You might also like
- History & Physical Examination of The ShoulderDocument53 pagesHistory & Physical Examination of The ShoulderzaimmuhtarNo ratings yet
- Physiotherapy For Osteoarthritis of The Knee PDFDocument391 pagesPhysiotherapy For Osteoarthritis of The Knee PDFPipi KNo ratings yet
- Skills Acquisition and Physiatric Evaluation Positive ResultDocument1 pageSkills Acquisition and Physiatric Evaluation Positive ResultJonathan Salvador GuinabayNo ratings yet
- Manual Therapy RecoveryDocument263 pagesManual Therapy RecoveryMfxMazprofxNo ratings yet
- The Guideline For Standing SCI Mascip FinalDocument30 pagesThe Guideline For Standing SCI Mascip FinalJavierSanMartínHerreraNo ratings yet
- Shoulderexaminationppt 180505152418Document19 pagesShoulderexaminationppt 180505152418KarthickNo ratings yet
- Examination of The ShoulderDocument20 pagesExamination of The ShoulderMalvino Giovanni100% (1)
- CervicothoracicSpine AssessmentDocument16 pagesCervicothoracicSpine AssessmentKanika SinhaNo ratings yet
- Cervical Assessment Form 2014Document2 pagesCervical Assessment Form 2014Mark Koval100% (1)
- Assessment FormDocument2 pagesAssessment FormDeepi GurungNo ratings yet
- Tennis Elbow JOSPT ArticleDocument11 pagesTennis Elbow JOSPT ArticleHasan RahmanNo ratings yet
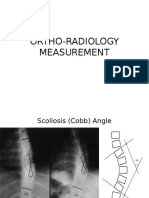
- Ortho Radiology MeasurementDocument25 pagesOrtho Radiology MeasurementNasrul Ha100% (1)
- Thermotherapy: by Ren Peterson, Laurel Petersen, Jason Neilsen, Angela PerkinsDocument104 pagesThermotherapy: by Ren Peterson, Laurel Petersen, Jason Neilsen, Angela PerkinsMaheswari DuraiNo ratings yet
- Certificate of Medical Necessity Dmerc 10.02BDocument2 pagesCertificate of Medical Necessity Dmerc 10.02BjackNo ratings yet
- CMS Form Approves Seat Lift Medical NecessityDocument2 pagesCMS Form Approves Seat Lift Medical NecessityLety Munoz NeffNo ratings yet
- Philhealth cf4Document6 pagesPhilhealth cf4Jose AcuinNo ratings yet
- Dme Information Form Cms-10125 - External Infusion PumpsDocument2 pagesDme Information Form Cms-10125 - External Infusion PumpsSonof GoddNo ratings yet
- EASYHCFA486Document2 pagesEASYHCFA486lokohugpoNo ratings yet
- Genre AnalysisDocument6 pagesGenre Analysisapi-508703903No ratings yet
- Health PDFDocument25 pagesHealth PDFShurieUNo ratings yet
- Others Claim FormDocument5 pagesOthers Claim FormArvind RayNo ratings yet
- Medical Billing Process: Naveen MajetyDocument21 pagesMedical Billing Process: Naveen MajetyNaveen KumarNo ratings yet
- SSS Form CLD-9NDocument2 pagesSSS Form CLD-9NCat LedesmaNo ratings yet
- OASIS Patient History GuidanceDocument20 pagesOASIS Patient History GuidancebiskwetNo ratings yet
- Sss 02Document2 pagesSss 02June CruzNo ratings yet
- PhilHealth Circular No. 0035, s.2013 Annex11 - GuidelinesOnTheProperAccomplishmentOfClaimForm2 (November2013)Document8 pagesPhilHealth Circular No. 0035, s.2013 Annex11 - GuidelinesOnTheProperAccomplishmentOfClaimForm2 (November2013)Chrysanthus HerreraNo ratings yet
- Medical Billing ProcessDocument24 pagesMedical Billing ProcessNajamHass100% (5)
- Spo Metode Komunikasi SbarDocument3 pagesSpo Metode Komunikasi SbaramihcimilNo ratings yet
- Nhs England Ifr FormDocument10 pagesNhs England Ifr FormdanielNo ratings yet
- GNP - Informe Médico y Aviso de Accidente o Enfermedad 20190510 Editable - Es.enDocument6 pagesGNP - Informe Médico y Aviso de Accidente o Enfermedad 20190510 Editable - Es.enSalai Nayagan ArunmozhiNo ratings yet
- DOH-4359 (2010) Physician'S Order For Personal Care/Consumer Directed Personal Assistance ServicesDocument4 pagesDOH-4359 (2010) Physician'S Order For Personal Care/Consumer Directed Personal Assistance ServicesRebeca MartínezNo ratings yet
- MDINDIA Healthcare Services Claim Form GuideDocument4 pagesMDINDIA Healthcare Services Claim Form GuideShubakar ReddyNo ratings yet
- California Primary Treating Physician Progress ReportDocument2 pagesCalifornia Primary Treating Physician Progress ReportAlyssa DavidNo ratings yet
- Medicare Medicaid Health Insurance Claim Form DetailsDocument2 pagesMedicare Medicaid Health Insurance Claim Form Detailstmnunes0419No ratings yet
- CMS-485 Certification Training GuideDocument56 pagesCMS-485 Certification Training GuideManisha Tidke100% (1)
- EPC Referral FormDocument1 pageEPC Referral Formwaterbearer85No ratings yet
- PhilHealth Circular No. 0035, s.2013 Annex11 - PhilHealthClaimForm2 (Revisednovember2013)Document2 pagesPhilHealth Circular No. 0035, s.2013 Annex11 - PhilHealthClaimForm2 (Revisednovember2013)Chrysanthus HerreraNo ratings yet
- DJPRH Processes and ProceduresDocument289 pagesDJPRH Processes and ProceduresjeffaguilarNo ratings yet
- Vhis Claimable Amount Estimate Preliminary Assessment Request FormDocument2 pagesVhis Claimable Amount Estimate Preliminary Assessment Request FormMartin StephanNo ratings yet
- QCIDocument27 pagesQCIerpNo ratings yet
- Health Care Provider ReportDocument2 pagesHealth Care Provider ReportsiskjereNo ratings yet
- GW Hospital MOU & Observer Health Information FormDocument2 pagesGW Hospital MOU & Observer Health Information Formengel0321hotmail.comNo ratings yet
- NapulanRM - Health Records Analysis and Clinical AuditDocument64 pagesNapulanRM - Health Records Analysis and Clinical AuditJeffreyReyesNo ratings yet
- Claims Reimbursement Form GuideDocument2 pagesClaims Reimbursement Form Guideathenixia100% (1)
- Module 4 HA Documentation and ReportingDocument9 pagesModule 4 HA Documentation and ReportingCalvo AdrianNo ratings yet
- 4a - Patient Registration FormDocument7 pages4a - Patient Registration FormHygiena Kumala SuciNo ratings yet
- Claims Reimbursement Form: Member General InformationDocument1 pageClaims Reimbursement Form: Member General InformationHarold TanNo ratings yet
- Deficiency of Case SheetDocument15 pagesDeficiency of Case SheetberliyaNo ratings yet
- Nurse Delegation Consent FormDocument2 pagesNurse Delegation Consent FormArry FirmansyahNo ratings yet
- Claims Reimbursement Form: Member General InformationDocument1 pageClaims Reimbursement Form: Member General InformationFirmament DevelopmentNo ratings yet
- Med Record Auditor - Sample PagesDocument5 pagesMed Record Auditor - Sample PagesDaniel O. FernandezNo ratings yet
- Template Registration Form and Consent Form V3 - Final For RPSDocument7 pagesTemplate Registration Form and Consent Form V3 - Final For RPSHamdi PutraNo ratings yet
- APTRANSCO-Form of Application For Medical ClaimsDocument6 pagesAPTRANSCO-Form of Application For Medical ClaimsmastiNo ratings yet
- PatientCareDocDocument15 pagesPatientCareDocAra- Cvsu Francisco100% (2)
- Florida Workers' Compensation FormDocument18 pagesFlorida Workers' Compensation FormYenitze PerezNo ratings yet
- Writing SOAP Notes NYCCDocument7 pagesWriting SOAP Notes NYCCmassagekevin100% (2)
- WORK SHEET EXP RajDocument2 pagesWORK SHEET EXP RajCOVID19 RECEPTION RITMNo ratings yet
- Claim Form (Out Patient + Hospitalisation)Document2 pagesClaim Form (Out Patient + Hospitalisation)ahsan_hayat28660% (1)
- N342 CareplanDocument4 pagesN342 CareplanC'klov Ag'ilNo ratings yet
- 2 Reporting EndorsementDocument16 pages2 Reporting Endorsementcarla yganNo ratings yet
- Sign 110Document84 pagesSign 110speedo78No ratings yet
- Pathophysiology of Postpartum HemorrhageDocument2 pagesPathophysiology of Postpartum HemorrhageroxaynnnNo ratings yet
- Occupational Therapy As A Major Activity of Human Being: by Rafia KhalidDocument20 pagesOccupational Therapy As A Major Activity of Human Being: by Rafia Khalidnomi9818No ratings yet
- Training English Individual Task Lecturers: Umi Rachmawati, M.PDDocument14 pagesTraining English Individual Task Lecturers: Umi Rachmawati, M.PDVeni UNNo ratings yet
- Beauty Care NC IIDocument84 pagesBeauty Care NC IIMairem BarrugaNo ratings yet
- BSBHRM506 Assessment 1Document9 pagesBSBHRM506 Assessment 1prasannareddy9989No ratings yet
- Philippine Traditional Games and SportsDocument12 pagesPhilippine Traditional Games and SportsJohn Peter BermudoNo ratings yet
- Operational Guidelines On Limited Face To Face ImplementationDocument36 pagesOperational Guidelines On Limited Face To Face ImplementationJohn Paul light100% (3)
- Restless Leg Syndrome Part 1Document2 pagesRestless Leg Syndrome Part 1Faried MananNo ratings yet
- Oct DirDocument81 pagesOct DirsinfhmukulNo ratings yet
- 2013 Sample Psychology Cover LettersDocument2 pages2013 Sample Psychology Cover LettersLavander Meggie100% (1)
- The Medical Letter: On Drugs and TherapeuticsDocument4 pagesThe Medical Letter: On Drugs and TherapeuticsbippityNo ratings yet
- Work-Life Balance - Facebook Com LinguaLIBDocument257 pagesWork-Life Balance - Facebook Com LinguaLIBDiegoAngeles100% (1)
- Stroke Anti CoagulationDocument26 pagesStroke Anti CoagulationdoctormussieaberraNo ratings yet
- Ss811e MSDS enDocument11 pagesSs811e MSDS enJeric SalcedoNo ratings yet
- An Auricular Marker For Covid-19: Nadia Volf, MD, PHD, Valery Salques, MD, and Anne Lassaux, MDDocument2 pagesAn Auricular Marker For Covid-19: Nadia Volf, MD, PHD, Valery Salques, MD, and Anne Lassaux, MDyan92120No ratings yet
- 10 WinterDocument48 pages10 WintercontinentdriftNo ratings yet
- "Extreme" Cosmetic Surgery: A Retrospective Study of Morbidity in Patients Undergoing Combined ProceduresDocument5 pages"Extreme" Cosmetic Surgery: A Retrospective Study of Morbidity in Patients Undergoing Combined ProceduresDakirdaNo ratings yet
- DWATCHDocument92 pagesDWATCHFawaz SayedNo ratings yet
- Nursing Student Cover LetterDocument8 pagesNursing Student Cover Letterafmrpaxgfqdkor100% (1)
- Irritable Bowel SyndromeDocument22 pagesIrritable Bowel SyndromeMarium NabeelNo ratings yet
- Risk Factors in Dental ErosionDocument6 pagesRisk Factors in Dental ErosionMuftihat IsrarNo ratings yet
- Expanding Designed Exercise Awareness and Produced by Gregory Petrovich GrabovoiDocument5 pagesExpanding Designed Exercise Awareness and Produced by Gregory Petrovich GrabovoiManojkumar NairNo ratings yet
- How To Maintain Interpersonal RelationshipsDocument5 pagesHow To Maintain Interpersonal RelationshipsRichard BryanNo ratings yet
- DM No. 2022-0298 Implementation of The HFP System in All Government and Private Hospitals, Infirmaries and Primary Care Facilities in The PhilippinesDocument5 pagesDM No. 2022-0298 Implementation of The HFP System in All Government and Private Hospitals, Infirmaries and Primary Care Facilities in The PhilippinesRhodora BenipayoNo ratings yet
- Pengetahuan Ergonomi Dan Postur Kerja Perawat Pada Perawatan Luka Dengan Gangguan Muskuloskeletal Di Dr. H. Koesnadi BondowosoDocument5 pagesPengetahuan Ergonomi Dan Postur Kerja Perawat Pada Perawatan Luka Dengan Gangguan Muskuloskeletal Di Dr. H. Koesnadi BondowosoImanuel SihotangNo ratings yet
- School ProspectDocument16 pagesSchool ProspectJeynalNo ratings yet
- Case HistoryDocument32 pagesCase HistoryHogan ObiNo ratings yet
- Daftar Isi Bridwell SpineDocument38 pagesDaftar Isi Bridwell Spineronny0% (1)
- Strokeaha 120 030653Document5 pagesStrokeaha 120 030653indanazulfaaNo ratings yet