 3.1benNo ratings yet
- Permit To WorkDocument2 pagesPermit To Worksubhanmusadiq100% (4)
- Protective Cloth PDFDocument1 pageProtective Cloth PDFsubhanmusadiq100% (1)
- Respirator PDFDocument1 pageRespirator PDFsubhanmusadiqNo ratings yet
- No Smoking PDFDocument1 pageNo Smoking PDFsubhanmusadiq100% (1)
- FAC Box PDFDocument1 pageFAC Box PDFsubhanmusadiqNo ratings yet
- Emergency Assembly Point 02 PDFDocument1 pageEmergency Assembly Point 02 PDFsubhanmusadiqNo ratings yet
- Ppe Is Mandatory Beyond This Point PDFDocument1 pagePpe Is Mandatory Beyond This Point PDFsubhanmusadiq100% (1)
- Highly Flammable Materials PDFDocument1 pageHighly Flammable Materials PDFsubhanmusadiqNo ratings yet
- Drinking Water PDFDocument1 pageDrinking Water PDFsubhanmusadiqNo ratings yet
- Lifting Operatio in Progress PDFDocument1 pageLifting Operatio in Progress PDFsubhanmusadiq100% (1)
- Deep Excavation PDFDocument1 pageDeep Excavation PDFsubhanmusadiqNo ratings yet
- Authorized Personnel Only PDFDocument1 pageAuthorized Personnel Only PDFsubhanmusadiq100% (1)
- Emergrncy Assembly Point PDFDocument1 pageEmergrncy Assembly Point PDFsubhanmusadiqNo ratings yet
- Falling Objects PDFDocument1 pageFalling Objects PDFsubhanmusadiqNo ratings yet
- Electricity PDFDocument1 pageElectricity PDFsubhanmusadiqNo ratings yet
- CD463M1 Data SheetDocument1 pageCD463M1 Data SheetsubhanmusadiqNo ratings yet
- Basic Rigging: Annotated Instructor's GuideDocument9 pagesBasic Rigging: Annotated Instructor's GuidesubhanmusadiqNo ratings yet
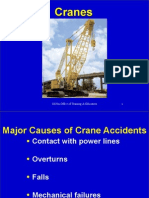
- CranesDocument39 pagesCranesMajji SatishNo ratings yet
- Toyo - Electric Chain HoistDocument6 pagesToyo - Electric Chain HoistsubhanmusadiqNo ratings yet
- BSA Alert 13.69 Fall of Materials From ScaffoldingDocument1 pageBSA Alert 13.69 Fall of Materials From ScaffoldingsubhanmusadiqNo ratings yet
- Candidate Handbook: National Commission For The Certification of Crane Operators (Nccco)Document40 pagesCandidate Handbook: National Commission For The Certification of Crane Operators (Nccco)subhanmusadiqNo ratings yet
- Employee Training: Facility Name: NPDES Permit NumberDocument2 pagesEmployee Training: Facility Name: NPDES Permit NumbersubhanmusadiqNo ratings yet
- Driver Evaluation FormDocument1 pageDriver Evaluation Formsubhanmusadiq100% (2)
- HH:MM Dd/Mm/Yyy Y HH:MM Dd/Mm/Yyy Y Name / Surname Name / SurnameDocument3 pagesHH:MM Dd/Mm/Yyy Y HH:MM Dd/Mm/Yyy Y Name / Surname Name / Surnamesubhanmusadiq100% (2)
- Section 2.4: Pre-Apprenticeship Training Program Tracking Form 2010-11 Ministry of Training, Colleges and Universities, Service Delivery BranchDocument4 pagesSection 2.4: Pre-Apprenticeship Training Program Tracking Form 2010-11 Ministry of Training, Colleges and Universities, Service Delivery BranchsubhanmusadiqNo ratings yet
- Science SOL 2.4 - Life Processes Notes Terms To KnowDocument2 pagesScience SOL 2.4 - Life Processes Notes Terms To KnowsubhanmusadiqNo ratings yet
- Environmental Monitoring ReportDocument1 pageEnvironmental Monitoring ReportsubhanmusadiqNo ratings yet
- BSA Alert 025 Grinder FatalityDocument1 pageBSA Alert 025 Grinder FatalitysubhanmusadiqNo ratings yet
- Training Record 2Document15 pagesTraining Record 2subhanmusadiqNo ratings yet
- Science SOL 2.3 - Matter Notes Terms To KnowDocument2 pagesScience SOL 2.3 - Matter Notes Terms To KnowsubhanmusadiqNo ratings yet
- Archirodon Group NV Integrated Management System Health, Safety & Environment (HSE)Document1 pageArchirodon Group NV Integrated Management System Health, Safety & Environment (HSE)subhanmusadiqNo ratings yet
- Agricultural BenefitsDocument7 pagesAgricultural BenefitsMa Glenda Rabulan DioquinoNo ratings yet
- Cerc 2014edition PDFDocument462 pagesCerc 2014edition PDFMMontes100% (1)
- Matheson Gas EO SDSDocument8 pagesMatheson Gas EO SDSXiaLUNo ratings yet
- Aqualink PLB SpecificationsDocument2 pagesAqualink PLB SpecificationsGeorge finkleNo ratings yet
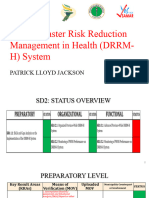
- Building Blocks Presentation - SD2Document13 pagesBuilding Blocks Presentation - SD2Patrick Lloyd JacksonNo ratings yet
- Mapel:Bahasa Inggris: Latihan SoalDocument6 pagesMapel:Bahasa Inggris: Latihan SoalBadaiNo ratings yet
- Department of Education: Narrative and Pictorial Reports On The National School Base Earthquake and Fire Drill 2018-2019Document23 pagesDepartment of Education: Narrative and Pictorial Reports On The National School Base Earthquake and Fire Drill 2018-2019Ser Cyrus75% (4)
- Home Workshop Explosives - Uncle FesterDocument175 pagesHome Workshop Explosives - Uncle FesterJean Tube100% (1)
- The Third Term Exam 2 2ESDocument2 pagesThe Third Term Exam 2 2ESAhcene BouflighaNo ratings yet
- Vision Ias Disaster-Management PDFDocument98 pagesVision Ias Disaster-Management PDFdefotel603No ratings yet
- Comprehensive Inspection FormDocument17 pagesComprehensive Inspection FormbaworsNo ratings yet
- Awis Ti Langenlangen: An Understanding of The Awareness of Isnhs' Stem Students On Responses To EmergencyDocument12 pagesAwis Ti Langenlangen: An Understanding of The Awareness of Isnhs' Stem Students On Responses To EmergencyKristine AsuncionNo ratings yet
- Analysis of Blast Loading Effect On High Rise BuildingsDocument7 pagesAnalysis of Blast Loading Effect On High Rise BuildingsAlexander DeckerNo ratings yet
- SAMPLE: Emergency Response Plan: Minor EmergenciesDocument3 pagesSAMPLE: Emergency Response Plan: Minor EmergenciesCyn SyjucoNo ratings yet
- Rubric Grade 10Document2 pagesRubric Grade 10Christine Joy RamosNo ratings yet
- Disasters and Diseaster ManagementDocument56 pagesDisasters and Diseaster ManagementShimmering Moon100% (1)
- KarnatakaDocument210 pagesKarnatakasudhakarashwithaNo ratings yet
- Show Me How To Survive: The Handbook For The Modern HeroDocument20 pagesShow Me How To Survive: The Handbook For The Modern HeroWeldon Owen Publishing75% (8)
- School Disaster Risk Management PlanningDocument49 pagesSchool Disaster Risk Management PlanningVon TatilNo ratings yet
- 2013HO - MS177 A.P. Cinema Theatre RulesDocument7 pages2013HO - MS177 A.P. Cinema Theatre RulesRaghu RamNo ratings yet
- Inspection of Collapse Cause of Sampoong Department StoreDocument3 pagesInspection of Collapse Cause of Sampoong Department StoreraihanNo ratings yet
- Auditing Data Center & Disaster RecoverDocument42 pagesAuditing Data Center & Disaster RecovernurfallahNo ratings yet
- Emergency Preparedness and Response ManualDocument14 pagesEmergency Preparedness and Response Manualphilip tamang100% (1)
- Risk Assessment For EmergeDocument12 pagesRisk Assessment For EmergeAdel SukerNo ratings yet
- Slide 16 TriageDocument10 pagesSlide 16 TriageSiti Dona IsnaeniNo ratings yet
- Disaster Management - VaibhavDocument27 pagesDisaster Management - Vaibhavvaibhav bhardwajNo ratings yet
- V1 Thornton Heat Bomb AttackDocument1 pageV1 Thornton Heat Bomb Attackchaudhry97No ratings yet
- Rehabilitation Issues and Case Study of Kedarnath LandslideDocument46 pagesRehabilitation Issues and Case Study of Kedarnath Landslidebittumonster5888100% (3)
- Brochure PDFDocument2 pagesBrochure PDFenviromunishNo ratings yet
- Fire Safety & Emergency Evacuation Plan Nicollet Public School Required by Minnesota State Fire CodeDocument5 pagesFire Safety & Emergency Evacuation Plan Nicollet Public School Required by Minnesota State Fire CodeidahssNo ratings yet