You might also like
- Donation Letter ChangesDocument1 pageDonation Letter ChangesAnonymous kprzCiZNo ratings yet
- Emails Over Conway's HarassmentDocument5 pagesEmails Over Conway's HarassmentAnonymous kprzCiZNo ratings yet
- Notice of Impending LawsuitDocument5 pagesNotice of Impending LawsuitAnonymous kprzCiZNo ratings yet
- Xcel Application 2016Document11 pagesXcel Application 2016Anonymous kprzCiZNo ratings yet
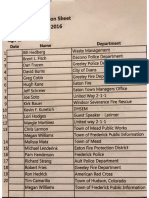
- Non County EOC AttendeesDocument1 pageNon County EOC AttendeesAnonymous kprzCiZNo ratings yet
- NAACP Resolution On Charter Schools - Colorado CounterpointDocument1 pageNAACP Resolution On Charter Schools - Colorado CounterpointAnonymous kprzCiZNo ratings yet
- Colorado Ballots Return UpdateDocument1 pageColorado Ballots Return UpdateAnonymous kprzCiZNo ratings yet
- IRS PublicationsDocument3 pagesIRS PublicationsAnonymous kprzCiZNo ratings yet
- Colorado Ballots Return UpdateDocument1 pageColorado Ballots Return UpdateAnonymous kprzCiZNo ratings yet
- Madden Application LetterDocument1 pageMadden Application LetterAnonymous kprzCiZNo ratings yet
- Xcel Meeting RequestDocument1 pageXcel Meeting RequestAnonymous kprzCiZNo ratings yet
- Shoemaker Madden CU New Job 2Document2 pagesShoemaker Madden CU New Job 2Anonymous kprzCiZNo ratings yet
- Xcel EmailsDocument6 pagesXcel EmailsAnonymous kprzCiZNo ratings yet
- Bill Garcia ExpenseDocument2 pagesBill Garcia ExpenseAnonymous kprzCiZNo ratings yet
- Roberts Email ColoradoDocument1 pageRoberts Email ColoradoAnonymous kprzCiZNo ratings yet
- Shoemaker Madden CU New JobDocument2 pagesShoemaker Madden CU New JobAnonymous kprzCiZNo ratings yet
- Shoemaker Independent ExpenditureDocument1 pageShoemaker Independent ExpenditureAnonymous kprzCiZNo ratings yet
- Group List of Extra Scrutiny Targets by IRSDocument10 pagesGroup List of Extra Scrutiny Targets by IRSAnonymous kprzCiZNo ratings yet
- CU Law School FinalistsDocument1 pageCU Law School FinalistsAnonymous kprzCiZNo ratings yet
- Email 38 in Our Pocket DOC WMDocument2 pagesEmail 38 in Our Pocket DOC WMAnonymous kprzCiZNo ratings yet
- Applied Trust LewisPalmerSchool Incident Review 2016-07-28Document1 pageApplied Trust LewisPalmerSchool Incident Review 2016-07-28Anonymous kprzCiZNo ratings yet
- Email 13 Purpose of The RequestDocument1 pageEmail 13 Purpose of The RequestAnonymous kprzCiZNo ratings yet
- FCC Emails Wheeler Krone WatermarkedDocument3 pagesFCC Emails Wheeler Krone WatermarkedAnonymous kprzCiZNo ratings yet
- Workers' Comp Handbook GuidanceDocument2 pagesWorkers' Comp Handbook GuidanceAnonymous kprzCiZNo ratings yet
- 16.07.12 - Order Granting Motion For SJDocument6 pages16.07.12 - Order Granting Motion For SJAnonymous kprzCiZNo ratings yet
- Fiscal Note 2005 HB 1139 ColoradoDocument3 pagesFiscal Note 2005 HB 1139 ColoradoAnonymous kprzCiZNo ratings yet
- HealthOP LetterDocument1 pageHealthOP LetterAnonymous kprzCiZNo ratings yet
- HealthOP Response From HollowayDocument1 pageHealthOP Response From HollowayAnonymous kprzCiZNo ratings yet
- ColoradoCare Cease and Desist LetterDocument2 pagesColoradoCare Cease and Desist LetterAnonymous kprzCiZNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5782)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Guide Questions For ARTICLE Forget Developing Poor CountriesDocument2 pagesGuide Questions For ARTICLE Forget Developing Poor CountriesWindel L GabuyaNo ratings yet
- Urdu Digital Books Survey Assesses Future GrowthDocument9 pagesUrdu Digital Books Survey Assesses Future GrowthQamar Hussain MulghaniNo ratings yet
- The SNU Quill - Volume 46Document22 pagesThe SNU Quill - Volume 46The SNU QuillNo ratings yet
- E-M-E-, AXXX XXX 420 (BIA Jan. 31, 2012)Document4 pagesE-M-E-, AXXX XXX 420 (BIA Jan. 31, 2012)Immigrant & Refugee Appellate Center, LLCNo ratings yet
- Thoo Brahmanwad - DR BR Ambedkar BooksDocument294 pagesThoo Brahmanwad - DR BR Ambedkar BooksAdhar_Chawhan100% (1)
- List of Guidelines Shifted To Archive: //192.168.4.1/e/public Enterprises (2018) /4077PE/4077PE (Annexure)Document36 pagesList of Guidelines Shifted To Archive: //192.168.4.1/e/public Enterprises (2018) /4077PE/4077PE (Annexure)vivekkaushikNo ratings yet
- Guidelines For Verification of Genuineness of Educational CertificateDocument4 pagesGuidelines For Verification of Genuineness of Educational CertificatephysicspalanichamyNo ratings yet
- The Great World WarDocument2 pagesThe Great World WarWilliam SmithNo ratings yet
- Dr. Paul Cameron - Psychiatric Professions Falsely Claim Gays No More Apt To MolestDocument13 pagesDr. Paul Cameron - Psychiatric Professions Falsely Claim Gays No More Apt To MolestRuben MicleaNo ratings yet
- Dossier The Secret History of Armand Hammer PDFDocument2 pagesDossier The Secret History of Armand Hammer PDFsorin birou100% (1)
- Strategic Uncertainty and Environmental Scanning: The Case For Institutional Influences On Scanning BehaviorDocument17 pagesStrategic Uncertainty and Environmental Scanning: The Case For Institutional Influences On Scanning BehaviorMohamed ShaminNo ratings yet
- 6 Reason Why We Agree With Polygamy: 1. Qur'an Permits Limited Polygamy. Before The Qur'an Was Revealed, ThereDocument3 pages6 Reason Why We Agree With Polygamy: 1. Qur'an Permits Limited Polygamy. Before The Qur'an Was Revealed, ThereMad DanNo ratings yet
- Lazaro Vs Social Security Commission GR 138254Document3 pagesLazaro Vs Social Security Commission GR 138254George PandaNo ratings yet
- Chapter 13 Rizal Visit UsDocument2 pagesChapter 13 Rizal Visit UsLance Axel Husana63% (8)
- PP v Fabian Anuar Mail High Court Ruling on Anti-Corruption ChargesDocument7 pagesPP v Fabian Anuar Mail High Court Ruling on Anti-Corruption ChargesAlias IbrahimNo ratings yet
- Free Legal Form: Vehicle Deed of SaleDocument2 pagesFree Legal Form: Vehicle Deed of SaleArchie Joseph LlanaNo ratings yet
- Africa Must Unite PDFDocument244 pagesAfrica Must Unite PDFEvelyneBrenerNo ratings yet
- Landcenter vs Ponce Rule 17 DismissalDocument1 pageLandcenter vs Ponce Rule 17 DismissalLynne SanchezNo ratings yet
- Gender and Development (Gad)Document4 pagesGender and Development (Gad)Romar TaroyNo ratings yet
- Race MixingDocument2 pagesRace MixingmansuradjvNo ratings yet
- Full Download Test Bank For Governing States and Localities 7th Edition Kevin B Smith Alan Greenblatt PDF Full ChapterDocument36 pagesFull Download Test Bank For Governing States and Localities 7th Edition Kevin B Smith Alan Greenblatt PDF Full Chaptergulessideslip.22kz100% (14)
- Short Quiz 013 PDFDocument6 pagesShort Quiz 013 PDFAaron PaulNo ratings yet
- RWDSDocument20 pagesRWDSJ RohrlichNo ratings yet
- 33 - Constituency Wise Detailed ResultDocument492 pages33 - Constituency Wise Detailed ResultAbhishek SachdevNo ratings yet
- Civil Procedure: I. COMPLAINT (In Some ActionsDocument3 pagesCivil Procedure: I. COMPLAINT (In Some ActionsKris Razo0% (1)
- Jail Inquiry Details2Document2 pagesJail Inquiry Details2Policeabuse.comNo ratings yet
- Lawrence v. State Tax Comm'n of Miss., 286 U.S. 276 (1932)Document6 pagesLawrence v. State Tax Comm'n of Miss., 286 U.S. 276 (1932)Scribd Government DocsNo ratings yet
- The Government of Philippine IslandsDocument825 pagesThe Government of Philippine IslandsRhenmar Morales GalvezNo ratings yet
- 103558Document18 pages103558محمود محمدNo ratings yet