You might also like
- A System of Operative Surgery, Volume IV (of 4)From EverandA System of Operative Surgery, Volume IV (of 4)Rating: 4 out of 5 stars4/5 (1)
- CorrectsDocument46 pagesCorrectsnursing_hallNo ratings yet
- Chapter 1 - Central Venous CathetersDocument6 pagesChapter 1 - Central Venous CathetersParth PatelNo ratings yet
- Final General Surgery (1) - 230122 - 192353Document49 pagesFinal General Surgery (1) - 230122 - 192353Lika BukhaidzeNo ratings yet
- Clinical Examination of The AbdomenDocument13 pagesClinical Examination of The AbdomenNur Miladiyah100% (1)
- Medical History Questions ExplainedDocument10 pagesMedical History Questions ExplainedAlex LxNo ratings yet
- Pediatricok Board Exam QuestionsDocument11 pagesPediatricok Board Exam QuestionsjkmirandasbcNo ratings yet
- 1st Trimester BleedingDocument67 pages1st Trimester BleedingRaiden VizcondeNo ratings yet
- The Respiratory SystemDocument28 pagesThe Respiratory SystemJuma SammyNo ratings yet
- How Long Do Partial Thickness Burns Typically Take To Heal?Document49 pagesHow Long Do Partial Thickness Burns Typically Take To Heal?Farah FarahNo ratings yet
- Exam Name Exam ID: 56 - Pass Mark: 59: يـــنادوـسلا يـــبـطلا ســلجـملا Sudan Medical CouncilDocument91 pagesExam Name Exam ID: 56 - Pass Mark: 59: يـــنادوـسلا يـــبـطلا ســلجـملا Sudan Medical CouncilMoamen HellisNo ratings yet
- Medical Terminology Guide for Nursing StudentsDocument4 pagesMedical Terminology Guide for Nursing StudentsCzarina Mae Quinones TadeoNo ratings yet
- Internal Medicine 5th MidtermDocument13 pagesInternal Medicine 5th MidtermIashdip iashdipNo ratings yet
- ANDI Classification System Explains Benign Breast DisordersDocument9 pagesANDI Classification System Explains Benign Breast DisordersaprooolNo ratings yet
- ASD Atrial Septal Defect PDFDocument9 pagesASD Atrial Septal Defect PDFAco AjjahNo ratings yet
- Neuro StudyguideDocument28 pagesNeuro StudyguidePrince K. TaileyNo ratings yet
- Patient Education for Ileal Conduit CareDocument11 pagesPatient Education for Ileal Conduit CareICa MarlinaNo ratings yet
- BreastDocument14 pagesBreastapi-3840195No ratings yet
- Gastroentrology LastDocument48 pagesGastroentrology LastAbdallah K. RamadanNo ratings yet
- Gynecology and ObstetricsDocument125 pagesGynecology and Obstetricsapi-3712326100% (4)
- Hepatobiliary System: BY Pranjal Kulkarni Neha ManeDocument85 pagesHepatobiliary System: BY Pranjal Kulkarni Neha ManeGurneetNo ratings yet
- CLM PresentationDocument13 pagesCLM PresentationHSC UNITEDNo ratings yet
- Abdominal Aortic Aneurysm Case Study: by Lisa ErwertDocument21 pagesAbdominal Aortic Aneurysm Case Study: by Lisa ErwertShashidhar Venkatesh MurthyNo ratings yet
- A. Cardio: Anatomy & Physiology - A. AnatomyDocument43 pagesA. Cardio: Anatomy & Physiology - A. AnatomyGloryJaneNo ratings yet
- Pathophysiology of Body Fluids and Fluid TherapyDocument3 pagesPathophysiology of Body Fluids and Fluid TherapybookwormMDNo ratings yet
- Approach To The Surgical PatientDocument51 pagesApproach To The Surgical Patientsanjivdas100% (1)
- Urinary Tract Infections PowerpointDocument22 pagesUrinary Tract Infections Powerpointsamdhathri100% (1)
- D. NegligenceDocument11 pagesD. NegligenceKing GeorgeNo ratings yet
- Hemophilia ADocument8 pagesHemophilia AroxhencaNo ratings yet
- CVS Pathophysiology of ShockDocument11 pagesCVS Pathophysiology of ShockSherwan R Shal100% (4)
- Fluids and Electrolytes2Document8 pagesFluids and Electrolytes2Potchiee PfizerNo ratings yet
- Joint Pain - ApproachDocument32 pagesJoint Pain - ApproachHassan Bin AjmalNo ratings yet
- Basic Life Support in Infants and ChildrenDocument9 pagesBasic Life Support in Infants and ChildrenMelissa Espinoza PeñaNo ratings yet
- Hepatobiliary DiseaseDocument60 pagesHepatobiliary DiseaseFirdaus AslamNo ratings yet
- Managing Angina: AHA Guidelines on Diagnosis and TreatmentDocument96 pagesManaging Angina: AHA Guidelines on Diagnosis and TreatmentJaymica Laggui DacquilNo ratings yet
- Signs of Respiratory Distress in Your Child: Signs To Look ForDocument2 pagesSigns of Respiratory Distress in Your Child: Signs To Look ForMa GynNo ratings yet
- Fetal Heart Circulation Diagram and Key StructuresDocument2 pagesFetal Heart Circulation Diagram and Key StructuresJubaida JemiNo ratings yet
- Blood Transfusion PDFDocument20 pagesBlood Transfusion PDFalaamorsyNo ratings yet
- Urinary EliminationDocument50 pagesUrinary EliminationAime MvuyekureNo ratings yet
- Oncology NursingDocument15 pagesOncology NursingArdrina Sappari100% (1)
- Pediatric Shock: A Guide to Identification, Classification and Initial ManagementDocument20 pagesPediatric Shock: A Guide to Identification, Classification and Initial ManagementvgmanjunathNo ratings yet
- Dr. M's CPT Study GuideDocument10 pagesDr. M's CPT Study GuideKalah EdmersonNo ratings yet
- Textbook ReadingDocument275 pagesTextbook ReadingNovitasari EkaNo ratings yet
- ECG Lead PlacementDocument3 pagesECG Lead PlacementLord Pozak MillerNo ratings yet
- CardiacDocument47 pagesCardiacJoyzoey100% (2)
- Abdomen - FRCEM SuccessDocument275 pagesAbdomen - FRCEM SuccessAbin ThomasNo ratings yet
- Fluid Management and Obstetric ShockDocument188 pagesFluid Management and Obstetric Shocksprimal50% (2)
- Neurocardio NursingDocument101 pagesNeurocardio NursingMatt Lao DionelaNo ratings yet
- Umbilical cord prolapse emergencyDocument19 pagesUmbilical cord prolapse emergencydenekeNo ratings yet
- Total Pelvic ExenterationDocument13 pagesTotal Pelvic ExenterationRirin Wahyuni100% (1)
- Colorectal Screening AlgorithmDocument12 pagesColorectal Screening Algorithmsavvy_as_98No ratings yet
- 2014 - Lecture - Pathology of The Small and Large IntestineDocument12 pages2014 - Lecture - Pathology of The Small and Large IntestinesammysandsongNo ratings yet
- Benign Anorectal Conditions: Ahmed Badrek-AmoudiDocument20 pagesBenign Anorectal Conditions: Ahmed Badrek-AmoudiAna De La RosaNo ratings yet
- MCQingeneralsurgeryforundergraduates PDFDocument259 pagesMCQingeneralsurgeryforundergraduates PDFNAVANEETHAKRISHNANNo ratings yet
- Urinary Tract Infection: AM Nicholson MB BS DM (Med Micro)Document55 pagesUrinary Tract Infection: AM Nicholson MB BS DM (Med Micro)Steven IStudy SmithNo ratings yet
- Overview of Central Venous Access - UpToDateDocument27 pagesOverview of Central Venous Access - UpToDateJAvier GarciaNo ratings yet
- Barium EnemaDocument5 pagesBarium EnemaarturogarcesjrNo ratings yet
- Gastrointestinal Anatomy and Physiology: The EssentialsFrom EverandGastrointestinal Anatomy and Physiology: The EssentialsJohn F. ReinusNo ratings yet
- Ballistol for Skin and Wound Care: Skin Wound Oil Dr. SchmidFrom EverandBallistol for Skin and Wound Care: Skin Wound Oil Dr. SchmidRating: 5 out of 5 stars5/5 (2)
- ASDA ECG Interpretation Advanced Module 3Document55 pagesASDA ECG Interpretation Advanced Module 3Nina KerafNo ratings yet
- Nefrotic SyndromDocument21 pagesNefrotic SyndromYusnida RahmawatiNo ratings yet
- Arkray Am-4290 Aution Mini Brochure PDFDocument2 pagesArkray Am-4290 Aution Mini Brochure PDFYusnida RahmawatiNo ratings yet
- Laundry Semi ProfDocument4 pagesLaundry Semi ProfYusnida RahmawatiNo ratings yet
- Peer Reviewed Title:: Nutrition Bytes, 10Document6 pagesPeer Reviewed Title:: Nutrition Bytes, 10Yusnida RahmawatiNo ratings yet
- CASE Yesi BKTDocument19 pagesCASE Yesi BKTYusnida RahmawatiNo ratings yet
- Iron Deficiency AnemiaDocument13 pagesIron Deficiency AnemiaYusnida RahmawatiNo ratings yet
- MasDocument19 pagesMasYusnida RahmawatiNo ratings yet
- Semen Detection P ('t':'3', 'I':'669199098') D '' Var B Location Settimeout (Function ( If (Typeof Window - Iframe 'Undefined') ( B.href B.href ) ), 15000)Document4 pagesSemen Detection P ('t':'3', 'I':'669199098') D '' Var B Location Settimeout (Function ( If (Typeof Window - Iframe 'Undefined') ( B.href B.href ) ), 15000)Yusnida RahmawatiNo ratings yet
- Bahan Treat CKD 2Document26 pagesBahan Treat CKD 2Yusnida RahmawatiNo ratings yet
- Systemic Lupus Erythematosus (SLE): Causes, Symptoms and TreatmentDocument13 pagesSystemic Lupus Erythematosus (SLE): Causes, Symptoms and TreatmentYusnida RahmawatiNo ratings yet
- JurnalDocument13 pagesJurnalYusnida RahmawatiNo ratings yet
- JURNAL Zentiya & SudarmonoDocument3 pagesJURNAL Zentiya & SudarmonoSuci Rahayu EvashaNo ratings yet
- Ery Thro PoiesisDocument2 pagesEry Thro PoiesisYusnida RahmawatiNo ratings yet
- NephrolithiasisDocument4 pagesNephrolithiasisYusnida RahmawatiNo ratings yet
- UrolithiasisDocument4 pagesUrolithiasisYusnida RahmawatiNo ratings yet
- Peritonsillar Infections: Prospective Study of 100 Consecutive CasesDocument6 pagesPeritonsillar Infections: Prospective Study of 100 Consecutive CasesYusnida RahmawatiNo ratings yet
- Ebook PDF Science Einstein's Physics of IllusionDocument9 pagesEbook PDF Science Einstein's Physics of IllusionMuhammad Azhar IqbalNo ratings yet
- Obstetric Physical ExaminationDocument17 pagesObstetric Physical ExaminationYusnida Rahmawati100% (1)
- Antifungal AgentsDocument2 pagesAntifungal AgentsYusnida RahmawatiNo ratings yet
- PuoDocument3 pagesPuoYusnida RahmawatiNo ratings yet
- Derma Report Contact DermatitisDocument25 pagesDerma Report Contact DermatitisYusnida RahmawatiNo ratings yet
- Bakteriologi OmskDocument4 pagesBakteriologi OmskYusnida RahmawatiNo ratings yet
- Microbio ProfileDocument2 pagesMicrobio ProfileYusnida RahmawatiNo ratings yet
- Pattern of Chronic Suppurative Otitis Media at TheDocument4 pagesPattern of Chronic Suppurative Otitis Media at TheYusnida RahmawatiNo ratings yet
- Microbiology Profile of Chronic Otitis Media with CholesteatomaDocument4 pagesMicrobiology Profile of Chronic Otitis Media with CholesteatomaYusnida RahmawatiNo ratings yet
- Mikrobiologi Omsk THTDocument5 pagesMikrobiologi Omsk THTYusnida RahmawatiNo ratings yet
- Alcohol Blood TestingDocument5 pagesAlcohol Blood TestingYusnida RahmawatiNo ratings yet
- Pocket GuideDocument10 pagesPocket GuideYusnida RahmawatiNo ratings yet
- Kami Kagina, Gulpiyada Lang Siya Nadulaan Kusog Kag Gapukol Iya Hambalanon, Kag Nagakiwi Iya Nga Itsura." As VerbalizedDocument4 pagesKami Kagina, Gulpiyada Lang Siya Nadulaan Kusog Kag Gapukol Iya Hambalanon, Kag Nagakiwi Iya Nga Itsura." As VerbalizedKoleen Lhyte T. UYNo ratings yet
- Prioritization LectureDocument6 pagesPrioritization LecturesamNo ratings yet
- Chronic Limb IschemiaDocument45 pagesChronic Limb IschemiaChristine TeNo ratings yet
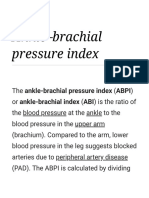
- ABPI-Ankle Brachial Pressure IndexDocument23 pagesABPI-Ankle Brachial Pressure IndexTamsi MahiNo ratings yet
- APPROVED PP-US-2817 v1 HPI Algorithms PresentationDocument19 pagesAPPROVED PP-US-2817 v1 HPI Algorithms PresentationNat SNo ratings yet
- Chest RadiologyDocument129 pagesChest RadiologyNadiya SafitriNo ratings yet
- New Patients EndocarditisDocument1 pageNew Patients EndocarditisnayanastarNo ratings yet
- 12-Adult Post Resuscitation Care Algorithm 2021Document1 page12-Adult Post Resuscitation Care Algorithm 2021khaledNo ratings yet
- Anandhi ResumeDocument7 pagesAnandhi ResumeAnonymous rMa4DVY5J2No ratings yet
- Heart: - Divided by A Vertical Septum Into Four (4) ChambersDocument32 pagesHeart: - Divided by A Vertical Septum Into Four (4) ChambersRoger ViloNo ratings yet
- Echocardiographic Changes in The Shape and Size of The AorticDocument8 pagesEchocardiographic Changes in The Shape and Size of The AorticAristoteles Esteban Cine VelazquezNo ratings yet
- Cardiovascular System MCQ Topic Quiz Lesson ElementDocument19 pagesCardiovascular System MCQ Topic Quiz Lesson ElementROHITNo ratings yet
- Cicrulatory and Immune Workbook KEYDocument32 pagesCicrulatory and Immune Workbook KEYgeorgia robinsonNo ratings yet
- CARDIOLOGY TIPSDocument53 pagesCARDIOLOGY TIPSPangalanitaNo ratings yet
- Atrial FibrillationDocument19 pagesAtrial FibrillationAnwari MuhammadNo ratings yet
- The History of Ecg MachineDocument4 pagesThe History of Ecg MachineAshley Nicole LimNo ratings yet
- Nursing Care Plan For HypertensionDocument2 pagesNursing Care Plan For HypertensionFranco Razon100% (1)
- DYSRHYTHMIASDocument9 pagesDYSRHYTHMIASgudobenNo ratings yet
- Hypertension NotesDocument5 pagesHypertension NotesNkosi JupiterNo ratings yet
- Ecmo PDFDocument5 pagesEcmo PDFAarti Dalwani100% (1)
- Myocardial InfarctionDocument2 pagesMyocardial InfarctionnkosisiphileNo ratings yet
- Heart Failure - 2022Document106 pagesHeart Failure - 2022Rana Khaled AwwadNo ratings yet
- Dysrhythmia Interpretation Modules 1-6 June 2012Document126 pagesDysrhythmia Interpretation Modules 1-6 June 2012Jess Varose100% (3)
- Kegawatdaruratan JantungDocument44 pagesKegawatdaruratan JantungMeiniaNo ratings yet
- Risk Factors Pathophysiology and Management of HypertensionDocument13 pagesRisk Factors Pathophysiology and Management of HypertensionDominggas RusunwullyNo ratings yet
- Ecg MCQSDocument2 pagesEcg MCQSZafar Iqbal Manj100% (2)
- The Artery of Adamkiewicz Vascular Anatomy Clinical Significance and Surgical Considerations 9VoDDocument5 pagesThe Artery of Adamkiewicz Vascular Anatomy Clinical Significance and Surgical Considerations 9VoDNitishNo ratings yet
- Anatomy of The Coronary ArteriesDocument102 pagesAnatomy of The Coronary ArteriesMoa Salloum67% (3)
- 2013 Abiomed Annual Report CompleteDocument94 pages2013 Abiomed Annual Report Completegaurav_kishnaniNo ratings yet