You might also like
- ERS Guidelines LRTIDocument43 pagesERS Guidelines LRTIkurutalaNo ratings yet
- Cpap and CopdDocument6 pagesCpap and CopdAshish PandeyNo ratings yet
- Status Asthmaticus Prolonged Expiratory TimeDocument4 pagesStatus Asthmaticus Prolonged Expiratory TimeAshish PandeyNo ratings yet
- Head Compartment SyndromeDocument40 pagesHead Compartment SyndromeAshish PandeyNo ratings yet
- Anaesthesia and CopdDocument7 pagesAnaesthesia and CopdAshish PandeyNo ratings yet
- Early Enteral Immunonutrition vs. Parenteral Nutrition in Critically Ill Patients Without Severe SepsisDocument8 pagesEarly Enteral Immunonutrition vs. Parenteral Nutrition in Critically Ill Patients Without Severe SepsisAshish PandeyNo ratings yet
- Alveolar Arterial Gradient and EmbolismDocument4 pagesAlveolar Arterial Gradient and EmbolismAshish PandeyNo ratings yet
- Glycemic Index ListingDocument60 pagesGlycemic Index ListingAshish PandeyNo ratings yet
- Approach To ThrombocytopeniaDocument9 pagesApproach To ThrombocytopeniaAshish PandeyNo ratings yet
- Disseminated Intravascular Coagulation: Nigel S. Key, MD Professor Division of Hematology/OncologyDocument40 pagesDisseminated Intravascular Coagulation: Nigel S. Key, MD Professor Division of Hematology/Oncologyuse4meNo ratings yet
- Hepatic Encephalopathy: Prof. Huiling Yang Dept. PathophysiologyDocument46 pagesHepatic Encephalopathy: Prof. Huiling Yang Dept. PathophysiologyAshish PandeyNo ratings yet
- Hepatic Encephalopathy: Prof. Huiling Yang Dept. PathophysiologyDocument46 pagesHepatic Encephalopathy: Prof. Huiling Yang Dept. PathophysiologyAshish PandeyNo ratings yet
- Recent Advances in Sepsis Management12Document41 pagesRecent Advances in Sepsis Management12Ashish PandeyNo ratings yet
- CCRP2012 950393 PDFDocument14 pagesCCRP2012 950393 PDFrahmawatusNo ratings yet
- Traumatic Brain Injury EnglishDocument41 pagesTraumatic Brain Injury EnglishAshish PandeyNo ratings yet
- CT Imaging of Acute PancreatitisDocument51 pagesCT Imaging of Acute PancreatitisVoNda Apriliani0% (1)
- Journal EbmDocument10 pagesJournal EbmmarthinNo ratings yet
- Manage Hyperthermia with Cooling MethodsDocument62 pagesManage Hyperthermia with Cooling MethodsAshish PandeyNo ratings yet
- Cardiopulmonary Interaction in Critically Ill Patients: Major Determinants of Cardiovascular Responses to VentilationDocument48 pagesCardiopulmonary Interaction in Critically Ill Patients: Major Determinants of Cardiovascular Responses to VentilationAshish PandeyNo ratings yet
- Copd and AsthmaDocument74 pagesCopd and AsthmaAdel HamadaNo ratings yet
- Cardiopulmonary Interaction in Critically Ill Patients: Major Determinants of Cardiovascular Responses to VentilationDocument48 pagesCardiopulmonary Interaction in Critically Ill Patients: Major Determinants of Cardiovascular Responses to VentilationAshish PandeyNo ratings yet
- Endemic Fungal DsDocument5 pagesEndemic Fungal DsdrsomanjanaNo ratings yet
- Cin Cim ClassDocument29 pagesCin Cim ClassAshish PandeyNo ratings yet
- Principles of Clinical Pharmacology: Steven P. Stratton, PH.DDocument53 pagesPrinciples of Clinical Pharmacology: Steven P. Stratton, PH.DAshish PandeyNo ratings yet
- XXXX Antibiotic Stewardship MDRO Chapter 5 Module Joint CommissionDocument28 pagesXXXX Antibiotic Stewardship MDRO Chapter 5 Module Joint CommissionAshish Pandey100% (2)
- When The Ventilator Alarm Sounds SANTANILLADocument58 pagesWhen The Ventilator Alarm Sounds SANTANILLAAshish PandeyNo ratings yet
- PV Loop PresentationDocument25 pagesPV Loop PresentationAshish PandeyNo ratings yet
- Amphotercin BDocument5 pagesAmphotercin BAshish PandeyNo ratings yet
- Myasthenia GravisDocument6 pagesMyasthenia GravisAshish PandeyNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5784)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hypersensitivity Type III - Tissue Damage by Immune Complex DepositionDocument16 pagesHypersensitivity Type III - Tissue Damage by Immune Complex DepositionRenz CofrerosNo ratings yet
- Sars-Cov-2 GM Rapid Test-HightopDocument18 pagesSars-Cov-2 GM Rapid Test-HightopKarina Zafra LaviNo ratings yet
- Immunization Titer FormsDocument19 pagesImmunization Titer FormsCole GarrettNo ratings yet
- Basic ImmunologyDocument57 pagesBasic ImmunologyRonalyn UgatNo ratings yet
- Questionnaire (ISBB)Document14 pagesQuestionnaire (ISBB)Angelo Mercede100% (1)
- Immunology - 1200Document2,640 pagesImmunology - 1200tcabanilNo ratings yet
- King Saud University Immunology Course OverviewDocument86 pagesKing Saud University Immunology Course OverviewAbbass El-Outa100% (1)
- E3042 16Document4 pagesE3042 164romi89No ratings yet
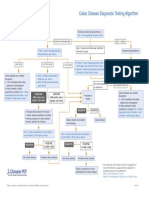
- Celiac Disease Diagnostic Testing AlgorithmDocument1 pageCeliac Disease Diagnostic Testing AlgorithmtarogiosdrakNo ratings yet
- CALIBRATE IMSE Answer Key by Sir CarlDocument5 pagesCALIBRATE IMSE Answer Key by Sir CarlMark Justin OcampoNo ratings yet
- Important Drug Summaries and Embryology ConceptsDocument175 pagesImportant Drug Summaries and Embryology Conceptsvk100% (1)
- Immunology Lecture 03 - Antibodies Part 1 - 2018Document36 pagesImmunology Lecture 03 - Antibodies Part 1 - 2018api-273068056No ratings yet
- TORCH in PregnancyDocument122 pagesTORCH in PregnancyroserosannaNo ratings yet
- Immune System Organs, Cells and MoleculesDocument39 pagesImmune System Organs, Cells and MoleculesFaith MbasaniNo ratings yet
- NRL Price List 2018Document17 pagesNRL Price List 2018Anonymous YS9NbuNo ratings yet
- Classification Criteria For SLEDocument4 pagesClassification Criteria For SLEofva26No ratings yet
- Hypersensitivity: M.G.Rajanandh, Dept. of Pharmacy Practice, SRM College of Pharmacy, SRM UniversityDocument87 pagesHypersensitivity: M.G.Rajanandh, Dept. of Pharmacy Practice, SRM College of Pharmacy, SRM UniversityJulienne Sanchez-SalazarNo ratings yet
- B. PhemfigoidDocument11 pagesB. PhemfigoidAdrin Ma'rufNo ratings yet
- Drug AllergyDocument28 pagesDrug AllergyVicky Sandhu100% (1)
- Intratect 50 G L SPC 05 02 2016 - UkDocument12 pagesIntratect 50 G L SPC 05 02 2016 - UkCarla CaldararuNo ratings yet
- Chapter 43: Nursing Care of A Family When A Child Has An Infectious Disorder The Infectious Process #1 Infectious Disease in ChildrenDocument20 pagesChapter 43: Nursing Care of A Family When A Child Has An Infectious Disorder The Infectious Process #1 Infectious Disease in ChildrenMark oliver Gonzales100% (1)
- A. Natural Passive Immunity: Igg & Iga Are ConsideredDocument9 pagesA. Natural Passive Immunity: Igg & Iga Are ConsideredIme.No ratings yet
- Anti-Glomerular Basement Membrane Disease An Update On Subgroups, Pathogenesis and TherapiesDocument7 pagesAnti-Glomerular Basement Membrane Disease An Update On Subgroups, Pathogenesis and TherapiesLucas SilveiraNo ratings yet
- PharmacologyTestsDocument37 pagesPharmacologyTestsmendozajanice0601No ratings yet
- A 0162 DatDocument1 pageA 0162 Dathonest_loezNo ratings yet
- MA Micro Carricullm Latest by TZT (Create)Document63 pagesMA Micro Carricullm Latest by TZT (Create)HlaSoe WinNo ratings yet
- Sars-Cov-2 RBD Neutralizing Antibody Induction Is Enhanced by Particulate VaccinationDocument11 pagesSars-Cov-2 RBD Neutralizing Antibody Induction Is Enhanced by Particulate VaccinationmwdhtirahNo ratings yet
- Lady Mary Wortley Montagu pioneers smallpox variolationDocument8 pagesLady Mary Wortley Montagu pioneers smallpox variolationCSEKhateeb Ahmed RoomiNo ratings yet
- Nutritional Interventions PDFDocument17 pagesNutritional Interventions PDFLalit MittalNo ratings yet
- Early Regular Egg Exposure in Infants With Eczema: A Randomized Controlled TrialDocument7 pagesEarly Regular Egg Exposure in Infants With Eczema: A Randomized Controlled TrialnicloverNo ratings yet