You might also like
- Sepsis Update 2018Document32 pagesSepsis Update 2018putri endah100% (1)
- Lactic Acidosis Update For Critical Care CliniciansDocument5 pagesLactic Acidosis Update For Critical Care CliniciansjohjossNo ratings yet
- Rapid Sequence Intubation: BY Budak KecikDocument25 pagesRapid Sequence Intubation: BY Budak KecikAqua ForceNo ratings yet
- ContohDocument4 pagesContohAqua ForceNo ratings yet
- Prevention Cardio CPGDocument63 pagesPrevention Cardio CPGAqua ForceNo ratings yet
- 10 1001@jama 2016 0287Document10 pages10 1001@jama 2016 0287ompardor7554No ratings yet
- Senarai Ho Banjir Medical 2014 PDFDocument4 pagesSenarai Ho Banjir Medical 2014 PDFAqua ForceNo ratings yet
- Rapid Sequence Intubation: BY Budak KecikDocument25 pagesRapid Sequence Intubation: BY Budak KecikAqua ForceNo ratings yet
- Att Letters SecDocument6 pagesAtt Letters SecAqua ForceNo ratings yet
- CampioneDocument1,652 pagesCampioneAqua ForceNo ratings yet
- Preterm Labor DahliaDocument4 pagesPreterm Labor DahliaAqua ForceNo ratings yet
- Absenteeism Letter On Letterhead PDFDocument2 pagesAbsenteeism Letter On Letterhead PDFAqua ForceNo ratings yet
- UK National Guideline For The Management of Pelvic Inflammatory Disease 2011 PDFDocument18 pagesUK National Guideline For The Management of Pelvic Inflammatory Disease 2011 PDFPrissilmaTaniaNo ratings yet
- DfsdfsdfeerberwerberbwerweDocument1 pageDfsdfsdfeerberwerberbwerweAqua ForceNo ratings yet
- Approach To Chest PainDocument17 pagesApproach To Chest PainAqua ForceNo ratings yet
- VDFHGFHF Rtretr GR Df33254Document1 pageVDFHGFHF Rtretr GR Df33254Aqua ForceNo ratings yet
- Timetable For International Program 2012-2013 - Section BDocument1 pageTimetable For International Program 2012-2013 - Section BAqua ForceNo ratings yet
- Coordinator of Six Year Prof Dr/Ahmed TarekDocument1 pageCoordinator of Six Year Prof Dr/Ahmed TarekAqua ForceNo ratings yet
- 243ear TraumaDocument33 pages243ear TraumaAqua ForceNo ratings yet
- NRDSDocument4 pagesNRDSAqua ForceNo ratings yet
- ReadmeDocument7 pagesReadmeLambourghiniNo ratings yet
- Emergency HTNDocument6 pagesEmergency HTNAqua ForceNo ratings yet
- Torrent Downloaded FromDocument1 pageTorrent Downloaded FromAqua ForceNo ratings yet
- Cervicitis and VaginitisDocument18 pagesCervicitis and VaginitisAqua ForceNo ratings yet
- Examples of OSCEDocument2 pagesExamples of OSCEAqua ForceNo ratings yet
- Surgery TopicsDocument1 pageSurgery TopicsAqua ForceNo ratings yet
- Examples of OSCEDocument2 pagesExamples of OSCEAqua ForceNo ratings yet
- Ent Past Years Question According To TopicsDocument32 pagesEnt Past Years Question According To Topicsmohamed100% (1)
- Autoimmune Bullous DermatosesDocument143 pagesAutoimmune Bullous DermatosesAqua ForceNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Sistem Motorik: Penyusun: Willy Wijaya, DR Pembimbing: Henny. A.S, DR, Sps (K)Document26 pagesSistem Motorik: Penyusun: Willy Wijaya, DR Pembimbing: Henny. A.S, DR, Sps (K)Novi Fatni MNo ratings yet
- VentrikulomegaliDocument2 pagesVentrikulomegaliAida NurwidyaNo ratings yet
- Diabetic NeuropathyDocument21 pagesDiabetic NeuropathyMargaretta RambuNo ratings yet
- Gait Speed 4Document30 pagesGait Speed 4api-545157726No ratings yet
- Extrapyramidal SyndromeDocument12 pagesExtrapyramidal SyndromeZahra Namika AiharaNo ratings yet
- Aaron Cohen-Gadol CVDocument41 pagesAaron Cohen-Gadol CVBilly UntuNo ratings yet
- Electrographic and Electroclinical Seizures BirdsDocument50 pagesElectrographic and Electroclinical Seizures BirdsNEUROMED NEURONo ratings yet
- The Role of Intratympanic Dexamethasone in Sudden Sensorineural Hearing LossDocument5 pagesThe Role of Intratympanic Dexamethasone in Sudden Sensorineural Hearing LossAditya HendraNo ratings yet
- Aphasia Rehabilitation - More Than Treating The Language Disorder PDFDocument3 pagesAphasia Rehabilitation - More Than Treating The Language Disorder PDFaramath7No ratings yet
- RorschachbookDocument8 pagesRorschachbookAynur XosrəviNo ratings yet
- Raised Intracranial PressureDocument6 pagesRaised Intracranial PressureindihimmakhairaniNo ratings yet
- Mathew Strake ScaleDocument2 pagesMathew Strake ScaleAbdur RasyidNo ratings yet
- Chapter62-Management of Patients With Cerebrovascular DisordersDocument35 pagesChapter62-Management of Patients With Cerebrovascular DisordersAhmed 123100% (1)
- Neurological AssessmentDocument47 pagesNeurological AssessmentRian TheredNo ratings yet
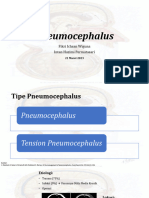
- PneumocephalusDocument12 pagesPneumocephalusFikri IchsanNo ratings yet
- Neuropsicologia y Epilepsia - J. Campos-Castelló A, S. Campos-SolerDocument12 pagesNeuropsicologia y Epilepsia - J. Campos-Castelló A, S. Campos-SolerVicente ArellanoNo ratings yet
- Gait Problems in Cerebellar AtaxiaDocument4 pagesGait Problems in Cerebellar AtaxiaWasemBhatNo ratings yet
- 4 Tips For Passing PACES: PreparationDocument10 pages4 Tips For Passing PACES: PreparationAhmed AbdelgelilNo ratings yet
- Hyperkinetic Movement DisordersDocument209 pagesHyperkinetic Movement DisordersRaluca-Andreea Ignat100% (1)
- StokesGrosofsky - Case Study StudentsDocument13 pagesStokesGrosofsky - Case Study StudentsSimmy Dhaliwal0% (1)
- Neuromyelitis Optica Spectrum Disorder and Other.15Document30 pagesNeuromyelitis Optica Spectrum Disorder and Other.15Doaa Mokhtar100% (1)
- Emotion Perception 2Document14 pagesEmotion Perception 2Juan Camilo Sánchez AriasNo ratings yet
- ENT BCQsDocument19 pagesENT BCQsSajid AliNo ratings yet
- Chapter 257: Head Trauma: Introduction and EpidemiologyDocument35 pagesChapter 257: Head Trauma: Introduction and EpidemiologyIustitia Septuaginta SambenNo ratings yet
- Bonicas Management of Pain 5th Edition Ebook PDFDocument61 pagesBonicas Management of Pain 5th Edition Ebook PDFpaul.tucker16998% (41)
- Amyotrophic Lateral SclerosisDocument58 pagesAmyotrophic Lateral SclerosisAathi PathmanathanNo ratings yet
- CNS TumorDocument32 pagesCNS TumorBbem ooNo ratings yet
- Tic DoulrexDocument7 pagesTic DoulrexGaurav ChakrabartyNo ratings yet
- Headache and Neck PainDocument3 pagesHeadache and Neck PainKelly BatesNo ratings yet
- Sacks LevodopaDocument3 pagesSacks LevodopaGabriel MaxNo ratings yet