You might also like
- DR - Mohsen.sacroiliac Joint Dysfunction and Piriformis Syndrome The Complete Guide For Physical TherapistsDocument407 pagesDR - Mohsen.sacroiliac Joint Dysfunction and Piriformis Syndrome The Complete Guide For Physical TherapistsAlina100% (5)
- Sacroiliac Joint SyndromeDocument4 pagesSacroiliac Joint SyndromeAnastasia Martha83% (6)
- The Complete Guide To Trigger Points & Myofascial Pain (2016)Document35 pagesThe Complete Guide To Trigger Points & Myofascial Pain (2016)salmazz50% (2)
- Unit Color Compendium 1702 Double PagesDocument144 pagesUnit Color Compendium 1702 Double PagesStarslayer RNC100% (3)
- Sacroiliac Joint Dysfunction and Piriformis Syndrome PDFDocument37 pagesSacroiliac Joint Dysfunction and Piriformis Syndrome PDFDevi SiswaniNo ratings yet
- Sajida Bibi Noonari Lecturer at National Institute of Physiotherapy Rehabilitation and MedicineDocument46 pagesSajida Bibi Noonari Lecturer at National Institute of Physiotherapy Rehabilitation and MedicineSajida Bibi NoonariNo ratings yet
- Travell and Simons' Trigger Point Flip Charts - Janet TravellDocument4 pagesTravell and Simons' Trigger Point Flip Charts - Janet Travellxipigepy100% (1)
- Bodywise: How Manual Therapy Helps Us Recover from Illness & Injuries & Stay Healthy, Without Drugs or SurgeryFrom EverandBodywise: How Manual Therapy Helps Us Recover from Illness & Injuries & Stay Healthy, Without Drugs or SurgeryNo ratings yet
- Biomechanics of Foot and AnkleDocument34 pagesBiomechanics of Foot and AnkleKanwal KhanNo ratings yet
- SI Joint Dysfunction Treatment Protocols: Presenter NotesDocument15 pagesSI Joint Dysfunction Treatment Protocols: Presenter NotesMichel BakkerNo ratings yet
- SI Joint Dysfunction Treatment Protocols: Presenter NotesDocument15 pagesSI Joint Dysfunction Treatment Protocols: Presenter NotesMichel BakkerNo ratings yet
- Sacroiliac Joint DysfunctionDocument9 pagesSacroiliac Joint DysfunctionJaved KhanNo ratings yet
- Hip Joint Complex: Aneena Alex MPT Ist Year MtimsDocument38 pagesHip Joint Complex: Aneena Alex MPT Ist Year MtimsNaroashNo ratings yet
- Sacroiliac Joint Exercises For Back Pain ReliefDocument13 pagesSacroiliac Joint Exercises For Back Pain ReliefSam Visnic100% (1)
- Gait Analysis: Prerequisite of Normal GaitDocument4 pagesGait Analysis: Prerequisite of Normal GaitKieran Levi100% (1)
- 24 Top Orthopedic TestsDocument29 pages24 Top Orthopedic TestsDavid Gal100% (1)
- Muscles Testing and Function PDFDocument1 pageMuscles Testing and Function PDFSundar Prabhu0% (3)
- Kinesiology Taping Theory and ApplicationDocument8 pagesKinesiology Taping Theory and Applicationtaxel00% (1)
- The Asymmetric Pelvis: Liz Gaggini, M.ADocument7 pagesThe Asymmetric Pelvis: Liz Gaggini, M.Aleo100% (1)
- Functional Neuromuscular AnatomyDocument56 pagesFunctional Neuromuscular AnatomyΒασίλης Βασιλείου100% (3)
- Manual Therapy Summary ANKLE FOOTDocument32 pagesManual Therapy Summary ANKLE FOOTnataleebella100% (2)
- Fascial Manipulation (Brief Introduction)Document6 pagesFascial Manipulation (Brief Introduction)tvbuddy123100% (1)
- Workbook 031512 With Cover PDFDocument197 pagesWorkbook 031512 With Cover PDFIndah Yulantari100% (2)
- 5.6 Muscle Energy Techniques For The Pelvis 167-171Document5 pages5.6 Muscle Energy Techniques For The Pelvis 167-171maricartiNo ratings yet
- Low Back PainDocument100 pagesLow Back Painchandrusai100% (1)
- CWK en DemoDocument16 pagesCWK en DemoVishal YogiNo ratings yet
- Postural Assessment ToolDocument2 pagesPostural Assessment Toolwanna_run_faster100% (3)
- Hand and Wrist InjuriesDocument25 pagesHand and Wrist InjuriesMAMA LALA100% (2)
- Muscle Energy Techniques Pt1Document22 pagesMuscle Energy Techniques Pt1vs_3457000100% (5)
- The Cervical & Thoracic Spine Mechanical Diagnosis & Therapy - Vol 1Document313 pagesThe Cervical & Thoracic Spine Mechanical Diagnosis & Therapy - Vol 1Eduardo Batista100% (10)
- Spinal TractionDocument37 pagesSpinal TractionDibyendunarayan BidNo ratings yet
- ART METS Strain-CounterstrainDocument14 pagesART METS Strain-CounterstrainPhysiotherapist Ali0% (1)
- Chiropractic Line AnalysisDocument10 pagesChiropractic Line AnalysisD N BidNo ratings yet
- A Comprehensive Treatment Guide For Frozen ShoulderDocument15 pagesA Comprehensive Treatment Guide For Frozen ShoulderHoan TrầnNo ratings yet
- Angela Hand and Upper ExtremityDocument59 pagesAngela Hand and Upper ExtremityJenny RajanNo ratings yet
- Clinical Hip ExaminationDocument90 pagesClinical Hip ExaminationalmaformaNo ratings yet
- Rotator Cuff Tears Orthoinfo - Aaos.org TopicDocument7 pagesRotator Cuff Tears Orthoinfo - Aaos.org TopicMontserrat LandaNo ratings yet
- Manual Therapy: DR - DharmavatiDocument78 pagesManual Therapy: DR - DharmavatiHitesh RohitNo ratings yet
- Biomechanics of The Knee During Closed Kinetic Chain ExercisesDocument31 pagesBiomechanics of The Knee During Closed Kinetic Chain ExercisesJean SantosNo ratings yet
- Trigger Point Chart Set: Torso & Extremities Paper - Anatomical Chart CompanyDocument4 pagesTrigger Point Chart Set: Torso & Extremities Paper - Anatomical Chart Companyfesyzyzu100% (1)
- Westside For Skinny Bastards, Part III: The Final ChapterDocument20 pagesWestside For Skinny Bastards, Part III: The Final ChapterMichel BakkerNo ratings yet
- Life of Pi Characters PDFDocument4 pagesLife of Pi Characters PDFAwang Q AmaikNo ratings yet
- Lumbopelvic Stability: SyllabusDocument13 pagesLumbopelvic Stability: Syllabusrapannika100% (3)
- Guitar Songs ListDocument72 pagesGuitar Songs Listsandeep0% (2)
- Sports Medicine Specialists Rehabilitation ProtocolsDocument59 pagesSports Medicine Specialists Rehabilitation ProtocolsThe Homie100% (2)
- Examination of Bone and Joint PathologyDocument89 pagesExamination of Bone and Joint PathologyMuhammad Thahir100% (1)
- Frozen Shoulder Whitney Lowe Massage MagDocument4 pagesFrozen Shoulder Whitney Lowe Massage Magwolfgangl70No ratings yet
- External Hip Rotator StretchDocument15 pagesExternal Hip Rotator StretchvishnuselvaNo ratings yet
- Tendon Problems in Athletic IndividualsDocument15 pagesTendon Problems in Athletic IndividualsMuhammadskNo ratings yet
- Clinical NeurodynamicsDocument41 pagesClinical Neurodynamicsramesh2007-mptNo ratings yet
- Palpation of Bony LandmarksDocument4 pagesPalpation of Bony LandmarksNur Ashriawati BurhanNo ratings yet
- Mulligan Concept of Manual TherapyDocument2 pagesMulligan Concept of Manual TherapySuMitra MohaNtyNo ratings yet
- The Rotator Cuff (Myofascial Techniques)Document4 pagesThe Rotator Cuff (Myofascial Techniques)Advanced-Trainings.com100% (3)
- Rotator Cuff Tear: Nurul Sahida Dina Fadhilah Monika MaghfiraDocument26 pagesRotator Cuff Tear: Nurul Sahida Dina Fadhilah Monika Maghfiradila_innongNo ratings yet
- Compton - PsoasDocument25 pagesCompton - PsoasiruizmolinaNo ratings yet
- Poor Posture, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandPoor Posture, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- 02advancedthinkahead2 Xprac Mod4bDocument2 pages02advancedthinkahead2 Xprac Mod4bNoemí Tejada Muñoz100% (1)
- Static Palpation of The Spine FINALDocument13 pagesStatic Palpation of The Spine FINALPrathap KumarNo ratings yet
- Dental Equilibration and OsteopathyDocument9 pagesDental Equilibration and OsteopathyshivnairNo ratings yet
- Temporomandibular Joint DysfunctionDocument11 pagesTemporomandibular Joint Dysfunctionr.boniver524No ratings yet
- Joint Mobilization: Lee Rosenzweig, PT, DPT, CHTDocument14 pagesJoint Mobilization: Lee Rosenzweig, PT, DPT, CHTAditya RanjanNo ratings yet
- TMJDocument33 pagesTMJMohamed Magdy El Meligie100% (2)
- Lumbar Instability Ands Exercises 2000Document11 pagesLumbar Instability Ands Exercises 2000Francisco Javier Quinteros GarcíaNo ratings yet
- The Pain Catastrophizing Scale: User ManualDocument36 pagesThe Pain Catastrophizing Scale: User ManualAlina Isabela CurtNo ratings yet
- Case Report - Low Back BainDocument2 pagesCase Report - Low Back BainMichel BakkerNo ratings yet
- IFOMPT Examination Cervical Spine Doc September 2012 DefinitiveDocument37 pagesIFOMPT Examination Cervical Spine Doc September 2012 DefinitiveMichel BakkerNo ratings yet
- Manual Therapy: David W. Evans, Nicholas LucasDocument6 pagesManual Therapy: David W. Evans, Nicholas LucasMichel BakkerNo ratings yet
- Filip D - Kineclub 2011 Herkennen CSDocument8 pagesFilip D - Kineclub 2011 Herkennen CSMichel BakkerNo ratings yet
- Wedel SIGDocument120 pagesWedel SIGMichel BakkerNo ratings yet
- Sacrum Self Study GuideDocument24 pagesSacrum Self Study GuideMichel BakkerNo ratings yet
- Book of Abstracts Mulligan MCTA Porto Conference 2011Document89 pagesBook of Abstracts Mulligan MCTA Porto Conference 2011Michel BakkerNo ratings yet
- Bekken. Load Transfer TestsDocument6 pagesBekken. Load Transfer TestsMichel BakkerNo ratings yet
- Anchoring Script-Haryana DayDocument5 pagesAnchoring Script-Haryana Dayrashmi pahelNo ratings yet
- Final Exam Basico 5 EFDocument5 pagesFinal Exam Basico 5 EFJULIO CHRISTIAN RAMIREZ VARGASNo ratings yet
- Independent and Dependent EventsDocument4 pagesIndependent and Dependent Eventsapi-314332531No ratings yet
- Acer BIOS Update InstructionsDocument6 pagesAcer BIOS Update InstructionsZachary MolinaNo ratings yet
- Key Blank Directory 12 Cross Reference Sec 10Document45 pagesKey Blank Directory 12 Cross Reference Sec 10Chuck ChongNo ratings yet
- Anh 6 GK 2 de 1Document4 pagesAnh 6 GK 2 de 1Dương Nguyễn ThùyNo ratings yet
- GameDocument2 pagesGameFadil IddleNo ratings yet
- Esio TrotDocument4 pagesEsio TrotThe GisseStyleNo ratings yet
- MU278 Exam 9Document2 pagesMU278 Exam 9Zedenia FernandezNo ratings yet
- Kyme9N: Flight 1 Departing ArrivingDocument1 pageKyme9N: Flight 1 Departing ArrivingSRI GURU GANESH TRAVELSNo ratings yet
- Wa0004.Document3 pagesWa0004.sumantkumar2.palNo ratings yet
- E Ticket 2Document1 pageE Ticket 2Rumi AcademicNo ratings yet
- TheaterDocument2 pagesTheaterJose Emmanuel LutraniaNo ratings yet
- Tourism Awareness and Tour GuidingDocument25 pagesTourism Awareness and Tour GuidingAnnalyn PeñaNo ratings yet
- Prepositions of PlaceDocument2 pagesPrepositions of PlaceicecrisNo ratings yet
- TRI105.DTA .002 Veefil-PK350-SpecificationsDocument3 pagesTRI105.DTA .002 Veefil-PK350-SpecificationsCarlos AndradeNo ratings yet
- Lesson Plan Number 2Document10 pagesLesson Plan Number 2Magali MeacaNo ratings yet
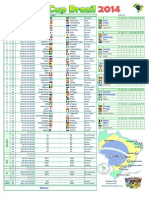
- Jadual World Cup 2014 Waktu MalaysiaDocument1 pageJadual World Cup 2014 Waktu MalaysiamrdanNo ratings yet
- 3 Bup 2 EvDocument11 pages3 Bup 2 EvcladelolNo ratings yet
- Lesson 4Document8 pagesLesson 4Sheena Mae Po100% (1)
- Run All These Below Scripts On Your Oracle Schema So That You Can Use This Data For All Your Lab ExercisesDocument4 pagesRun All These Below Scripts On Your Oracle Schema So That You Can Use This Data For All Your Lab ExercisesKatie RuizNo ratings yet
- Soldiers of Christ AriseDocument2 pagesSoldiers of Christ AriseRodrigo LuisNo ratings yet
- Monteverdi and Orfeo PDFDocument34 pagesMonteverdi and Orfeo PDFEdgarJaredFloresCoboNo ratings yet
- Computer Hardware: COMPSCI 111 SC - Lecture 1Document3 pagesComputer Hardware: COMPSCI 111 SC - Lecture 1grace bulawitNo ratings yet
- AME ReleaseDocument18 pagesAME Releasevjkos81No ratings yet
- List of Hindi Karaoke Songs AvailableDocument14 pagesList of Hindi Karaoke Songs Availableapi-19980524No ratings yet