You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- ValedictionDocument6 pagesValedictionMarius Clifford BilledoNo ratings yet
- Philippines DOH Region 1 Nurse Program Report Sep 2015Document1 pagePhilippines DOH Region 1 Nurse Program Report Sep 2015Marius Clifford BilledoNo ratings yet
- Ready To Complete Your PNB Online Account Application We'Re Here For You. Ref. No. 2235@0931@08!20!2021@0033425Document3 pagesReady To Complete Your PNB Online Account Application We'Re Here For You. Ref. No. 2235@0931@08!20!2021@0033425Marius Clifford BilledoNo ratings yet
- Got TalentDocument1 pageGot TalentMarius Clifford BilledoNo ratings yet
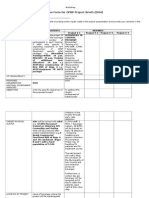
- Evaluation Form For GPBP Project Briefs (DOH) : Name of LGUDocument3 pagesEvaluation Form For GPBP Project Briefs (DOH) : Name of LGUMarius Clifford BilledoNo ratings yet
- Marius BsurDocument16 pagesMarius BsurMarius Clifford BilledoNo ratings yet
- Debut QuestionsDocument5 pagesDebut QuestionsMarius Clifford BilledoNo ratings yet
- Mr. Romeo Calderon and Mrs. Perla Caldero. Mr. Emanual Peralta Sr. and Mrs. Josefina PeraltaDocument4 pagesMr. Romeo Calderon and Mrs. Perla Caldero. Mr. Emanual Peralta Sr. and Mrs. Josefina PeraltaMarius Clifford BilledoNo ratings yet
- Fashion ShowDocument2 pagesFashion ShowMarius Clifford BilledoNo ratings yet
- Universal Profiling Consolidation Matrix-March 11Document8 pagesUniversal Profiling Consolidation Matrix-March 11Marius Clifford BilledoNo ratings yet
- Date/ Time Activity Venue Persons Involve: Barangay PoblacionDocument5 pagesDate/ Time Activity Venue Persons Involve: Barangay PoblacionMarius Clifford BilledoNo ratings yet
- Ans KeyDocument63 pagesAns KeyMarius Clifford BilledoNo ratings yet
- Tsekap NarativeDocument3 pagesTsekap NarativeMarius Clifford BilledoNo ratings yet
- 2016 June Case StudyDocument8 pages2016 June Case StudyMarius Clifford BilledoNo ratings yet
- Philippines DOH Region 1 Nurse Program Report Sep 2015Document1 pagePhilippines DOH Region 1 Nurse Program Report Sep 2015Marius Clifford BilledoNo ratings yet
- Philippines DOH Region 1 Nurse Program Report Sep 2015Document1 pagePhilippines DOH Region 1 Nurse Program Report Sep 2015Marius Clifford BilledoNo ratings yet
- Nryli ReportDocument1 pageNryli ReportMarius Clifford BilledoNo ratings yet
- Ans KeyDocument36 pagesAns KeyMarius Clifford BilledoNo ratings yet
- Nursing Care Plan for Fluid Volume Excess and Activity IntoleranceDocument4 pagesNursing Care Plan for Fluid Volume Excess and Activity IntoleranceMarius Clifford BilledoNo ratings yet
- ResumeDocument6 pagesResumeMarius Clifford BilledoNo ratings yet
- March ReportDocument9 pagesMarch ReportMarius Clifford BilledoNo ratings yet
- NCPDocument4 pagesNCPMarius Clifford BilledoNo ratings yet
- Nursing Care Plan: Assessment Nursing Diagnosis Nursing Objectives Intervention Rationale EvaluationDocument1 pageNursing Care Plan: Assessment Nursing Diagnosis Nursing Objectives Intervention Rationale EvaluationMarius Clifford BilledoNo ratings yet
- DRUG Study FormatDocument1 pageDRUG Study FormatMarius Clifford BilledoNo ratings yet
- Peer Facis - bencHMARKING (BSAccountancy)Document7 pagesPeer Facis - bencHMARKING (BSAccountancy)Marius Clifford BilledoNo ratings yet
- Impact of Culture To Family StructureDocument3 pagesImpact of Culture To Family StructureMarius Clifford BilledoNo ratings yet
- Impact of Culture To Family StructureDocument3 pagesImpact of Culture To Family StructureMarius Clifford BilledoNo ratings yet
- Impact of Culture To Family StructureDocument3 pagesImpact of Culture To Family StructureMarius Clifford BilledoNo ratings yet
- MariusDocument5 pagesMariusMarius Clifford BilledoNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)