You might also like
- Toxicology Course Outline - CompletedDocument4 pagesToxicology Course Outline - Completedtpetronellah mandishona100% (1)
- ParagisDocument15 pagesParagisNeil Francel D. MangilimanNo ratings yet
- Hospital PharmacyDocument100 pagesHospital PharmacySyeda Eshaal JavaidNo ratings yet
- Pharm Care 4 Chapter 1Document25 pagesPharm Care 4 Chapter 1MaraNagaSambarani100% (1)
- Introduction to Dispensing in the PhilippinesDocument30 pagesIntroduction to Dispensing in the PhilippinesRoselyn DawongNo ratings yet
- PH Chem 1Document10 pagesPH Chem 1Starlyn Jonalee Amarillo Alger50% (2)
- 2010 Preliminary Round Case Answer KeyDocument23 pages2010 Preliminary Round Case Answer KeyrefNo ratings yet
- PHR Epp Course Plan - Dohpd PacopDocument4 pagesPHR Epp Course Plan - Dohpd PacopIvan GeromeNo ratings yet
- Individual Prescription Order SystemDocument2 pagesIndividual Prescription Order SystemMeem Abdullah Azeem 1813455049No ratings yet
- Hospital and Its OrganizationsDocument11 pagesHospital and Its Organizationssaloni patel100% (1)
- VaccineDocument72 pagesVaccineSiddharth Shekhar SinghNo ratings yet
- Hospital pharmacy journal insightsDocument7 pagesHospital pharmacy journal insightsMa Victoria ChuaNo ratings yet
- Household Poisnous MaterialsDocument4 pagesHousehold Poisnous MaterialsTarfha AbduhalimNo ratings yet
- Legal Pharm Course OutlineDocument69 pagesLegal Pharm Course OutlineLysa VeeNo ratings yet
- Good Dispensing PracticeDocument59 pagesGood Dispensing Practicechalii100% (1)
- Pharmacognosy Prelim ExperimentsDocument18 pagesPharmacognosy Prelim ExperimentsMello Diax100% (1)
- Pharmaceutical Analysis I - TheoryDocument3 pagesPharmaceutical Analysis I - TheoryHarit0% (1)
- Pharmacists Role Clinical Pharmacokinetic MonitoringDocument2 pagesPharmacists Role Clinical Pharmacokinetic MonitoringauliaNo ratings yet
- B. Informatics (Slides 1-66)Document7 pagesB. Informatics (Slides 1-66)Chrissy LayugNo ratings yet
- Ama Namin by Barbie Dumlao SatbDocument8 pagesAma Namin by Barbie Dumlao SatbLou Andrae G. SantosNo ratings yet
- Documentation Pharmaceutical Care ProcessDocument1 pageDocumentation Pharmaceutical Care ProcessPurpleeyoreNo ratings yet
- BAMU B.pharmacy First Year SyllabusDocument31 pagesBAMU B.pharmacy First Year SyllabusGajanan Vaishnav0% (1)
- Immunization Policy Guidline - Kenya 2013Document72 pagesImmunization Policy Guidline - Kenya 2013okwadha simionNo ratings yet
- (Dispensing 1 Laboratory) Review NotesDocument12 pages(Dispensing 1 Laboratory) Review NotesZen HeartNo ratings yet
- Session 1 Introduction To PICS GMP 009-14Document12 pagesSession 1 Introduction To PICS GMP 009-14Elton SubijanoNo ratings yet
- Ward Round Participation Benefits for PharmacistsDocument2 pagesWard Round Participation Benefits for PharmacistsAnonymous whcvnPBeQNo ratings yet
- MSPH 600 Ao 64 S. 1989 ReportDocument6 pagesMSPH 600 Ao 64 S. 1989 ReportShynne RPhNo ratings yet
- PharmacovigilanceDocument43 pagesPharmacovigilanceTanoy SahaNo ratings yet
- (PHA6129 LAB) PrescriptionDocument5 pages(PHA6129 LAB) PrescriptionNotfor TaoNo ratings yet
- Controls: I. Material ControlDocument11 pagesControls: I. Material ControlDaena TimtimanNo ratings yet
- Pharmacy Orientation PPP211: Introduction To The Pharmacy Profession and The Future of The PharmacistDocument27 pagesPharmacy Orientation PPP211: Introduction To The Pharmacy Profession and The Future of The PharmacistJape GarridoNo ratings yet
- Drug Categorizatio RULEDocument27 pagesDrug Categorizatio RULEDIPENDRA CHAUDHARYNo ratings yet
- Social and Administrative PharmacyDocument18 pagesSocial and Administrative PharmacyMarianne Cruz100% (1)
- Practical-Physical Pharmacy-Covering Page & InstructionsDocument4 pagesPractical-Physical Pharmacy-Covering Page & Instructionsmamk77No ratings yet
- New Drug Development and Approval ProcessDocument19 pagesNew Drug Development and Approval ProcessKristine Aubrey AlvarezNo ratings yet
- Pharmaceutical Jurisprudence ManualDocument12 pagesPharmaceutical Jurisprudence ManualSlark SlarkNo ratings yet
- APPLICATION PROJECT 3: Drug Procurement & Inventory Control Kaye Erin B. Nadonga PH 4-ADocument5 pagesAPPLICATION PROJECT 3: Drug Procurement & Inventory Control Kaye Erin B. Nadonga PH 4-APrincess TiongsonNo ratings yet
- Clinical ToxicologyDocument16 pagesClinical ToxicologyJanina Arleth RamirezNo ratings yet
- Practical Aspects of Good Pharmacy PracticeDocument26 pagesPractical Aspects of Good Pharmacy PracticeNur AjiNo ratings yet
- Statement of Principle Self-Care Including Self-Medication - The Professional Role of The PharmacistDocument5 pagesStatement of Principle Self-Care Including Self-Medication - The Professional Role of The PharmacistAprilia R. Permatasari0% (1)
- Guidelines On Dispensing Dangerous DrugDocument4 pagesGuidelines On Dispensing Dangerous DrugColeen TecsonNo ratings yet
- Medical colleges quality control drug testingDocument4 pagesMedical colleges quality control drug testingpearlyn grace bangaanNo ratings yet
- Physicochemical IncompatibilitiesDocument20 pagesPhysicochemical Incompatibilitiesvicbart11No ratings yet
- Pharm Ad 1 PDFDocument7 pagesPharm Ad 1 PDFMaria Cristina QuiamjotNo ratings yet
- Stroke and HypertensionDocument4 pagesStroke and HypertensionKhessie Laye Garcia JacintoNo ratings yet
- Pharmaceutical Analysis - IiDocument12 pagesPharmaceutical Analysis - IiMae Quenie Abadingo TiroNo ratings yet
- Buccal Drug Delivery SystemDocument7 pagesBuccal Drug Delivery SystemJaikapil KachhawaNo ratings yet
- JURIS Laws PDFDocument3 pagesJURIS Laws PDFuypaul97No ratings yet
- BiopharmaceuticsDocument52 pagesBiopharmaceuticsDharma ShantiniNo ratings yet
- Worker's Care Monitored Receives Instructions.: PH-PHR 212 Dispensing 1 - LECDocument7 pagesWorker's Care Monitored Receives Instructions.: PH-PHR 212 Dispensing 1 - LECSeania BuenaventuraNo ratings yet
- Procurement and WarehouseDocument28 pagesProcurement and WarehouseVarshith Gandla100% (1)
- BiotransformationDocument27 pagesBiotransformationDemy ClementeNo ratings yet
- UST Junior Pharmacist's Association Oath and HymnDocument1 pageUST Junior Pharmacist's Association Oath and HymnJane100% (1)
- Balochistan Drugs RulesDocument5 pagesBalochistan Drugs RulesWàrìs Ràfìqùé ßàlòçhNo ratings yet
- Internship at Asia's Leading Beauty Retailer WatsonsDocument2 pagesInternship at Asia's Leading Beauty Retailer WatsonsSebastian MoronNo ratings yet
- Abnormal Uterine Bleeding in A 39 Year OldDocument16 pagesAbnormal Uterine Bleeding in A 39 Year OldEliana GerzonNo ratings yet
- Trading 101 BasicsDocument3 pagesTrading 101 BasicsNaveen KumarNo ratings yet
- Interpretation of Data FormulasDocument5 pagesInterpretation of Data FormulasEliana GerzonNo ratings yet
- 4b Case Analysis Group 3Document3 pages4b Case Analysis Group 3Eliana GerzonNo ratings yet
- Interpretation of Data FormulasDocument5 pagesInterpretation of Data FormulasEliana GerzonNo ratings yet
- Hospital Pharmacy Survey Tool PDFDocument4 pagesHospital Pharmacy Survey Tool PDFEliana GerzonNo ratings yet
- ASHP Guidelines Minimum Standard For Pharmacies in InsitutionsDocument42 pagesASHP Guidelines Minimum Standard For Pharmacies in InsitutionsEliana GerzonNo ratings yet
- Creative ParkDocument14 pagesCreative ParkAli SimsekNo ratings yet
- Fables Grade 2Document4 pagesFables Grade 2angeliNo ratings yet
- 2023 Pink Schedule FinalDocument20 pages2023 Pink Schedule Finalapi-84174556No ratings yet
- A2.student. Parts of The BodyDocument4 pagesA2.student. Parts of The BodyLaia MartíNo ratings yet
- Forensic Odontology PDFDocument6 pagesForensic Odontology PDFmoreiraingrid100% (1)
- LearnEnglish ProfessionalsPodcasts Biotechnology 0Document3 pagesLearnEnglish ProfessionalsPodcasts Biotechnology 0dinaria_ruNo ratings yet
- Stretching and FlexibilityDocument47 pagesStretching and Flexibilitymartin.wilfred7257No ratings yet
- Grammar Exercises - Simple Past TenseDocument6 pagesGrammar Exercises - Simple Past TensePatty JonasNo ratings yet
- Action Potential of NeuronsDocument3 pagesAction Potential of NeuronscheaterxorcistNo ratings yet
- The LoversDocument4 pagesThe LoversabnerdormiendoNo ratings yet
- List of Collective Nouns For Birds - Animal Group NamesDocument2 pagesList of Collective Nouns For Birds - Animal Group NamesHailee Koh Shi QiNo ratings yet
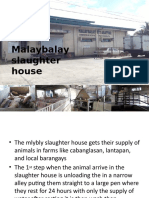
- Ansci 30 Slaughter HouseDocument34 pagesAnsci 30 Slaughter HouseDieanne MaeNo ratings yet
- Indian import duty rates for live animals, meat, fish and aquatic productsDocument98 pagesIndian import duty rates for live animals, meat, fish and aquatic productsGopal UNo ratings yet
- Animal RestraintDocument72 pagesAnimal RestraintNicka VILLANUEVANo ratings yet
- Zoo Animal Flash Cards1 PDFDocument2 pagesZoo Animal Flash Cards1 PDFsaraNo ratings yet
- Bai Darfo Registered Pet Shops As of June 30 2023Document6 pagesBai Darfo Registered Pet Shops As of June 30 2023itshardtogetauserNo ratings yet
- 114 Dog Breeds Ranked by Temperament PDFDocument1 page114 Dog Breeds Ranked by Temperament PDFRamona DonisaNo ratings yet
- Ben Ming Nian (Chinese Zodiac Animal Year of Birth)Document2 pagesBen Ming Nian (Chinese Zodiac Animal Year of Birth)SALIMNo ratings yet
- TigersDocument15 pagesTigersChinna MuthuNo ratings yet
- Ujian Masuk Program Pascasarjana: Jangan Dibuka Dulu. Tunggu PetunjukDocument21 pagesUjian Masuk Program Pascasarjana: Jangan Dibuka Dulu. Tunggu PetunjukLalu SuhaimiNo ratings yet
- Philippine Literature - Ilocos RegionDocument6 pagesPhilippine Literature - Ilocos RegionRj Bengil0% (1)
- Script Jungle CruiseDocument24 pagesScript Jungle CruiseronnyNo ratings yet
- Art336 Pre Lab 9Document4 pagesArt336 Pre Lab 9rian afriansyahNo ratings yet
- Shadowdark RPG - Welcome Pack - BWDocument17 pagesShadowdark RPG - Welcome Pack - BWVal89% (9)
- Animal Farm / Chapter 8 Reading Organizer Sample AnswersDocument7 pagesAnimal Farm / Chapter 8 Reading Organizer Sample AnswersJacques SnicketNo ratings yet
- Mage The Awakening - Intruders - Encounters With The Abyss PDFDocument228 pagesMage The Awakening - Intruders - Encounters With The Abyss PDFJohnRichardWuethrich100% (2)
- Solved CAT 2000 Paper With Solutions PDFDocument80 pagesSolved CAT 2000 Paper With Solutions PDFAravind ShekharNo ratings yet
- Mga Uri NG ManokDocument31 pagesMga Uri NG ManokMa LeslynneNo ratings yet
- Balinese Cat Breed Profile: Characteristics, Care, Health and MoreDocument23 pagesBalinese Cat Breed Profile: Characteristics, Care, Health and MoreprosvetiteljNo ratings yet
- Office Head Titles MunicipalityDocument2 pagesOffice Head Titles MunicipalityGeo AngeloNo ratings yet