You might also like
- The HDL Handbook: Biological Functions and Clinical ImplicationsFrom EverandThe HDL Handbook: Biological Functions and Clinical ImplicationsNo ratings yet
- Raising HDL Cholesterol in Women - 111709 PDFDocument11 pagesRaising HDL Cholesterol in Women - 111709 PDFDina Aulia FakhrinaNo ratings yet
- Abstract and IntroductionDocument14 pagesAbstract and Introductiondavid_lg6179No ratings yet
- Medical TerminologyDocument17 pagesMedical TerminologySofia Isabelle GarciaNo ratings yet
- HDL in CKD-ThesisDocument27 pagesHDL in CKD-ThesisEndy SusenoNo ratings yet
- Case Study: Chapter 35: Agents Used in DyslipidemiaDocument28 pagesCase Study: Chapter 35: Agents Used in DyslipidemiaNguyen Huu TinNo ratings yet
- Mechanism of Action of Fibrates On Lipid and Lipoprotein MetabolismDocument7 pagesMechanism of Action of Fibrates On Lipid and Lipoprotein MetabolismNava AlisiaNo ratings yet
- Lifestyle Factors and Pharmacological Agents That Manage Hyperlipidemia Through Activation of Peroxisome Proliferator Activated ReceptorsDocument16 pagesLifestyle Factors and Pharmacological Agents That Manage Hyperlipidemia Through Activation of Peroxisome Proliferator Activated ReceptorsjebacNo ratings yet
- Markel 2011 - The Resurgence of Niacin, From Nicotinic Acid To NiaspanlaropiprantDocument7 pagesMarkel 2011 - The Resurgence of Niacin, From Nicotinic Acid To NiaspanlaropiprantAlbert CalvetNo ratings yet
- Farmakoterapi DislipidemiaDocument52 pagesFarmakoterapi DislipidemialisaNo ratings yet
- Srikant H 2016Document10 pagesSrikant H 2016aditya sekarNo ratings yet
- 2049 3614 Ec 21 0002Document15 pages2049 3614 Ec 21 0002Aura NirwanaNo ratings yet
- Disorders of Lipid Metabolism LectureDocument55 pagesDisorders of Lipid Metabolism LectureRichard SiahaanNo ratings yet
- Medical Nutrition Therapy For Cardiovascular DiseaseDocument210 pagesMedical Nutrition Therapy For Cardiovascular DiseaseBok MatthewNo ratings yet
- Dyslipidemia 140710032036 Phpapp01Document90 pagesDyslipidemia 140710032036 Phpapp01Elena EllaNo ratings yet
- Beyond Low Density in CholesterolDocument8 pagesBeyond Low Density in CholesterolenriqueavilazamoraNo ratings yet
- 1 s2.0 S266637912030001X MainDocument13 pages1 s2.0 S266637912030001X MainPhạm SỉNo ratings yet
- Dyslipidemia in Patients With Thyroid Disorders: Evagelos N Liberopoulos, Moses S ElisafDocument6 pagesDyslipidemia in Patients With Thyroid Disorders: Evagelos N Liberopoulos, Moses S ElisafBunPământNo ratings yet
- 1.HDL-a Therapeutic TargetDocument8 pages1.HDL-a Therapeutic TargetAshraf ChowdhuryNo ratings yet
- Presentation - LipoproteinDocument31 pagesPresentation - Lipoproteinrahulshrmaa2222No ratings yet
- HDL Muy Alto 2019Document10 pagesHDL Muy Alto 2019Luis C Ribon VNo ratings yet
- Biomarker 3Document7 pagesBiomarker 3Raluca Andreea AxinteNo ratings yet
- Atherosclerosis, Dyslipidaemia and Diabetes SlidesDocument83 pagesAtherosclerosis, Dyslipidaemia and Diabetes SlidesTatiana GobjilăNo ratings yet
- Effects of Dietary Flavonoids On Reverse Cholesterol Transport, HDL Metabolism, and HDL FunctionDocument14 pagesEffects of Dietary Flavonoids On Reverse Cholesterol Transport, HDL Metabolism, and HDL FunctionYoungFanjiensNo ratings yet
- Toward A Higher Standard: Raising HDL in Clinical PracticeDocument11 pagesToward A Higher Standard: Raising HDL in Clinical PracticeAlexandre Sant'AnaNo ratings yet
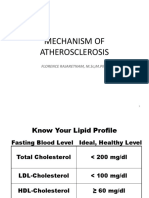
- Lipid ProfileDocument23 pagesLipid Profilekyawswakyawswa100% (1)
- Notes Chapter 35Document16 pagesNotes Chapter 35Christene GVNo ratings yet
- A Hyper - Emia A A PseudohyponatremiaDocument14 pagesA Hyper - Emia A A PseudohyponatremiaSrinivas PolikepatiNo ratings yet
- Meningkatkan Kolesterol HDL Paradigma Baru Dalam Pencegahan Penyakit KardiovaskularDocument10 pagesMeningkatkan Kolesterol HDL Paradigma Baru Dalam Pencegahan Penyakit KardiovaskularMega RatnasariNo ratings yet
- Management of HyperlipidemiaDocument34 pagesManagement of HyperlipidemiaCarleta StanNo ratings yet
- Pharmacology & Therapeutics: Anette Varbo, Marianne Benn, Børge G. NordestgaardDocument10 pagesPharmacology & Therapeutics: Anette Varbo, Marianne Benn, Børge G. NordestgaardIonuț CozmaNo ratings yet
- Caso Clinico 30Document8 pagesCaso Clinico 30Ariel SanNo ratings yet
- Familial Hypercholesterolemia Nota10 Idioma AnglesDocument4 pagesFamilial Hypercholesterolemia Nota10 Idioma AnglesMarina RamirezNo ratings yet
- Clinical Cardiology - October 1987 - Wolinsky - The Effects of Beta Adrenergic Blocking Agents On Blood Lipid LevelsDocument6 pagesClinical Cardiology - October 1987 - Wolinsky - The Effects of Beta Adrenergic Blocking Agents On Blood Lipid LevelsSrinivasa RaghavanNo ratings yet
- LipidDocument31 pagesLipidahmed abd elazizNo ratings yet
- Dyslipidemia in Renal DiseaseDocument9 pagesDyslipidemia in Renal DiseasealfonsomhNo ratings yet
- Samuel VinhoDocument5 pagesSamuel Vinhosamuel rangelNo ratings yet
- Review: S. E. Borggreve, R. de Vries and R. P. F. DullaartDocument19 pagesReview: S. E. Borggreve, R. de Vries and R. P. F. DullaartFCiênciasNo ratings yet
- Bandeali-Farmer2012 Article High-DensityLipoproteinAndAtheDocument7 pagesBandeali-Farmer2012 Article High-DensityLipoproteinAndAtheDainius JakubauskasNo ratings yet
- Effect of Diuretics On The Plasma Lipid Profile: KEY WORDS: Hypertension, Diuretics, Dyslipidaemia, Glucose IntoleranceDocument7 pagesEffect of Diuretics On The Plasma Lipid Profile: KEY WORDS: Hypertension, Diuretics, Dyslipidaemia, Glucose IntoleranceVims BatchNo ratings yet
- Chen-2012-The Effects of Jiang-Zhi-Ning and ItDocument10 pagesChen-2012-The Effects of Jiang-Zhi-Ning and ItSven SchröderNo ratings yet
- Efficacy and Safety of High-Density Lipoprotein Cholesterol-Increasing CompoundsDocument13 pagesEfficacy and Safety of High-Density Lipoprotein Cholesterol-Increasing CompoundsAdityasekar WangiNo ratings yet
- Clase 1. Lipoproteins and Fatty Acids in CKD Molecular and Metabolic AlterationsDocument15 pagesClase 1. Lipoproteins and Fatty Acids in CKD Molecular and Metabolic Alterationsdulce orozcoNo ratings yet
- Original Article: Zvyagintseva TD, Glushchenko SVDocument4 pagesOriginal Article: Zvyagintseva TD, Glushchenko SVHironmoy RoyNo ratings yet
- Pownall 2021Document12 pagesPownall 2021AldoNo ratings yet
- R Mechanism of AtherosclerosisDocument41 pagesR Mechanism of AtherosclerosisAmanuel MaruNo ratings yet
- Plasma Lipid and Coronary Heart DiseaseDocument6 pagesPlasma Lipid and Coronary Heart Diseaseukosam10No ratings yet
- Biochemistry LipoproteinDocument84 pagesBiochemistry LipoproteiniqiqiqiqiqNo ratings yet
- 13 FullDocument16 pages13 FullGyse LemaNo ratings yet
- Familial Hypercholesterolemia: Gourav Kumar M.Sc. Biotech Second Sem 2 207Document43 pagesFamilial Hypercholesterolemia: Gourav Kumar M.Sc. Biotech Second Sem 2 207Gourav Kumar SinhaNo ratings yet
- Chapter 26Document33 pagesChapter 26raul sinatoNo ratings yet
- Triglyceride Profile in Dyslipidaemia of Type 2 Diabetes MellitusDocument4 pagesTriglyceride Profile in Dyslipidaemia of Type 2 Diabetes MellitusTanveerNo ratings yet
- Alcohol MetabolismDocument2 pagesAlcohol MetabolismVincent MwirigiNo ratings yet
- Atherosclerosis, Dyslipidaemia and Diabetes SlidesDocument83 pagesAtherosclerosis, Dyslipidaemia and Diabetes SlidesWee DaliNo ratings yet
- Case Study 2 MNTDocument11 pagesCase Study 2 MNTapi-242547654No ratings yet
- Cvs4-Clinical Aspects of Serum Cholesterol LevelDocument2 pagesCvs4-Clinical Aspects of Serum Cholesterol LevelGabriella ChafrinaNo ratings yet
- Popa2009 PDFDocument6 pagesPopa2009 PDFHeinz FischerNo ratings yet
- Secondary Causes of DyslipidemiaDocument3 pagesSecondary Causes of DyslipidemiaAnghelo Aldair Velásquez CarrilloNo ratings yet
- Bpjv07i02p399 409Document12 pagesBpjv07i02p399 409PNo ratings yet
- Nonparametric Correlations: Lampiran 6Document2 pagesNonparametric Correlations: Lampiran 6RainolNo ratings yet
- Fisiologi Hormon Baru - 1Document73 pagesFisiologi Hormon Baru - 1RainolNo ratings yet
- Andre Rjaset Gadung 2854-2860Document7 pagesAndre Rjaset Gadung 2854-2860RainolNo ratings yet
- Analysis and Identification of Phenolic Compounds in Dioscorea Hispida DennstDocument14 pagesAnalysis and Identification of Phenolic Compounds in Dioscorea Hispida DennstRainolNo ratings yet
- Analysis and Identification of Phenolic Compounds in Dioscorea Hispida DennstDocument14 pagesAnalysis and Identification of Phenolic Compounds in Dioscorea Hispida DennstRainolNo ratings yet
- v70 58Document7 pagesv70 58RainolNo ratings yet
- Pathway BronkopneumoniDocument1 pagePathway BronkopneumoniRainolNo ratings yet
- Thyroid Hormone 2013Document49 pagesThyroid Hormone 2013RainolNo ratings yet
- J. Lipid Res. 1984 Eisenberg 1017 58Document42 pagesJ. Lipid Res. 1984 Eisenberg 1017 58RainolNo ratings yet
- J. Lipid Res. 1984 Eisenberg 1017 58Document42 pagesJ. Lipid Res. 1984 Eisenberg 1017 58RainolNo ratings yet
- HDL Classification SlidesDocument20 pagesHDL Classification SlidesRainolNo ratings yet
- "A Comparative Study To Assess Knowledge and Practice On Cardio Pulmonary Resuscitation Among Icu/Ccu NursesDocument21 pages"A Comparative Study To Assess Knowledge and Practice On Cardio Pulmonary Resuscitation Among Icu/Ccu NursesPushpa ChhillarNo ratings yet
- Top 10 Takeaways Clinicians - UpdatedDocument1 pageTop 10 Takeaways Clinicians - UpdatedBea Barbara CarrascalNo ratings yet
- Dwnload Full Little and Falaces Dental Management of The Medically Compromised Patient 8th Edition Little Test Bank PDFDocument36 pagesDwnload Full Little and Falaces Dental Management of The Medically Compromised Patient 8th Edition Little Test Bank PDFdanagarzad90y100% (10)
- Histamine and Anti HistaminesDocument12 pagesHistamine and Anti HistaminesshrikantNo ratings yet
- A Patient With Altered Mental StatusDocument51 pagesA Patient With Altered Mental StatusSolomon Seth SallforsNo ratings yet
- Biliary Tract Surgery 2008, Vol.88, Issues 6Document292 pagesBiliary Tract Surgery 2008, Vol.88, Issues 6Barbero JuanNo ratings yet
- PritikinDocument15 pagesPritikinpatobotero043No ratings yet
- Pharmacy Preceptors Guild of The Philippines: InstructionsDocument2 pagesPharmacy Preceptors Guild of The Philippines: InstructionsCarline ScarletNo ratings yet
- Smoking EffectsDocument7 pagesSmoking EffectstsikiNo ratings yet
- 011 ReviewDocument26 pages011 ReviewSoad ShedeedNo ratings yet
- Ekokardiografi Dasar WS SCUDocument55 pagesEkokardiografi Dasar WS SCUAdi PrabowoNo ratings yet
- Internal Medicine in Training Exam IM ITE ObjectivesDocument7 pagesInternal Medicine in Training Exam IM ITE ObjectivesPisica ZmeuNo ratings yet
- Thesis On Coronary Artery DiseaseDocument7 pagesThesis On Coronary Artery Diseasesherielliottbillings100% (1)
- Hipertensi Dan Krisis HipertensiDocument26 pagesHipertensi Dan Krisis Hipertensiseptian_tjayaNo ratings yet
- Lithium: Mimicry, Mania, and Muscle Relaxants: Simon Flood MRCP FRCA Andrew Bodenham FRCADocument4 pagesLithium: Mimicry, Mania, and Muscle Relaxants: Simon Flood MRCP FRCA Andrew Bodenham FRCARizwan AhmedNo ratings yet
- Material Mini NetterDocument21 pagesMaterial Mini NetterVALENTINA ALBORNOZ BASTÍASNo ratings yet
- ICCFEP, Falla Renal, 2021Document11 pagesICCFEP, Falla Renal, 2021GeovannaHGNo ratings yet
- Clinical Pathway ACSDocument7 pagesClinical Pathway ACSherrerachaimNo ratings yet
- GIT Cont 071628Document51 pagesGIT Cont 071628Olatomide OlaniranNo ratings yet
- Medical Health Examination FormDocument4 pagesMedical Health Examination FormAldwin Bagtas0% (1)
- Pathophysiology of Congestive Heart FailureDocument2 pagesPathophysiology of Congestive Heart FailureTrixia Almendral100% (2)
- Nej Mo A 2208391Document11 pagesNej Mo A 2208391Melchor Alcántara BarreraNo ratings yet
- Moyamoya DiseaseDocument12 pagesMoyamoya DiseaseFarida Irawati SiregarNo ratings yet
- Kidney Stones: An IntroductionDocument3 pagesKidney Stones: An IntroductionSisti AninditaNo ratings yet
- Listening Scripts: Unit 1Document7 pagesListening Scripts: Unit 1Kami MagNo ratings yet
- Palpitation:evaluation, Ambulatory Monitoring, Mobile Telemetry Eg - MCOT@2012Document19 pagesPalpitation:evaluation, Ambulatory Monitoring, Mobile Telemetry Eg - MCOT@2012Navojit ChowdhuryNo ratings yet
- Wrist Blood Pressure Monitor: HEM-6161 Instruction ManualDocument2 pagesWrist Blood Pressure Monitor: HEM-6161 Instruction ManualRicky Pretta PamiNo ratings yet
- The Strawberry Tongue: What, How and WhereDocument6 pagesThe Strawberry Tongue: What, How and WhereVasishta NadellaNo ratings yet
- Panre and Pance Review Cardiovascular IIDocument26 pagesPanre and Pance Review Cardiovascular IIThe Physician Assistant Life100% (1)
- Abdominal ExaminationDocument16 pagesAbdominal ExaminationLana IbrahimNo ratings yet