You might also like
- MagSulfate InfoSheetDocument2 pagesMagSulfate InfoSheetRatning TitissariNo ratings yet
- Journal Reading MgSO4Document12 pagesJournal Reading MgSO4Jejem Marandra EmkamasNo ratings yet
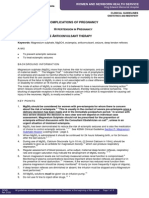
- Complications of Pregnancy H P: Agnesium Ulphate Nticonvulsant TherapyDocument8 pagesComplications of Pregnancy H P: Agnesium Ulphate Nticonvulsant TherapysucyasyifaNo ratings yet
- Magnesium Sulfate in Water For Injection: Flexible Plastic Container For Intravenous Use OnlyDocument5 pagesMagnesium Sulfate in Water For Injection: Flexible Plastic Container For Intravenous Use OnlyKN BaijuNo ratings yet
- WNHS - og.HypertensionPregnancy MagnesiumAnticonvulsantDocument13 pagesWNHS - og.HypertensionPregnancy MagnesiumAnticonvulsantNisa UlfaturrosyidaNo ratings yet
- Mgso4 Mekanisme in KehamilanDocument10 pagesMgso4 Mekanisme in KehamilanIqra AnugerahNo ratings yet
- P2010/0509-001 Management of EclampsiaDocument7 pagesP2010/0509-001 Management of EclampsiaYwagar YwagarNo ratings yet
- 4784 17639 1 PB PDFDocument6 pages4784 17639 1 PB PDFbaidyanath kumarNo ratings yet
- MG Sulfate Pada Pencegahan EklamsiaDocument16 pagesMG Sulfate Pada Pencegahan Eklamsiaasti dNo ratings yet
- Rovamycin 3868 DR 1256036243912Document6 pagesRovamycin 3868 DR 1256036243912Ahmed El AlfyNo ratings yet
- Magnesium SulfateDocument2 pagesMagnesium SulfateKarla Karina Dela CruzNo ratings yet
- Magnesium Sulfate - Management of Hypertensive Disorders of PregnancyDocument7 pagesMagnesium Sulfate - Management of Hypertensive Disorders of PregnancySylvester J DakaNo ratings yet
- Summary of Product Characteristics: PosologyDocument9 pagesSummary of Product Characteristics: Posologyddandan_2No ratings yet
- Comparison of Safety and Efficacy of Intramuscular and Intravenous Regime of Magnesium Sulfate in Eclampsia and Severe PreeclampsiaDocument5 pagesComparison of Safety and Efficacy of Intramuscular and Intravenous Regime of Magnesium Sulfate in Eclampsia and Severe PreeclampsiaEdo eaNo ratings yet
- Alkeran®: (Melphalan) TabletsDocument8 pagesAlkeran®: (Melphalan) Tabletskaren rodriguezNo ratings yet
- Epilepsy Update SeshadriDocument10 pagesEpilepsy Update SeshadriSeshadri Sekhar ChatterjeeNo ratings yet
- Primaquine: Phosphate Tablets, UspDocument6 pagesPrimaquine: Phosphate Tablets, UspEphenk PunkNo ratings yet
- Is Zuspan Regimen Adequate For Preventing EclampsiDocument3 pagesIs Zuspan Regimen Adequate For Preventing EclampsiTimpswalo EmatsuloNo ratings yet
- Epilepsia IIIDocument13 pagesEpilepsia IIILeslie TelssieNo ratings yet
- Analgesic: Mefenamic AcidDocument5 pagesAnalgesic: Mefenamic Acidmegazhang94No ratings yet
- Magnesium Sulphate (Mgso4) For Fetal Neuroprotection: DR Rajiv KumarDocument16 pagesMagnesium Sulphate (Mgso4) For Fetal Neuroprotection: DR Rajiv KumarManju KumariNo ratings yet
- Purixan (Mercaptopurine) - Drug: Nova Laboratories, LTDDocument7 pagesPurixan (Mercaptopurine) - Drug: Nova Laboratories, LTDsupandiNo ratings yet
- Purixan (Mercaptopurine) - Drug: Nova Laboratories, LTDDocument7 pagesPurixan (Mercaptopurine) - Drug: Nova Laboratories, LTDsupandiNo ratings yet
- Anticonvulsant Therapy For EclampsiaDocument7 pagesAnticonvulsant Therapy For Eclampsiarafifah_nadiaNo ratings yet
- Resurrection University Medication CardDocument2 pagesResurrection University Medication CardBohung ConNo ratings yet
- Magnesium Sulfate: Injection, UspDocument13 pagesMagnesium Sulfate: Injection, Uspnur-aisyahkNo ratings yet
- MolnupiravirDocument7 pagesMolnupiravirConcepStore PyNo ratings yet
- Steroid Resistant Nephrotic SyndromeDocument72 pagesSteroid Resistant Nephrotic SyndromeMonika Angra100% (1)
- ZometaDocument6 pagesZometaMisgi Candra DasaNo ratings yet
- MEFENAMIC-ACID-mefenamic Acid Caps Ule Sciele Pharma IncDocument14 pagesMEFENAMIC-ACID-mefenamic Acid Caps Ule Sciele Pharma IncIrma DamayantiNo ratings yet
- Management of Eclampsia and Magnesium ToxicityDocument34 pagesManagement of Eclampsia and Magnesium ToxicityRezki IsharNo ratings yet
- Lamivudine: in Vitro Studies Indicate That Zidovudine-Resistant Virus Isolates Can Become ZidovudineDocument7 pagesLamivudine: in Vitro Studies Indicate That Zidovudine-Resistant Virus Isolates Can Become ZidovudineKirtikrushna Suresh Prasad OjhaNo ratings yet
- Omalizumab - Drug Information - UpToDate-4Document5 pagesOmalizumab - Drug Information - UpToDate-4Vh TRNo ratings yet
- البراسيتول في استرالياDocument11 pagesالبراسيتول في استراليازيد محمدNo ratings yet
- BGGTN - 1311-Spc-Revu enDocument6 pagesBGGTN - 1311-Spc-Revu enGenesisNo ratings yet
- Pediatric Malaria Treatment & Management: Approach Considerations, Intensive Care, Deterrence and PreventionDocument4 pagesPediatric Malaria Treatment & Management: Approach Considerations, Intensive Care, Deterrence and PreventionVivi DeviyanaNo ratings yet
- Regulatory Document2 EngDocument201 pagesRegulatory Document2 EngDomenico LombardiniNo ratings yet
- Immunosuppressive Regimens For Renal Transplantation: J. D. BriggsDocument3 pagesImmunosuppressive Regimens For Renal Transplantation: J. D. BriggshassanNo ratings yet
- Mgso 4Document3 pagesMgso 4dr_dhiyaNo ratings yet
- Levetiracetam in Refractory Pediatric EpilepsyDocument11 pagesLevetiracetam in Refractory Pediatric EpilepsyAdlinaNo ratings yet
- Preeclampsia Prep Questions-HaleyVestDocument5 pagesPreeclampsia Prep Questions-HaleyVestHaley Vest MustaficNo ratings yet
- CiclosporinDocument7 pagesCiclosporinLunatic DreamerNo ratings yet
- MOXIFLOXACIN MonographDocument3 pagesMOXIFLOXACIN Monographfayrouz fathiNo ratings yet
- LINEZOLID MonographDocument3 pagesLINEZOLID Monographfayrouz fathiNo ratings yet
- Magnesium Sulfa-WPS OfficeDocument21 pagesMagnesium Sulfa-WPS OfficeNeha SinghNo ratings yet
- Low Dose Magnesium Sulphate Regime For Eclampsia: Bangal V., Kwatra A., Raghav S., Jadhav SDocument3 pagesLow Dose Magnesium Sulphate Regime For Eclampsia: Bangal V., Kwatra A., Raghav S., Jadhav STika RiantyNo ratings yet
- AnesthEssaysRes73307-3408652 092806Document6 pagesAnesthEssaysRes73307-3408652 092806Nadya LiemNo ratings yet
- Omeprazole: Losec 40 MG Powder and Solvent For Solution For Injection CompositionDocument11 pagesOmeprazole: Losec 40 MG Powder and Solvent For Solution For Injection CompositionNadia AfifahNo ratings yet
- Piroxicam Pharmacology 1Document16 pagesPiroxicam Pharmacology 1Shafira TamaraNo ratings yet
- NIVOLUMAB - Caracteristicile Produsului Document EMADocument58 pagesNIVOLUMAB - Caracteristicile Produsului Document EMALaurentiu DecuNo ratings yet
- 14 Aher EtalDocument4 pages14 Aher EtaleditorijmrhsNo ratings yet
- AzathioprineDocument14 pagesAzathioprineNur Wakhid HidayatNo ratings yet
- WWW - Fda.gov/medwatch: Reference ID: 4335341Document17 pagesWWW - Fda.gov/medwatch: Reference ID: 4335341Daniel Del Rio RamirezNo ratings yet
- Magnesium Sulfate: Injection, USPDocument13 pagesMagnesium Sulfate: Injection, USPRagesh .MNo ratings yet
- Australian Product Information - Maxolon (Metoclopramide Hydrochloride) Tablets and Injection 1 Name of The MedicineDocument10 pagesAustralian Product Information - Maxolon (Metoclopramide Hydrochloride) Tablets and Injection 1 Name of The Medicinefoaad foaadNo ratings yet
- 10 Gram Loading Dose of MgSo4 Okusanya BO Et AlDocument6 pages10 Gram Loading Dose of MgSo4 Okusanya BO Et AlTRI HARYANINo ratings yet
- PRIMAQUINE PHOSPHATE-primaquine Phos Phate Tablet Bays Hore Pharmaceuticals, LLCDocument8 pagesPRIMAQUINE PHOSPHATE-primaquine Phos Phate Tablet Bays Hore Pharmaceuticals, LLCKulfi BarfiNo ratings yet
- LEVOFLOXACIN MonographDocument3 pagesLEVOFLOXACIN Monographfayrouz fathiNo ratings yet
- Fast Facts: Ottimizzazione del trattamento delle fluttuazioni motorie nella malattia di ParkinsonFrom EverandFast Facts: Ottimizzazione del trattamento delle fluttuazioni motorie nella malattia di ParkinsonNo ratings yet
- Clinical Chemistry, Immunology and Laboratory Quality Control: A Comprehensive Review for Board Preparation, Certification and Clinical PracticeFrom EverandClinical Chemistry, Immunology and Laboratory Quality Control: A Comprehensive Review for Board Preparation, Certification and Clinical PracticeRating: 5 out of 5 stars5/5 (1)
- Luncheon Keynote Address: Global Nurse Leadership at Work - Mozambque - DBossemeyerDocument22 pagesLuncheon Keynote Address: Global Nurse Leadership at Work - Mozambque - DBossemeyerJhpiegoNo ratings yet
- Burkina Faso and Jhpiego Kick Off $15 Million Effort To Reduce Malaria Deaths by 50% CountrywideDocument1 pageBurkina Faso and Jhpiego Kick Off $15 Million Effort To Reduce Malaria Deaths by 50% CountrywideJhpiegoNo ratings yet
- Ronald McDonald House Charities Awards Jhpiego Grant To Reach Thousands of Children With Lifesaving Malaria ServicesDocument2 pagesRonald McDonald House Charities Awards Jhpiego Grant To Reach Thousands of Children With Lifesaving Malaria ServicesJhpiegoNo ratings yet
- Helping Mothers Survive: Bleeding After BirthDocument36 pagesHelping Mothers Survive: Bleeding After BirthJhpiegoNo ratings yet
- GE Foundation Awards Jhpiego $2.3 Million To Accelerate Global Health InnovationsDocument2 pagesGE Foundation Awards Jhpiego $2.3 Million To Accelerate Global Health InnovationsJhpiegoNo ratings yet
- Closing Remarks - Nursing Midwifery LeadershipDocument19 pagesClosing Remarks - Nursing Midwifery LeadershipJhpiegoNo ratings yet
- Jhpiego Wins UN Population AwardDocument1 pageJhpiego Wins UN Population AwardJhpiegoNo ratings yet
- Use of Google Group Applications Technology To Enhance Commodity Security in Health Facilities: Experiences From Eastern and Central KenyaDocument1 pageUse of Google Group Applications Technology To Enhance Commodity Security in Health Facilities: Experiences From Eastern and Central KenyaJhpiegoNo ratings yet
- Caution in Interpreting Demographic and Health Survey Male Circumcision ResultsDocument1 pageCaution in Interpreting Demographic and Health Survey Male Circumcision ResultsJhpiegoNo ratings yet
- Strengthening TB/HIV Services in Zambia Defence Force Contributes To High Numbers of TB Cases Diagnosed and Tested For HIVDocument1 pageStrengthening TB/HIV Services in Zambia Defence Force Contributes To High Numbers of TB Cases Diagnosed and Tested For HIVJhpiegoNo ratings yet
- Use of Google Group Applications Technology To Enhance Commodity Security in Health Facilities: Experiences From Eastern and Central KenyaDocument1 pageUse of Google Group Applications Technology To Enhance Commodity Security in Health Facilities: Experiences From Eastern and Central KenyaJhpiegoNo ratings yet
- Patient Escorts - An Essential Element of An HIV Program in NigeriaDocument14 pagesPatient Escorts - An Essential Element of An HIV Program in NigeriaJhpiegoNo ratings yet
- Reaching Adolescents With Safe Male Circumcision Services: School Campaigns in BotswanaDocument1 pageReaching Adolescents With Safe Male Circumcision Services: School Campaigns in BotswanaJhpiegoNo ratings yet
- "Catching Up" Through Improved Voluntary Medical Male Circumcision (VMMC) Campaigns: Lessons From ZambiaDocument1 page"Catching Up" Through Improved Voluntary Medical Male Circumcision (VMMC) Campaigns: Lessons From ZambiaJhpiegoNo ratings yet
- Integrated PMTCT and Maternal Health Services Improve Both HIV and Maternal Health Indicators in Rural EthiopiaDocument1 pageIntegrated PMTCT and Maternal Health Services Improve Both HIV and Maternal Health Indicators in Rural EthiopiaJhpiegoNo ratings yet
- The Sustainability Plan: Early Lessons From The Integration of Early Infant Male Circumcision Services Into Reproductive and Child Health Services in Iringa Region, TanzaniaDocument1 pageThe Sustainability Plan: Early Lessons From The Integration of Early Infant Male Circumcision Services Into Reproductive and Child Health Services in Iringa Region, TanzaniaJhpiegoNo ratings yet
- Sexual Prevention and Adolescents Attending Voluntary Medical Male Circumcision (VMMC) Services in Tanzania: A Golden Opportunity To Offer Adolescent-Targeted ServicesDocument1 pageSexual Prevention and Adolescents Attending Voluntary Medical Male Circumcision (VMMC) Services in Tanzania: A Golden Opportunity To Offer Adolescent-Targeted ServicesJhpiegoNo ratings yet
- Spatial Mapping Results in a Successful Large-Scale Voluntary Medical Male Circumcision (VMMC) Campaign: Using GIS Data for Decision-Making Positively Impacts the VMMC Scale-Up in Iringa and Njombe Regions of TanzaniaDocument1 pageSpatial Mapping Results in a Successful Large-Scale Voluntary Medical Male Circumcision (VMMC) Campaign: Using GIS Data for Decision-Making Positively Impacts the VMMC Scale-Up in Iringa and Njombe Regions of TanzaniaJhpiegoNo ratings yet
- Capturing A Missed Opportunity Through Postpartum Intrauterine Contraceptive Device (PPIUCD) in Ethiopia: Experience of The Maternal and Child Health Integrated Program (MCHIP)Document13 pagesCapturing A Missed Opportunity Through Postpartum Intrauterine Contraceptive Device (PPIUCD) in Ethiopia: Experience of The Maternal and Child Health Integrated Program (MCHIP)JhpiegoNo ratings yet
- Seizing The Opportunity - Working With Adolescent Boys For An HIV-free Generation"Document14 pagesSeizing The Opportunity - Working With Adolescent Boys For An HIV-free Generation"JhpiegoNo ratings yet
- Cervical Cancer Screening - JhpiegoDocument15 pagesCervical Cancer Screening - JhpiegoJhpiego100% (1)
- Community Health Workers Creating Family Planning Social Networks Through Satisified ClientsDocument15 pagesCommunity Health Workers Creating Family Planning Social Networks Through Satisified ClientsJhpiegoNo ratings yet
- BeAccess To Loop Electrosurgical Excision Procedure (LEEP) in Cervical Cancer Prevention Is Critical For HIV-Endemic Settings: Experiences From Tanzaniasana - CECAPDocument1 pageBeAccess To Loop Electrosurgical Excision Procedure (LEEP) in Cervical Cancer Prevention Is Critical For HIV-Endemic Settings: Experiences From Tanzaniasana - CECAPJhpiegoNo ratings yet
- Improving Family Planning Services Through Training and Capacity Building of Frontline Workers of Maternal and Newborn Health Care Program in A Low-Resource Area of Rural BangladeshDocument20 pagesImproving Family Planning Services Through Training and Capacity Building of Frontline Workers of Maternal and Newborn Health Care Program in A Low-Resource Area of Rural BangladeshJhpiegoNo ratings yet
- The Missing Indicator: The Use of A Strategic Advocacy Approach To Promote Data-Driven Decisions On Task-Sharing in KenyaDocument9 pagesThe Missing Indicator: The Use of A Strategic Advocacy Approach To Promote Data-Driven Decisions On Task-Sharing in KenyaJhpiegoNo ratings yet
- Screening For Maternal Anemia: A Low-Cost Solution For A Persistent Global Health ChallengeDocument1 pageScreening For Maternal Anemia: A Low-Cost Solution For A Persistent Global Health ChallengeJhpiegoNo ratings yet
- Counseling and Improved Family Planning Uptake During The Extended Postpartum Period - Pakistan ExperienceDocument15 pagesCounseling and Improved Family Planning Uptake During The Extended Postpartum Period - Pakistan ExperienceJhpiegoNo ratings yet
- Use of Long-Acting Reversible Contraceptive (LARC) Methods in Postabortal PeriodDocument11 pagesUse of Long-Acting Reversible Contraceptive (LARC) Methods in Postabortal PeriodJhpiegoNo ratings yet
- Malaria-Protecting Mothers and Their FamiliesDocument4 pagesMalaria-Protecting Mothers and Their FamiliesJhpiegoNo ratings yet
- CryoPop: A Low-Cost Solution For Treating Cervical CancerDocument1 pageCryoPop: A Low-Cost Solution For Treating Cervical CancerJhpiegoNo ratings yet
- ID Pengaruh Self Selected Individual MusicDocument12 pagesID Pengaruh Self Selected Individual MusicNur AiniNo ratings yet
- Level 2 Unit 39 Assist in The Administration of MedicationDocument7 pagesLevel 2 Unit 39 Assist in The Administration of MedicationSzabolcs LehotaNo ratings yet
- Soares - Como Escolher Um Anestesico Local - 2005 PDFDocument9 pagesSoares - Como Escolher Um Anestesico Local - 2005 PDFjvb sobralNo ratings yet
- Workbook Answer KeyDocument27 pagesWorkbook Answer Keysalcedo4479% (56)
- Hypertensive Disorder in PregnancyDocument7 pagesHypertensive Disorder in PregnancyBiscuits and milkNo ratings yet
- Wiri 08 - Zambia Trip Application FormDocument11 pagesWiri 08 - Zambia Trip Application Forminfo@zcfcanada.orgNo ratings yet
- Telescopium) EXTRACTS: West Visayas State University College of MedicineDocument5 pagesTelescopium) EXTRACTS: West Visayas State University College of MedicineMark FuerteNo ratings yet
- Jocelyn JanniDocument2 pagesJocelyn Janniapi-271982945No ratings yet
- Mental HealthDocument80 pagesMental HealthSingYen QuickNo ratings yet
- Child Abuse Nursing Care PlanDocument7 pagesChild Abuse Nursing Care PlanMAHESH KOUJALAGINo ratings yet
- Worksheet 15 For Prep A: FR - ZMR.18 / R.02 / R.T: 22.09.2012 1 / 4Document4 pagesWorksheet 15 For Prep A: FR - ZMR.18 / R.02 / R.T: 22.09.2012 1 / 4elif demirelNo ratings yet
- Argument Essay ReflectionDocument5 pagesArgument Essay Reflectionapi-509671089No ratings yet
- Application Letter Nurse AideDocument2 pagesApplication Letter Nurse AideOliver Ian ReposoNo ratings yet
- To The Philosophy of The Human Person: Quarter 1 - Module 4.2: Care For The EnvironmentDocument21 pagesTo The Philosophy of The Human Person: Quarter 1 - Module 4.2: Care For The EnvironmentDustin EsguerraNo ratings yet
- Fu Zhen and TurtleDocument7 pagesFu Zhen and Turtledrakpo100% (2)
- DizzinessDocument65 pagesDizzinessעידית בנימיןNo ratings yet
- S9 Q4 M1 Transport and Excretion and Respiration and Energy Exchange QuizDocument3 pagesS9 Q4 M1 Transport and Excretion and Respiration and Energy Exchange QuizJermae DizonNo ratings yet
- List of AntibioticsDocument9 pagesList of Antibioticsdesi_mNo ratings yet
- Garrison, NancyDocument139 pagesGarrison, NancyBrunoNo ratings yet
- Jawaharlal Nehru Engineering College: Laboratory ManualDocument58 pagesJawaharlal Nehru Engineering College: Laboratory ManualKrishna Vasishta KavuturuNo ratings yet
- Mapping Bellvitge 2023Document8 pagesMapping Bellvitge 2023Lluís Cavallé MorenoNo ratings yet
- Washington D.C. Afro-American Newspaper, July 24, 2010Document20 pagesWashington D.C. Afro-American Newspaper, July 24, 2010The AFRO-American NewspapersNo ratings yet
- Adi Setya Frida Utami - FIKES PDFDocument108 pagesAdi Setya Frida Utami - FIKES PDFZyy VyeNo ratings yet
- ADHD and The Endocannabinoid SystemDocument11 pagesADHD and The Endocannabinoid Systempn100% (1)
- Jain College, Bangalore Mock Paper - 1, March - 2021 II PUC - EnglishDocument6 pagesJain College, Bangalore Mock Paper - 1, March - 2021 II PUC - EnglishSuchit KarnamNo ratings yet
- Star Health and Allied Insurance Company Limited: Customer Information Sheet - Family Health Optima Insurance PlanDocument12 pagesStar Health and Allied Insurance Company Limited: Customer Information Sheet - Family Health Optima Insurance Plananiket goyalNo ratings yet
- Mr. H, 41YO, Multiple Vulnus Apertum, Dr. Saktrio D. Subarno, SP - BP-REDocument23 pagesMr. H, 41YO, Multiple Vulnus Apertum, Dr. Saktrio D. Subarno, SP - BP-REMusayada Dawua Part IINo ratings yet
- Woman Burned by Acid in Random Subway Attack Has 16th SurgeryDocument1 pageWoman Burned by Acid in Random Subway Attack Has 16th Surgeryed2870winNo ratings yet
- Heat StrokeDocument4 pagesHeat StrokeGerald YasonNo ratings yet
- MAPEH Study NotesDocument5 pagesMAPEH Study NotesBithao DaisyNo ratings yet