You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Lion Air - 03 Aug 2014 - YpnoalDocument2 pagesLion Air - 03 Aug 2014 - YpnoalNovita WulandariNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Scabies and Pediculosis Pubis: An Update of Treatment Regimens and General ReviewDocument7 pagesScabies and Pediculosis Pubis: An Update of Treatment Regimens and General ReviewNovita WulandariNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- WindDocument3 pagesWindNovita WulandariNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Scabies and Pediculosis Pubis: An Update of Treatment Regimens and General ReviewDocument7 pagesScabies and Pediculosis Pubis: An Update of Treatment Regimens and General ReviewNovita WulandariNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- NAMA: NIM: : Checklist BLOK 3 Pemeriksaan FisikDocument2 pagesNAMA: NIM: : Checklist BLOK 3 Pemeriksaan FisikNovita WulandariNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Asphyxia Dr. BetaDocument7 pagesAsphyxia Dr. BetaDefri RahmanNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- AlwiDocument2 pagesAlwiNovita WulandariNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Jadwal Defisiensi Public Health S2 IKM FK UGM. ULFAHDocument1 pageJadwal Defisiensi Public Health S2 IKM FK UGM. ULFAHNovita WulandariNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Pain Lecture Nociceptic and NeuropathicDocument56 pagesPain Lecture Nociceptic and NeuropathicNovita WulandariNo ratings yet
- Chapter1 ACG Taxonomy 16Document24 pagesChapter1 ACG Taxonomy 16Novita WulandariNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Chapter1 ACG Taxonomy 16Document24 pagesChapter1 ACG Taxonomy 16Novita WulandariNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Disease Transmission and ContextDocument24 pagesDisease Transmission and ContextSaad MotawéaNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Lecture10animals2 Taxonomy 5Document9 pagesLecture10animals2 Taxonomy 5Novita WulandariNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Hilda TigerDocument2 pagesHilda TigerNovita WulandariNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Persentasi 1n (Print)Document3 pagesPersentasi 1n (Print)Novita Wulandari100% (2)
- Klasifikasi Gangguan JiwaDocument49 pagesKlasifikasi Gangguan JiwaBonaventura Ahardiansyah Bo100% (1)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Unconditional Loa NottinghamDocument1 pageUnconditional Loa NottinghamNovita WulandariNo ratings yet
- MaswanDocument7 pagesMaswanNovita WulandariNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Tuberculosis in Canada: Pre-ReleaseDocument10 pagesTuberculosis in Canada: Pre-ReleaseNovita WulandariNo ratings yet
- Medication Management in People With Parkinson'sDocument5 pagesMedication Management in People With Parkinson'sNovita WulandariNo ratings yet
- McMahon Ch54Document14 pagesMcMahon Ch54SLINo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Gon Update April 2007Document5 pagesGon Update April 2007Novita WulandariNo ratings yet
- 996 FullDocument9 pages996 FullNovita WulandariNo ratings yet
- InijugaDocument30 pagesInijugaNovita WulandariNo ratings yet
- 18 25 1 PBDocument7 pages18 25 1 PBSafira T LNo ratings yet
- Pl2-1 - Zhengping Lu - PublishableDocument33 pagesPl2-1 - Zhengping Lu - PublishableNovita WulandariNo ratings yet
- Cerebral Blood Flow by Arterial Spin Labeling in Poststroke DementiaDocument7 pagesCerebral Blood Flow by Arterial Spin Labeling in Poststroke DementiaNovita WulandariNo ratings yet
- Form Konfirmasi Sponsorship (Hoka Hoka Bento)Document1 pageForm Konfirmasi Sponsorship (Hoka Hoka Bento)Novita WulandariNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Erythema Nodosum: A Sign of Systemic DiseaseDocument6 pagesErythema Nodosum: A Sign of Systemic DiseaseMuhammad ZubaidiNo ratings yet
- Spinal Anaesthesia A Practical GuideDocument14 pagesSpinal Anaesthesia A Practical GuideNovita WulandariNo ratings yet
- 1365 2768 1 PBDocument16 pages1365 2768 1 PBAlief AyuNo ratings yet
- Midwife Essay TopicsDocument1 pageMidwife Essay Topicsmal6640No ratings yet
- Unintended PregnancyDocument10 pagesUnintended PregnancynathanNo ratings yet
- Resume Azadeh RahmatianDocument3 pagesResume Azadeh RahmatianSepideh MirzaeiNo ratings yet
- Ob 11Document4 pagesOb 11Alleya SheeneNo ratings yet
- MidwifeDocument19 pagesMidwifesung hooNo ratings yet
- Trauma and Fear in Australian Midwives - 2019 - Women and BirthDocument8 pagesTrauma and Fear in Australian Midwives - 2019 - Women and BirthlinaNo ratings yet
- Reading Practice-Sentence Structure and Vocab - Abortion A Controversial IssueDocument4 pagesReading Practice-Sentence Structure and Vocab - Abortion A Controversial IssueAgung AdyatmikaNo ratings yet
- Varayti NG Wika 12-47-1-PBDocument26 pagesVarayti NG Wika 12-47-1-PBAlmira Amor MarginNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Jurnal Kasus Etikolegal Dalam Praktik KebidananDocument13 pagesJurnal Kasus Etikolegal Dalam Praktik KebidananErni AnggieNo ratings yet
- ENDORSEMENTDocument6 pagesENDORSEMENTArianna MabungaNo ratings yet
- Teen Talk Vol 3Document2 pagesTeen Talk Vol 3api-309082881No ratings yet
- ESP For MIDWIFERY English For Specific PDocument46 pagesESP For MIDWIFERY English For Specific PMrKanghasanNo ratings yet
- Family Planning MethodDocument7 pagesFamily Planning MethodDebyang B ChangliNo ratings yet
- Normal Birth As A Cultural PhenomenonDocument8 pagesNormal Birth As A Cultural PhenomenonMaria Johanna SchoutenNo ratings yet
- Dengue Hemorrhagic Fever: Dian Rahayu Ningtias 030.14.052 Pembimbing: Dr. Andri Firdaus, Sp.ADocument35 pagesDengue Hemorrhagic Fever: Dian Rahayu Ningtias 030.14.052 Pembimbing: Dr. Andri Firdaus, Sp.Adirani rahmanNo ratings yet
- Phyilosophy of Midwifery Care 2Document13 pagesPhyilosophy of Midwifery Care 2Noella BezzinaNo ratings yet
- Causes of Maternal Mortality and MorbidityDocument20 pagesCauses of Maternal Mortality and MorbidityRaNa MaYaaNo ratings yet
- Abortion in The PhilippinesDocument24 pagesAbortion in The PhilippinesJeff Ray DobluisNo ratings yet
- Midwifery JurisprudenceDocument56 pagesMidwifery JurisprudenceKaren Mae AlcantaraNo ratings yet
- Post Abortal CareDocument14 pagesPost Abortal CareRanyang Akafa100% (1)
- Faktor Penyebab Terjadinya Bendungan Asi Pada Ibu PostpartumDocument8 pagesFaktor Penyebab Terjadinya Bendungan Asi Pada Ibu PostpartumNur Rohmatul AiniNo ratings yet
- PRC Delivery Case 2Document5 pagesPRC Delivery Case 2rosebelleos2024No ratings yet
- 1280 2976 1 SMDocument15 pages1280 2976 1 SMNovita Lina100% (1)
- Lubchanco Classification of Newborns-BoysgirlsDocument1 pageLubchanco Classification of Newborns-BoysgirlsAmanda JulianaNo ratings yet
- Modified Early Obstetric Warning Score MEOWS MID33 AO13 v4.2Document9 pagesModified Early Obstetric Warning Score MEOWS MID33 AO13 v4.2indirinoor5No ratings yet
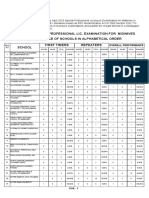
- April 2023 Special Professional Lic. Examination For MidwivesDocument2 pagesApril 2023 Special Professional Lic. Examination For MidwivesRapplerNo ratings yet
- Family Planning (Text)Document2 pagesFamily Planning (Text)Corrinne TayNo ratings yet
- Toc 21 CBT Information BookletDocument12 pagesToc 21 CBT Information BookletJane TriceNo ratings yet
- 5 - Revised - Self-Assessment Tool For Selected MNCHN Indicators - August14,2014Document92 pages5 - Revised - Self-Assessment Tool For Selected MNCHN Indicators - August14,2014Glenn L. RavanillaNo ratings yet
- AP® Chemistry Crash Course, For the 2020 Exam, Book + Online: Get a Higher Score in Less TimeFrom EverandAP® Chemistry Crash Course, For the 2020 Exam, Book + Online: Get a Higher Score in Less TimeRating: 5 out of 5 stars5/5 (1)
- Periodic Tales: A Cultural History of the Elements, from Arsenic to ZincFrom EverandPeriodic Tales: A Cultural History of the Elements, from Arsenic to ZincRating: 3.5 out of 5 stars3.5/5 (137)
- Is That a Fact?: Frauds, Quacks, and the Real Science of Everyday LifeFrom EverandIs That a Fact?: Frauds, Quacks, and the Real Science of Everyday LifeRating: 5 out of 5 stars5/5 (4)
- The Nature of Drugs Vol. 1: History, Pharmacology, and Social ImpactFrom EverandThe Nature of Drugs Vol. 1: History, Pharmacology, and Social ImpactRating: 5 out of 5 stars5/5 (5)
- Handbook of Formulating Dermal Applications: A Definitive Practical GuideFrom EverandHandbook of Formulating Dermal Applications: A Definitive Practical GuideNo ratings yet
- Fundamentals of Chemistry: A Modern IntroductionFrom EverandFundamentals of Chemistry: A Modern IntroductionRating: 5 out of 5 stars5/5 (1)