You might also like
- Community As ClientDocument13 pagesCommunity As ClientVirus50% (2)
- ETP Flexible Eating GuideDocument61 pagesETP Flexible Eating Guidecoachhand100% (1)
- CHN - Community DiagnosisDocument45 pagesCHN - Community DiagnosisStudentnurseMj100% (1)
- 3 Heart InternetNewDocument55 pages3 Heart InternetNewCoral Srinivasa RamaluNo ratings yet
- Community Assessment and DiagnosisDocument25 pagesCommunity Assessment and DiagnosisVince Patrick LeonidaNo ratings yet
- Fetus & Neoborn-3Document25 pagesFetus & Neoborn-3Mateen Shukri100% (1)
- Community Health Nursing ProcessDocument23 pagesCommunity Health Nursing ProcessMaureen A. Bawang0% (1)
- CHNIMODULEIDocument44 pagesCHNIMODULEIlagumbayjoviann1No ratings yet
- Shape Shifter Yoga Starter ManualDocument25 pagesShape Shifter Yoga Starter ManualVernetteNg100% (1)
- Learning Material-Community Health Nursing ProcessDocument52 pagesLearning Material-Community Health Nursing Processzebzeb STEMANo ratings yet
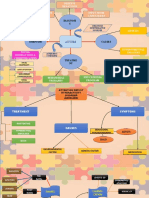
- Mind MapDocument3 pagesMind MapaziemNo ratings yet
- ASA Physical Status ClassificationDocument1 pageASA Physical Status ClassificationАндрій ДанильцівNo ratings yet
- Assessing Community Health NeedsDocument17 pagesAssessing Community Health NeedsClarissa Isuriña100% (2)
- Elements of A Comprehensive Community DiagnosisDocument6 pagesElements of A Comprehensive Community DiagnosisAila Hinlog100% (8)
- CHN 005Document14 pagesCHN 005betiful100% (5)
- Diseases of Poultry A Colour AtlasDocument213 pagesDiseases of Poultry A Colour AtlasShakil Mahmod100% (1)
- The Community DiagnosisDocument11 pagesThe Community DiagnosisAize Francisco100% (2)
- NCM 113 - Community Health Nursing 2 Community DiagnosisDocument10 pagesNCM 113 - Community Health Nursing 2 Community DiagnosisFrancheska Kyla GomezNo ratings yet
- Community Health Nursing ProcessDocument6 pagesCommunity Health Nursing ProcessAmiel Francisco ReyesNo ratings yet
- CHN NotesDocument65 pagesCHN Noteslanie_jecielNo ratings yet
- Cirrhosis of LiverDocument35 pagesCirrhosis of LiverShazia Parveen100% (1)
- Community DiagnosisDocument30 pagesCommunity DiagnosisPaulo Galang83% (6)
- Disease Emergence and Resurgence: The Wildlife-Human ConnectionDocument402 pagesDisease Emergence and Resurgence: The Wildlife-Human ConnectionMaíra100% (1)
- Community Health Nursing Ii NUR204: Population Groups and Community As Clients)Document31 pagesCommunity Health Nursing Ii NUR204: Population Groups and Community As Clients)ZairaNo ratings yet
- WEEK 1 - Concept of CommunityDocument5 pagesWEEK 1 - Concept of Communitypoleene de leonNo ratings yet
- Community Health Nursing ReviewerDocument24 pagesCommunity Health Nursing ReviewergilpogsNo ratings yet
- CHN Lec Activity 1Document9 pagesCHN Lec Activity 1RickNo ratings yet
- The Community DiagnosisDocument5 pagesThe Community DiagnosisEries Lacanlale Lumba50% (4)
- New Health Systems: Integrated Care and Health Inequalities ReductionFrom EverandNew Health Systems: Integrated Care and Health Inequalities ReductionNo ratings yet
- Community Health Nursing ProcessDocument69 pagesCommunity Health Nursing ProcessDharylle CariñoNo ratings yet
- Birth AsphyxiaDocument27 pagesBirth AsphyxiaJaya Prabha100% (5)
- Epidemiology methods guide for researchDocument183 pagesEpidemiology methods guide for researchBekele AtnafuNo ratings yet
- Continuing Education in NursingDocument22 pagesContinuing Education in NursingOmie TumanguilNo ratings yet
- CommunityDocument6 pagesCommunityMyrrha TaganasNo ratings yet
- Micro TeachingDocument52 pagesMicro TeachingMatetzky Sapiter Bueno0% (1)
- Community Phc2 RleDocument12 pagesCommunity Phc2 Rleefermin_lovely100% (1)
- Community DiagnosisDocument27 pagesCommunity DiagnosislouvvhartNo ratings yet
- Community Needs Assessment HRDP COPAR 2013Document6 pagesCommunity Needs Assessment HRDP COPAR 2013Amiel Francisco Reyes100% (1)
- 2 Community AssessmentDocument35 pages2 Community AssessmentDrshahira MohamedNo ratings yet
- COMMUNITY HEALTH DIAGNOSISDocument22 pagesCOMMUNITY HEALTH DIAGNOSISkuruvagadda sagarNo ratings yet
- Community Health Nursing Process AssessmentDocument44 pagesCommunity Health Nursing Process AssessmentApril FlorendoNo ratings yet
- COMMUNITY HEALTH PROFILEDocument39 pagesCOMMUNITY HEALTH PROFILELuo Miyanda100% (1)
- Community-Diagnosis ReferenceDocument45 pagesCommunity-Diagnosis ReferenceAnonymous h2EnKyDbNo ratings yet
- Community Health Nursing ProcessDocument9 pagesCommunity Health Nursing ProcessJohn Lawrence YbanezNo ratings yet
- CHN Assignment (Answer)Document10 pagesCHN Assignment (Answer)buttercup_chrissieNo ratings yet
- CSAB Community Health NSG Process Com DiagnosisDocument36 pagesCSAB Community Health NSG Process Com DiagnosisG26 Panaguiton, JairaNo ratings yet
- CHN 2 NUR 1214 Week 5 Module 5 Assessment and DiagnosisDocument12 pagesCHN 2 NUR 1214 Week 5 Module 5 Assessment and DiagnosisLorraine Jazmine AquinoNo ratings yet
- COPAR Community Assessment 1Document3 pagesCOPAR Community Assessment 1Winter KimNo ratings yet
- The ROLE OF The Public Health Nurse-AnnievadneDocument39 pagesThe ROLE OF The Public Health Nurse-AnnievadneDolores BeeNo ratings yet
- Fa18-Fsn-016 Ans A4Document11 pagesFa18-Fsn-016 Ans A4Mehwish MughalNo ratings yet
- Community Assessment: Prepper by Nariman NOUHDocument25 pagesCommunity Assessment: Prepper by Nariman NOUHN NNo ratings yet
- A Community Is A Cluster of People With at Least One Common CharacteristicDocument7 pagesA Community Is A Cluster of People With at Least One Common CharacteristicWilliam Ezekiel JUju CustodioNo ratings yet
- Community Assessment and Community DiagnosisDocument4 pagesCommunity Assessment and Community DiagnosisLaurence ZernaNo ratings yet
- Study Guide For ExamDocument36 pagesStudy Guide For ExamCatherine Drew SimsNo ratings yet
- CHN Chapter 6Document6 pagesCHN Chapter 6Paulo Marie TanNo ratings yet
- Community Diagnosis:: Community Health Nursing ProcessDocument44 pagesCommunity Diagnosis:: Community Health Nursing Processlaydomingo11No ratings yet
- Planning Community Health InterventionsDocument5 pagesPlanning Community Health InterventionsJanisse CalaguiNo ratings yet
- Community DiagnosisDocument12 pagesCommunity DiagnosisRichard Onen100% (1)
- 6) Community Diagnosis 2011Document33 pages6) Community Diagnosis 2011Dinar Kartika HapsariNo ratings yet
- CHN II - ReviewerDocument34 pagesCHN II - ReviewerKarina Blanca Sanico AdranedaNo ratings yet
- Principles of CHN New UpdatedDocument4 pagesPrinciples of CHN New Updatediheart musicNo ratings yet
- BaliteDocument5 pagesBaliteRaymond Lee Montilla BaliteNo ratings yet
- PHC Community DiagnosisDocument27 pagesPHC Community DiagnosisCassandra_Maca_6324No ratings yet
- CHN2Document43 pagesCHN2Sidney Bon LuceroNo ratings yet
- Community Health Diagnosis GuideDocument2 pagesCommunity Health Diagnosis GuidekimerellaNo ratings yet
- Community Health Nursing Diagnosis & InterventionsDocument17 pagesCommunity Health Nursing Diagnosis & InterventionsMarthy BollenaNo ratings yet
- Community Diagnosis 2016-2Document14 pagesCommunity Diagnosis 2016-2wanjohiisaac84No ratings yet
- Community HealthDocument30 pagesCommunity HealthKeyceeleen Guevarra LimNo ratings yet
- Carmel Marie Venezuela - Nursing Process in The Care of Population Groups and Community ActivityDocument5 pagesCarmel Marie Venezuela - Nursing Process in The Care of Population Groups and Community ActivityCarmel Venezuela100% (1)
- Community AssessmentDocument9 pagesCommunity Assessmentرانيا احمد عبد الكريمNo ratings yet
- Meeting the Needs of Older Adults with Serious Illness: Challenges and Opportunities in the Age of Health Care ReformFrom EverandMeeting the Needs of Older Adults with Serious Illness: Challenges and Opportunities in the Age of Health Care ReformAmy S. KelleyNo ratings yet
- Nurse's Guide to Patient CareDocument30 pagesNurse's Guide to Patient CareOmie TumanguilNo ratings yet
- Drug Calculation SkillsDocument13 pagesDrug Calculation SkillsOmie TumanguilNo ratings yet
- Managing Diabetes and ComplicationsDocument35 pagesManaging Diabetes and ComplicationsOmie TumanguilNo ratings yet
- Reqtmsn PreDocument11 pagesReqtmsn PreOmie TumanguilNo ratings yet
- 01Document13 pages01Omie TumanguilNo ratings yet
- The National Health Plan-OutlineDocument9 pagesThe National Health Plan-OutlineOmie TumanguilNo ratings yet
- The National Health Plan-OutlineDocument9 pagesThe National Health Plan-OutlineOmie TumanguilNo ratings yet
- Problems 10th Revision (ICD-10) Is A Coding of Diseases and Signs, Symptoms, AbnormalDocument10 pagesProblems 10th Revision (ICD-10) Is A Coding of Diseases and Signs, Symptoms, AbnormalOmie TumanguilNo ratings yet
- Fields of NursingDocument8 pagesFields of NursingOmie TumanguilNo ratings yet
- Funda Bullet FormDocument11 pagesFunda Bullet FormannherreraNo ratings yet
- Ob DXDocument12 pagesOb DXOmie TumanguilNo ratings yet
- CNS Pathology StrokeDocument11 pagesCNS Pathology StrokeKamran Khan KhalilNo ratings yet
- Quaratine Isolation Center DesignDocument6 pagesQuaratine Isolation Center DesignYeabtsega ZelalemNo ratings yet
- Approach To Anemia Chalk Talk NotesDocument2 pagesApproach To Anemia Chalk Talk NotesMarl KarxNo ratings yet
- CIcloyd Psychosis Peralta CuestaDocument10 pagesCIcloyd Psychosis Peralta CuestaJuan IgnacioNo ratings yet
- Manual Muscle Test (MMT) : Ajith C Student of Department of Physio Kmch-CoptDocument80 pagesManual Muscle Test (MMT) : Ajith C Student of Department of Physio Kmch-Coptayesha solNo ratings yet
- Prevalence of Seizure and Prescribing Patterns of Aed in Patients With NeuroDocument120 pagesPrevalence of Seizure and Prescribing Patterns of Aed in Patients With NeurosnigdhaNo ratings yet
- Lecture 15 Cardiovascular DiseaseDocument19 pagesLecture 15 Cardiovascular DiseaseHHGV JGYGUNo ratings yet
- Reflexology Research PapersDocument10 pagesReflexology Research Paperskyle atienzaNo ratings yet
- Endocrinology: Differences Between Nervous and Endocrine SystemDocument34 pagesEndocrinology: Differences Between Nervous and Endocrine SystemRezaul RazibNo ratings yet
- Bakteri Anaerob: Morfologi, Fisiologi, Epidemiologi, Diagnosis, Pemeriksaan Sy. Miftahul El J.TDocument46 pagesBakteri Anaerob: Morfologi, Fisiologi, Epidemiologi, Diagnosis, Pemeriksaan Sy. Miftahul El J.TAlif NakyukoNo ratings yet
- Ate PatDocument31 pagesAte PatJerry ChioNo ratings yet
- MF2 - Spinal Cord InjuryDocument43 pagesMF2 - Spinal Cord InjuryAnnbe BarteNo ratings yet
- Pathomorphology FinalDocument216 pagesPathomorphology FinalAugustine A. KollieNo ratings yet
- 1st Bi PediaDocument19 pages1st Bi PediaBeo Adelynn - AiiyuNo ratings yet
- Granuloma Annulare TreatmentDocument2 pagesGranuloma Annulare Treatmentjohn martenNo ratings yet
- Common Medical AbbreviationsDocument4 pagesCommon Medical AbbreviationsApril Joy de LimaNo ratings yet
- Diet Prevents Polio by Maintaining Normal Blood SugarDocument69 pagesDiet Prevents Polio by Maintaining Normal Blood SugarIyemhetepNo ratings yet
- 04 InfectionDocument18 pages04 InfectionMalinda KarunaratneNo ratings yet