You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- QuickStudy - Lymphatic SystemDocument2 pagesQuickStudy - Lymphatic SystemEmina Borovac100% (2)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Superficial Parotidectomy TRZDocument20 pagesSuperficial Parotidectomy TRZdokteraan100% (3)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Index: Use CTRL + Home To Return To The First PageDocument41 pagesIndex: Use CTRL + Home To Return To The First Pagesurendra reddy100% (9)
- HOMEOSTASIS - Lecture (Human Biology)Document22 pagesHOMEOSTASIS - Lecture (Human Biology)dokteraanNo ratings yet
- Acute Limb Ischemia SiteDocument23 pagesAcute Limb Ischemia Sitedokteraan100% (2)
- 1.principles of Oral SurgeryDocument13 pages1.principles of Oral SurgerydrpnnreddyNo ratings yet
- Anesthesia in Day Care SurgeryDocument143 pagesAnesthesia in Day Care SurgeryGmkmcNo ratings yet
- NP3. Nursing Board Exam November 2008 Answer KeyDocument12 pagesNP3. Nursing Board Exam November 2008 Answer KeyAlyssa Mier Dacua Patalinjug100% (1)
- MCQs Surgery Liaqat-FarhanDocument22 pagesMCQs Surgery Liaqat-Farhanasim shehzad100% (1)
- Nursing Test 4 (NP Iii)Document16 pagesNursing Test 4 (NP Iii)Yuxin Liu100% (2)
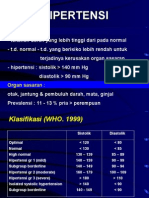
- HipertensiDocument28 pagesHipertensidokteraanNo ratings yet
- History of Plastic Surgery: From Ancient Times to Modern MicrosurgeryDocument21 pagesHistory of Plastic Surgery: From Ancient Times to Modern MicrosurgeryPaul David Zamora AlarconNo ratings yet
- Doctors ListDocument6 pagesDoctors ListDcStrokerehabNo ratings yet
- Nle 3Document6 pagesNle 3Aijem RyanNo ratings yet
- Compartment SyndromeDocument14 pagesCompartment SyndromedokteraanNo ratings yet
- 12 DHF DRDocument56 pages12 DHF DRdokteraanNo ratings yet
- TRIGONUM RevisiDocument5 pagesTRIGONUM RevisidokteraanNo ratings yet
- Hotchkiss 2013Document13 pagesHotchkiss 2013dokteraanNo ratings yet
- Pelvic Fracture-Related Injuries of The Bladder Neck andDocument12 pagesPelvic Fracture-Related Injuries of The Bladder Neck anddokteraanNo ratings yet
- Inguinal HerniaDocument14 pagesInguinal HerniaSakinah Mar'ie SanadNo ratings yet
- Guide to Head and Neck Physical ExamDocument39 pagesGuide to Head and Neck Physical ExamdokteraanNo ratings yet
- TRIGONUM RevisiDocument5 pagesTRIGONUM RevisidokteraanNo ratings yet
- TRIGONUM RevisiDocument5 pagesTRIGONUM RevisidokteraanNo ratings yet
- Abdominal Anatomy For GIST: The Peritoneum and RetroperitoneumDocument5 pagesAbdominal Anatomy For GIST: The Peritoneum and RetroperitoneumdokteraanNo ratings yet
- A B S T R A C TDocument2 pagesA B S T R A C TdokteraanNo ratings yet
- PneumothoraxDocument17 pagesPneumothoraxRizal FadhlurrahmanNo ratings yet
- Barrett Farm FoodDocument1 pageBarrett Farm FooddokteraanNo ratings yet
- Zometa PI Nov2004Document23 pagesZometa PI Nov2004dokteraanNo ratings yet
- Bonefos PM Eng 22feb2007 112121Document27 pagesBonefos PM Eng 22feb2007 112121dokteraanNo ratings yet
- Guide to Decompressive Craniectomy for Severe Head InjuryDocument8 pagesGuide to Decompressive Craniectomy for Severe Head InjurydokteraanNo ratings yet
- Output PathDocument4 pagesOutput PathdokteraanNo ratings yet
- Cuci Tangan, Sarung Tangan, Gaun Dan Mask 05.06Document18 pagesCuci Tangan, Sarung Tangan, Gaun Dan Mask 05.06Dewi Ayu Puspitasari TwinNo ratings yet
- Cancer Is An Abnormal Disorganised Growth of Cells in The: PrintDocument1 pageCancer Is An Abnormal Disorganised Growth of Cells in The: Printshailesh284No ratings yet
- Gastroscizis IngDocument1 pageGastroscizis IngdokteraanNo ratings yet
- Handbook of PEDIATRIC SURGERY PDFDocument43 pagesHandbook of PEDIATRIC SURGERY PDFPETERNo ratings yet
- CUPS Pediatric Trauma EvaluationDocument2 pagesCUPS Pediatric Trauma EvaluationdokteraanNo ratings yet
- Good Surgical PracticeDocument10 pagesGood Surgical PracticedokteraanNo ratings yet
- Good Surgical PracticeDocument10 pagesGood Surgical PracticedokteraanNo ratings yet
- Lay Out LT 2Document1 pageLay Out LT 2dokteraanNo ratings yet
- Presentación Proyecto Trabajo Doodle Orgánico MulticolorDocument11 pagesPresentación Proyecto Trabajo Doodle Orgánico MulticolorcamilleNo ratings yet
- Evans Endoscopic InstrumentDocument2 pagesEvans Endoscopic InstrumentsigmakarsaNo ratings yet
- Sps. Flores v. Sps. PinedaDocument7 pagesSps. Flores v. Sps. PinedaRachel CayangaoNo ratings yet
- Suture BootiesDocument1 pageSuture Bootiespatrickkalmeida6565No ratings yet
- OS 2 Module 5 ReportDocument151 pagesOS 2 Module 5 ReportChristineMartinNo ratings yet
- Final Peds Concept MapDocument9 pagesFinal Peds Concept Mapapi-495456666No ratings yet
- Periosteal Releasing Incision For Successful Coverage of Augmented Sites. A Technical NoteDocument6 pagesPeriosteal Releasing Incision For Successful Coverage of Augmented Sites. A Technical NotemaxNo ratings yet
- Barber-Effects Hypnosis PainDocument31 pagesBarber-Effects Hypnosis PainEzzat Abdelhafeez SalemNo ratings yet
- Tranexamic Acid For Lower GI HemorrhageDocument8 pagesTranexamic Acid For Lower GI HemorrhagekarinalavianiNo ratings yet
- Arunji Speech J&K ABVP's Response To JNU Victory............Document25 pagesArunji Speech J&K ABVP's Response To JNU Victory............NSadagopanNo ratings yet
- Avoiding Complication Laparoscpy 2014 EnglishDocument102 pagesAvoiding Complication Laparoscpy 2014 EnglishdanludiNo ratings yet
- Antibiotics Surgical ProphylaxisDocument4 pagesAntibiotics Surgical ProphylaxisAshraf AlbhlaNo ratings yet
- Health Professionals - WKTDocument3 pagesHealth Professionals - WKTtimesnewspapersNo ratings yet
- Wound NursingDocument22 pagesWound NursingAgeng Catur WicaksonoNo ratings yet
- Introduction To 270/271: Health Care Eligibility Inquiry/ResponseDocument18 pagesIntroduction To 270/271: Health Care Eligibility Inquiry/ResponseNikhil SatavNo ratings yet
- UntitledDocument18 pagesUntitledMaria Paola RogelNo ratings yet
- Cryopreservation Versus Subcutaneous Preservation of Autologous Bone Flaps For CranioplastyDocument5 pagesCryopreservation Versus Subcutaneous Preservation of Autologous Bone Flaps For CranioplastyNontaphon PiyawattanamethaNo ratings yet
- Opmi Pentero 800 From Zeiss: Never CompromiseDocument14 pagesOpmi Pentero 800 From Zeiss: Never CompromiseLucas RibeiroNo ratings yet
- FECAVA Key Recommendations For Hygiene and Infection Control in Veterinary PracticeDocument1 pageFECAVA Key Recommendations For Hygiene and Infection Control in Veterinary PracticePetrisor GheorghiuNo ratings yet
- The Art and Science of Facelift Surgery A Video Atlas Ebook PDFDocument47 pagesThe Art and Science of Facelift Surgery A Video Atlas Ebook PDFpatrick.charriez697100% (33)
- Talbot DeclDocument5 pagesTalbot DeclCassandra FairbanksNo ratings yet