You might also like
- Support For The Distal Extension Denture Base Altered Cast Technique 1Document39 pagesSupport For The Distal Extension Denture Base Altered Cast Technique 1ahmed.kald896No ratings yet
- A New Design For A Hybrid PDocument16 pagesA New Design For A Hybrid PDavid CLNo ratings yet
- Definitive Obturator Modified For Crown - PPTX DR AmrDocument49 pagesDefinitive Obturator Modified For Crown - PPTX DR AmrHatem Ibrahim Ahmed AburiaNo ratings yet
- Horizontal Augmentation Through The Ridge-Split Procedure: A Predictable Surgical Modality in Implant ReconstructionDocument10 pagesHorizontal Augmentation Through The Ridge-Split Procedure: A Predictable Surgical Modality in Implant ReconstructionWuppuluri Jayanth Kumar SharmaNo ratings yet
- Articulators and Related InstrumentsDocument4 pagesArticulators and Related InstrumentsUmut ASLANNo ratings yet
- Elias On 1983Document3 pagesElias On 1983JesusCordoba100% (2)
- Esthetic Rehabilitation With A Cast Partial Denture: Case ReportDocument4 pagesEsthetic Rehabilitation With A Cast Partial Denture: Case ReportMissyNo ratings yet
- RPH Clasp Assembly - A Simple Alternative To Traditional DesignsDocument3 pagesRPH Clasp Assembly - A Simple Alternative To Traditional DesignsFaheemuddin Muhammad0% (1)
- Ridge Defects and Pontic DesignDocument14 pagesRidge Defects and Pontic DesignFaheemuddin MuhammadNo ratings yet
- The Mandibular First Premolar As An Abutment For Distal-Extension Removable Partial Dentures: A Modified Clasp Assembly DesignDocument3 pagesThe Mandibular First Premolar As An Abutment For Distal-Extension Removable Partial Dentures: A Modified Clasp Assembly DesignDentist HereNo ratings yet
- Introduction of Removable Partial Denture - Design and RetentionDocument72 pagesIntroduction of Removable Partial Denture - Design and RetentionDilesh Pradhan0% (1)
- Chapter 4 Final Impression FinalDocument19 pagesChapter 4 Final Impression FinalMohammed AsfourNo ratings yet
- A Review of The Surgical Protocol For Reconstruction of Alveolar Ridge DeficiencyDocument21 pagesA Review of The Surgical Protocol For Reconstruction of Alveolar Ridge DeficiencyAymen Elatrash100% (1)
- Diagnostic Procedures and Articulation Occlusion 2021-2022Document43 pagesDiagnostic Procedures and Articulation Occlusion 2021-2022محمد ربيعيNo ratings yet
- Designing Removable Partial Dentures for Optimal FunctionDocument32 pagesDesigning Removable Partial Dentures for Optimal FunctionAbdelrhman AdelNo ratings yet
- Epi IDocument4 pagesEpi IAna-Maria MachidonNo ratings yet
- Modified Pontic Design For Ridge DefectsDocument11 pagesModified Pontic Design For Ridge DefectsFaheemuddin MuhammadNo ratings yet
- Lec 8 3rd Class PDFDocument4 pagesLec 8 3rd Class PDFBrandon AviciiNo ratings yet
- First Impressions Count: RestorativeDocument12 pagesFirst Impressions Count: RestorativeMasitah GraceNo ratings yet
- A New Concept in Maintaining The Emergence ProfileDocument8 pagesA New Concept in Maintaining The Emergence ProfileankitaNo ratings yet
- Ovate PDFDocument11 pagesOvate PDFAriPratiwiNo ratings yet
- BDJ Volume 201 Issue 6 2006 (Doi 10.1038/sj - bdj.4814041) Chee, W Jivraj, S - Treatment Planning of The Edentulous MandibleDocument9 pagesBDJ Volume 201 Issue 6 2006 (Doi 10.1038/sj - bdj.4814041) Chee, W Jivraj, S - Treatment Planning of The Edentulous MandibleahmadNo ratings yet
- RPD Test With KeyDocument14 pagesRPD Test With KeySaleh Al-naimiNo ratings yet
- Basic Principles of Clasp DesignDocument124 pagesBasic Principles of Clasp Designbharathi krishnaNo ratings yet
- Prepearing Teeth For RPDDocument14 pagesPrepearing Teeth For RPDShreyans DamadeNo ratings yet
- Dental ImplantDocument34 pagesDental Implantjuren.zafat.05No ratings yet
- RPD ReviewDocument212 pagesRPD ReviewAlnielJoManlapig100% (3)
- Ten Facts About Dental Implants: September-October 2016 - No. 5, Vol. 6 P D WWW - Dental-Tribune - MeDocument4 pagesTen Facts About Dental Implants: September-October 2016 - No. 5, Vol. 6 P D WWW - Dental-Tribune - Mefreddybot89No ratings yet
- 1 s2.0 S0278239196903651 MainDocument3 pages1 s2.0 S0278239196903651 MaindrescobedocomfNo ratings yet
- 6.rpa Clasp DesignDocument3 pages6.rpa Clasp DesignbarbieNo ratings yet
- Distal ExtensionDocument110 pagesDistal ExtensionParmod GuliaNo ratings yet
- Chairside Options For The TreatmentDocument6 pagesChairside Options For The TreatmentdiliesdiNo ratings yet
- Initial Placement - DR Hasanain-2023-2024Document10 pagesInitial Placement - DR Hasanain-2023-2024SRO oONo ratings yet
- Tran2009 PDFDocument4 pagesTran2009 PDFDaniel SisniegasNo ratings yet
- 4 Relining TechniquesDocument9 pages4 Relining TechniquesvinnycoolbuddyNo ratings yet
- Chapter 101. Primary Hip Arthroplasty - I. Total Hip ArthroplastyDocument65 pagesChapter 101. Primary Hip Arthroplasty - I. Total Hip ArthroplastyVanessa Yvonne GurtizaNo ratings yet
- RPI and RPA ConceptDocument62 pagesRPI and RPA ConceptAnshuman Chaturvedi75% (4)
- Benefits of RPD: Elements and Compromised Function. The Removal of Exostoses and Tori Is Not A Complex ProcedureDocument8 pagesBenefits of RPD: Elements and Compromised Function. The Removal of Exostoses and Tori Is Not A Complex ProcedureSonia LeeNo ratings yet
- Using Intraoral Gothic Arch Tracing To Balance Full Dentures and Determine Centric Relation and Occlusal Vertical DimensionDocument15 pagesUsing Intraoral Gothic Arch Tracing To Balance Full Dentures and Determine Centric Relation and Occlusal Vertical DimensionAlfred OrozcoNo ratings yet
- Rotational Path Removable Partial Denture DesignDocument7 pagesRotational Path Removable Partial Denture DesignNapatsorn RakpakwanNo ratings yet
- Awais AssignmentDocument3 pagesAwais AssignmentMuhammad AwaisNo ratings yet
- Densit Osoasa A Palatului DurDocument8 pagesDensit Osoasa A Palatului DurDiana DrutaNo ratings yet
- Prosthetic Rehabilitation of Maxillectomy Patient With Telescopic DenturesDocument6 pagesProsthetic Rehabilitation of Maxillectomy Patient With Telescopic DenturesVero AngelNo ratings yet
- Indications and Contraindications For Rpa &rpi (Group 3)Document10 pagesIndications and Contraindications For Rpa &rpi (Group 3)sidney changiNo ratings yet
- Distal ExtentionDocument33 pagesDistal ExtentionMohammed HassanNo ratings yet
- Prosthetic Management of Implants Placed With The Socket-Shield TechniqueDocument5 pagesProsthetic Management of Implants Placed With The Socket-Shield TechniqueRiya KvNo ratings yet
- Improving RPD Retention with RPI SystemDocument17 pagesImproving RPD Retention with RPI Systemishtiii100% (2)
- Gingivally Approaching Clasp - PedagogyDocument35 pagesGingivally Approaching Clasp - PedagogyNiaz AhammedNo ratings yet
- Prosthodonticsdd2011-2012 DR GhadeerDocument172 pagesProsthodonticsdd2011-2012 DR GhadeerGhadeerHassaan100% (5)
- Restoring Extensively Destroyed Posterior TeethDocument68 pagesRestoring Extensively Destroyed Posterior TeethHend MohamedNo ratings yet
- Impression Techniques in RPDDocument82 pagesImpression Techniques in RPDpramodaniNo ratings yet
- Fabrication of Conventional Complete Dentures For A Left Segmental MandibulectomyDocument4 pagesFabrication of Conventional Complete Dentures For A Left Segmental MandibulectomyIndrani DasNo ratings yet
- Bowman2018 PDFDocument48 pagesBowman2018 PDFKhyati GuptaNo ratings yet
- 12) Types of Clasp AssembliesDocument16 pages12) Types of Clasp Assembliesطيبة نعمانNo ratings yet
- Endodontic Cavity PreparationDocument166 pagesEndodontic Cavity Preparationagusaranp0% (1)
- Effect of implant support on mandibular distal extension removable partial denturesDocument4 pagesEffect of implant support on mandibular distal extension removable partial denturesNovita RNo ratings yet
- Assignment: 1-What Is The Rationale Behind The Mesial Rest Concept in Distal Extension Removable Partial Denture Cases ?Document7 pagesAssignment: 1-What Is The Rationale Behind The Mesial Rest Concept in Distal Extension Removable Partial Denture Cases ?احمد القحطانيNo ratings yet
- 2018 Admixed TechDocument3 pages2018 Admixed TechBrijesh MaskeyNo ratings yet
- Deswsdfdfgf DGDocument9 pagesDeswsdfdfgf DGNaresh TeresNo ratings yet
- God Is GreatDocument1 pageGod Is GreatlalitnidNo ratings yet
- Revised CRPD Sbipo Rectruitment English AdvertisementDocument3 pagesRevised CRPD Sbipo Rectruitment English AdvertisementNaresh TeresNo ratings yet
- DeswDocument10 pagesDeswNaresh TeresNo ratings yet
- DeswDocument10 pagesDeswNaresh TeresNo ratings yet
- DeswDocument9 pagesDeswNaresh TeresNo ratings yet
- Deswsdfdfgf DGDocument9 pagesDeswsdfdfgf DGNaresh TeresNo ratings yet
- PassDocument1 pagePassNaresh TeresNo ratings yet
- PassDocument1 pagePassNaresh TeresNo ratings yet
- FredDocument31 pagesFredNaresh TeresNo ratings yet
- PKIET Recruitment for Teaching PostsDocument8 pagesPKIET Recruitment for Teaching PostsNaresh TeresNo ratings yet
- FredDocument263 pagesFredNaresh TeresNo ratings yet
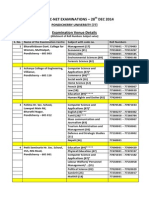
- CBSE-UGC-NET Examination (Dec 2014) - Examination Venue Details (Revised)Document2 pagesCBSE-UGC-NET Examination (Dec 2014) - Examination Venue Details (Revised)Naresh TeresNo ratings yet
- DersfdsfDocument253 pagesDersfdsfNaresh TeresNo ratings yet
- FredDocument125 pagesFredNaresh TeresNo ratings yet
- FredDocument125 pagesFredNaresh TeresNo ratings yet
- FredDocument124 pagesFredNaresh TeresNo ratings yet
- 17Document9 pages17Naresh TeresNo ratings yet
- FredDocument28 pagesFredNaresh TeresNo ratings yet
- ConclusionDocument1 pageConclusionNaresh TeresNo ratings yet
- FredDocument5 pagesFredNaresh TeresNo ratings yet
- FredDocument5 pagesFredNaresh TeresNo ratings yet
- Evaluating Peri-Implant Tissues with Platform SwitchingDocument5 pagesEvaluating Peri-Implant Tissues with Platform SwitchingNaresh TeresNo ratings yet
- WellDocument1 pageWellNaresh TeresNo ratings yet
- DSFSD FDGDFG FHFSHFGDocument8 pagesDSFSD FDGDFG FHFSHFGNaresh TeresNo ratings yet
- GK 2012Document2 pagesGK 2012Krishna GNo ratings yet
- Revised CRPD Sbipo Rectruitment English AdvertisementDocument3 pagesRevised CRPD Sbipo Rectruitment English AdvertisementNaresh TeresNo ratings yet
- N Orthodontic TreatmentDocument4 pagesN Orthodontic TreatmentNaresh TeresNo ratings yet
- Intraoral implants provide retention and supportDocument5 pagesIntraoral implants provide retention and supportNaresh TeresNo ratings yet
- Intraoral implants provide retention and supportDocument5 pagesIntraoral implants provide retention and supportNaresh TeresNo ratings yet
- Pedo MCQs QuestionsDocument17 pagesPedo MCQs QuestionsYazan Emad Salem90% (30)
- Lip RepositioningDocument5 pagesLip RepositioningNurul Novita SuhartonoNo ratings yet
- Extra Oral ExaminationDocument22 pagesExtra Oral ExaminationFitri AfrianitaNo ratings yet
- DR Narendra Basutkar M.D.S (Prosthodontics)Document42 pagesDR Narendra Basutkar M.D.S (Prosthodontics)Rohan GroverNo ratings yet
- Peoples' Dental College and HospitalDocument28 pagesPeoples' Dental College and HospitalNiraaz DhyakoNo ratings yet
- Using Modified Polyetheretherketone (PEEK) As An Alternative Material For Endocrown Restorations - A Short-Term Clinical ReportDocument5 pagesUsing Modified Polyetheretherketone (PEEK) As An Alternative Material For Endocrown Restorations - A Short-Term Clinical Reportdody rahman100% (1)
- Articulo AdulteroDocument17 pagesArticulo AdulteroEddy RodriguezNo ratings yet
- Post MortemDocument4 pagesPost MortemErlinda YulyNo ratings yet
- 3.management and Restauration of Badly Broken Down Tetth 2017-2018Document96 pages3.management and Restauration of Badly Broken Down Tetth 2017-2018Hend AlghamdiNo ratings yet
- Biomech of Head Gear-Ortho / Orthodontic Courses by Indian Dental AcademyDocument57 pagesBiomech of Head Gear-Ortho / Orthodontic Courses by Indian Dental Academyindian dental academy100% (2)
- Bushing Method 1Document11 pagesBushing Method 1khalisha salsabilaNo ratings yet
- Epidemiology of Oral Diseases and CancerDocument38 pagesEpidemiology of Oral Diseases and CancerZainab MohammadNo ratings yet
- The Effect of Polishing Techniques On The Surface Roughness of A Feldspathic PorcelainDocument3 pagesThe Effect of Polishing Techniques On The Surface Roughness of A Feldspathic PorcelainffazlaliNo ratings yet
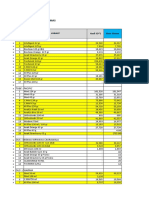
- Bahan Kemas - Selisih SO Vs Sistem FY2020 - 291220Document17 pagesBahan Kemas - Selisih SO Vs Sistem FY2020 - 291220Idan RidwanNo ratings yet
- Serial ExtractionDocument9 pagesSerial ExtractionFarheen MahmoodaNo ratings yet
- Fixed ProsthodonticsDocument16 pagesFixed ProsthodonticsMagnet ShotNo ratings yet
- Sex DeterminationDocument14 pagesSex DeterminationHemant ChourhaNo ratings yet
- Smile Esthetics: Smile Arc Protection Vs Traditional ApproachDocument11 pagesSmile Esthetics: Smile Arc Protection Vs Traditional ApproachPublicidad Digital CanariaNo ratings yet
- Cosmetic Dentistry Two Stage ESthetic Crown Lengthening Sonick Rothenberg and Hwang 2Document52 pagesCosmetic Dentistry Two Stage ESthetic Crown Lengthening Sonick Rothenberg and Hwang 2Ahsan NaseerNo ratings yet
- AAE Position Statement On Vital Pulp Therapy 2021Document10 pagesAAE Position Statement On Vital Pulp Therapy 2021Abhishek Isaac Mathew100% (1)
- DPP Dental Terms PDFDocument15 pagesDPP Dental Terms PDFana dizonNo ratings yet
- Maxillary Expansion in The Mixed Dentition: Rapid or Semi-Rapid?Document8 pagesMaxillary Expansion in The Mixed Dentition: Rapid or Semi-Rapid?Shriya MurarkaNo ratings yet
- Surgical Orthodontic Cephalometric Prediction TracingDocument8 pagesSurgical Orthodontic Cephalometric Prediction TracingMariyamNo ratings yet
- Download Atlas Of Oral Histology 2Nd Edition Harikrishnan Prasad full chapterDocument67 pagesDownload Atlas Of Oral Histology 2Nd Edition Harikrishnan Prasad full chaptervicki.jackson553100% (5)
- Fitting and Checking Retainers: First F Itting of Removable RetainersDocument4 pagesFitting and Checking Retainers: First F Itting of Removable Retainerspuspita witriaNo ratings yet
- Development of OcclusionDocument49 pagesDevelopment of OcclusionSardarni Ramandeep KaurNo ratings yet
- Endo Morphology Chart PDFDocument1 pageEndo Morphology Chart PDFNaji Z. ArandiNo ratings yet
- Oral Hygiene Index (OHIDocument4 pagesOral Hygiene Index (OHIKurnia Indah PuspitasariNo ratings yet
- Pengantar Anatomi Gigi, Teriminologi, & NomenklaturDocument19 pagesPengantar Anatomi Gigi, Teriminologi, & NomenklaturniputusellyowNo ratings yet
- Stages in Orthodontic TreatmentDocument32 pagesStages in Orthodontic TreatmentDavid FernandezNo ratings yet
- Stable Relation: A Memoir of One Woman's Spirited Journey Home, by Way of the BarnFrom EverandStable Relation: A Memoir of One Woman's Spirited Journey Home, by Way of the BarnRating: 5 out of 5 stars5/5 (4)
- The Equine Listenology Guide - Essential Horsemanship, Horse Body Language & Behaviour, Groundwork, In-hand Exercises & Riding Lessons to Develop Softness, Connection & Collection.From EverandThe Equine Listenology Guide - Essential Horsemanship, Horse Body Language & Behaviour, Groundwork, In-hand Exercises & Riding Lessons to Develop Softness, Connection & Collection.Rating: 5 out of 5 stars5/5 (1)
- Horse Training 101: Key Techniques for Every Horse OwnerFrom EverandHorse Training 101: Key Techniques for Every Horse OwnerRating: 4.5 out of 5 stars4.5/5 (27)
- Groundwork with horses: Natural Horsemanship & Groundwork Training for Your HorseFrom EverandGroundwork with horses: Natural Horsemanship & Groundwork Training for Your HorseNo ratings yet
- Horses: 101 Super Fun Facts and Amazing Pictures (Featuring The World's Top 18 Horse Breeds)From EverandHorses: 101 Super Fun Facts and Amazing Pictures (Featuring The World's Top 18 Horse Breeds)Rating: 3.5 out of 5 stars3.5/5 (11)
- Dressage Training and Competition Exercises for Beginners: Flatwork & Collection Schooling for HorsesFrom EverandDressage Training and Competition Exercises for Beginners: Flatwork & Collection Schooling for HorsesNo ratings yet
- There's More to Training Horses: 100 Tips, 100 Days, 100% BetterFrom EverandThere's More to Training Horses: 100 Tips, 100 Days, 100% BetterNo ratings yet
- The Tao of Equus: A Woman's Journey of Healing and Transformation through the Way of the HorseFrom EverandThe Tao of Equus: A Woman's Journey of Healing and Transformation through the Way of the HorseRating: 4.5 out of 5 stars4.5/5 (3)
- The Everything Horse Book: Buying, riding, and caring for your equine companionFrom EverandThe Everything Horse Book: Buying, riding, and caring for your equine companionRating: 2 out of 5 stars2/5 (1)
- From Stride to Ride; Basic Fundamentals for Beginner Horse TrainersFrom EverandFrom Stride to Ride; Basic Fundamentals for Beginner Horse TrainersNo ratings yet
- Fitness Evaluation of the HorseFrom EverandFitness Evaluation of the HorseRating: 5 out of 5 stars5/5 (1)
- Cavaletti: Cavaletti horse training and groundwork with horsesFrom EverandCavaletti: Cavaletti horse training and groundwork with horsesNo ratings yet
- Horse training simply explained: Basic Horse training, Foal training, Natural Horsemanship and much moreFrom EverandHorse training simply explained: Basic Horse training, Foal training, Natural Horsemanship and much moreNo ratings yet
- Hoof Physics: How to Recognize the Signs of Hoof DistortionFrom EverandHoof Physics: How to Recognize the Signs of Hoof DistortionRating: 5 out of 5 stars5/5 (1)
- Horse treats Do-It-Yourself - Cookbook for horses: Cookbook for horses - Make your own horse treatsFrom EverandHorse treats Do-It-Yourself - Cookbook for horses: Cookbook for horses - Make your own horse treatsNo ratings yet
- Straight from the Horse's Mouth: How to Talk to Animals and Get AnswersFrom EverandStraight from the Horse's Mouth: How to Talk to Animals and Get AnswersNo ratings yet
- Joey: How a Blind Rescue Horse Helped Others Learn to SeeFrom EverandJoey: How a Blind Rescue Horse Helped Others Learn to SeeRating: 5 out of 5 stars5/5 (12)