You might also like
- Pediatrics in Review 2014 Piedimonte 519 30Document15 pagesPediatrics in Review 2014 Piedimonte 519 30Felipe CeaNo ratings yet
- Sepsis Management of Neonates With Suspected or Proven Early-Onset BacterialDocument12 pagesSepsis Management of Neonates With Suspected or Proven Early-Onset BacterialAldo CancellaraNo ratings yet
- Inotropicos en Neonatos 2Document13 pagesInotropicos en Neonatos 2Paola DiazNo ratings yet
- Sepsis Neonatal 2012 PeiatricsDocument12 pagesSepsis Neonatal 2012 PeiatricsWalter LojaNo ratings yet
- 2018 UNICEF Eswatini Neonatal GuidelinesDocument180 pages2018 UNICEF Eswatini Neonatal GuidelinesTrishenth FonsekaNo ratings yet
- Neonatal Sepsis 2019.Document6 pagesNeonatal Sepsis 2019.Jean Paúl LópezNo ratings yet
- Sepsis Neonatal: Bryan L Ohning, MD, PHD, Clinical Associate Professor of Pediatrics, MedicalDocument43 pagesSepsis Neonatal: Bryan L Ohning, MD, PHD, Clinical Associate Professor of Pediatrics, Medicalapi-19492580No ratings yet
- Neonatal MnemonicDocument3 pagesNeonatal MnemonicA.h.MuradNo ratings yet
- Common Dysmorphic Syndromes in The NICUDocument12 pagesCommon Dysmorphic Syndromes in The NICUDaniel PuertasNo ratings yet
- Keyes Neonatal Emergencies FinalDocument108 pagesKeyes Neonatal Emergencies FinalthanyunNo ratings yet
- Theraputic Agent in NeonateDocument7 pagesTheraputic Agent in Neonateد. محمد فريد الغنامNo ratings yet
- Guideline For Acute Care of Neonates 2014 PDFDocument176 pagesGuideline For Acute Care of Neonates 2014 PDFNaruto_Uchiha777No ratings yet
- Recent Developments in The Management of Neonatal HyperbilirubinemiaDocument8 pagesRecent Developments in The Management of Neonatal HyperbilirubinemiaMyrtle SetiawanNo ratings yet
- Gomella - SepsisDocument15 pagesGomella - SepsisJustine Frances CabalayNo ratings yet
- Paracetamol Dosing and Metabolism in NeonatesDocument7 pagesParacetamol Dosing and Metabolism in Neonatesnurul sya'binNo ratings yet
- Neonatal SepsisDocument12 pagesNeonatal Sepsissandra bullaNo ratings yet
- Antibiotic Use in Critical Care: DR Radha Sundaram Lead Clinician RAH PaisleyDocument36 pagesAntibiotic Use in Critical Care: DR Radha Sundaram Lead Clinician RAH PaisleyHidayati IdaNo ratings yet
- OSCE Checklist Newborn Baby Assessment NIPEDocument3 pagesOSCE Checklist Newborn Baby Assessment NIPETauqeer Ahmed0% (1)
- Infection in NeonateDocument28 pagesInfection in Neonateamel015No ratings yet
- Abstracts From The 6th International Conference On Prevention & Infection Control (ICPIC 2021)Document140 pagesAbstracts From The 6th International Conference On Prevention & Infection Control (ICPIC 2021)Karen RodriguezNo ratings yet
- Algorithm For Anemia in Children Based On MCV - UpToDateDocument2 pagesAlgorithm For Anemia in Children Based On MCV - UpToDatefabsscribdworksNo ratings yet
- Early-Onset Sepsis :clinical and Laboratory ChallengeDocument34 pagesEarly-Onset Sepsis :clinical and Laboratory ChallengelordofthewebNo ratings yet
- Adjunctive Therapies in Bronchopulmonary Dysplasia, NeoReview 2017Document9 pagesAdjunctive Therapies in Bronchopulmonary Dysplasia, NeoReview 2017Edrei Lopez CNo ratings yet
- Case Study #1: History and Exam of a Critically Ill NewbornDocument39 pagesCase Study #1: History and Exam of a Critically Ill Newbornleonzon_ben442296No ratings yet
- Pediatrics in Review-2013-Sahai-216-27Document14 pagesPediatrics in Review-2013-Sahai-216-27Facu GuerreroNo ratings yet
- Bronquiolite Guidelines AAPDocument32 pagesBronquiolite Guidelines AAPDiego Guedes da SilvaNo ratings yet
- Aap-Bordetella Pertussis (Pertussis)Document13 pagesAap-Bordetella Pertussis (Pertussis)Ana BlueNo ratings yet
- Parenteral Nutrition in NICUDocument13 pagesParenteral Nutrition in NICUshindy107100% (1)
- AAO READING ON RETINOPATHY OF PREMATURITYDocument34 pagesAAO READING ON RETINOPATHY OF PREMATURITYUNHAS OphthalmologyNo ratings yet
- Starship Children's ECG GuideDocument7 pagesStarship Children's ECG GuideCivodarbo RimidubNo ratings yet
- Antimicrobial Therapy and Late Onset SepsisDocument10 pagesAntimicrobial Therapy and Late Onset SepsisKendy LópezNo ratings yet
- InTech-Neonatal Pneumonia PDFDocument14 pagesInTech-Neonatal Pneumonia PDFClaudia PalominoNo ratings yet
- Infections of The Fetus and NewbornDocument55 pagesInfections of The Fetus and Newbornlordoftheweb100% (4)
- Neonatal HypoglycemiaDocument12 pagesNeonatal HypoglycemiayogaNo ratings yet
- Neonatal JaundiceDocument72 pagesNeonatal JaundiceThya HakimNo ratings yet
- Fever in The Pediatric Patient PDFDocument24 pagesFever in The Pediatric Patient PDFSABASA1012No ratings yet
- Inflammatory: Bowel DiseaseDocument14 pagesInflammatory: Bowel Diseaseusmani_nida1No ratings yet
- 05 Polycythemia in The NewbornDocument11 pages05 Polycythemia in The NewbornMorales Eli PediatraNo ratings yet
- DR Bragg - Endocarditis - Pediatric in Review April 2014Document9 pagesDR Bragg - Endocarditis - Pediatric in Review April 2014angelicaNo ratings yet
- Optimizing Antibiotic Use in the Neonatal UnitDocument41 pagesOptimizing Antibiotic Use in the Neonatal UnityusahanaNo ratings yet
- Pediatric Cervical LymphadenopathyDocument13 pagesPediatric Cervical LymphadenopathyShaira Aquino VerzosaNo ratings yet
- Neonatal Sepsis: A Study of The Risk FactorsDocument42 pagesNeonatal Sepsis: A Study of The Risk FactorsNithin100% (3)
- NRP ppt1Document29 pagesNRP ppt1sumana BanerjeeNo ratings yet
- PIR Nov 2014vol 35 No 11Document66 pagesPIR Nov 2014vol 35 No 11kary_42035865No ratings yet
- Practical Management of AsthmaDocument13 pagesPractical Management of AsthmaAmi LuNo ratings yet
- Necrotizing Enterocolitis - 2019Document10 pagesNecrotizing Enterocolitis - 2019Mischief ManagerNo ratings yet
- Kırşehir Ahi Evran Üniversitesi Sağlık Bilimleri Enstitüsü: Neonatal Sepsis & MeningitisDocument40 pagesKırşehir Ahi Evran Üniversitesi Sağlık Bilimleri Enstitüsü: Neonatal Sepsis & MeningitisAli FalihNo ratings yet
- Evaluation and Treatment of Nonmonosymptomatic EnuresisDocument11 pagesEvaluation and Treatment of Nonmonosymptomatic EnuresisastrogliaNo ratings yet
- Clinical Approach To Respiratory Distress in NewbornDocument29 pagesClinical Approach To Respiratory Distress in Newbornabhivnair100% (1)
- Pediatrics in Review 2013 Adam 368 70Document5 pagesPediatrics in Review 2013 Adam 368 70Cynthia TanuwijoyoNo ratings yet
- Use of C-Reactive Protein and Ferritin Biomarkers in Daily Pediatric PracticeDocument14 pagesUse of C-Reactive Protein and Ferritin Biomarkers in Daily Pediatric PracticeMichelleHanNo ratings yet
- Complete IssueDocument62 pagesComplete IssueAzaliRiccoNo ratings yet
- 9, Procedure of PICCDocument9 pages9, Procedure of PICCputriseptinaNo ratings yet
- NNF Guidelines 2011Document344 pagesNNF Guidelines 2011Vijay Dihora0% (1)
- Neonatal Jaundice ManagementDocument39 pagesNeonatal Jaundice ManagementAfdelina RizkyNo ratings yet
- Pediatric Emergencies 2015Document90 pagesPediatric Emergencies 2015tatiana feliciaNo ratings yet
- NR March2014Document44 pagesNR March2014Susana Jacqueline Echeverria Muñoz100% (1)
- Nursing the NeonateFrom EverandNursing the NeonateMaggie MeeksNo ratings yet
- Abdominal TB Causing Intestinal ObstructionDocument10 pagesAbdominal TB Causing Intestinal ObstructionCleoanne GallegosNo ratings yet
- The Nurse and The Mental Patient A Study in Interpersonal RelationshipDocument300 pagesThe Nurse and The Mental Patient A Study in Interpersonal RelationshipCleoanne GallegosNo ratings yet
- Neonates PDFDocument26 pagesNeonates PDFCleoanne GallegosNo ratings yet
- Child - AsthmaDocument2 pagesChild - AsthmaCleoanne Gallegos0% (1)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- AsthmaDocument8 pagesAsthmaCleoanne GallegosNo ratings yet
- Crit Care Nurse-2011 Overview of MV ModesDocument17 pagesCrit Care Nurse-2011 Overview of MV ModesCleoanne GallegosNo ratings yet
- Clinical Pediatrics: Postdischarge Feeding Patterns in Early-And Late-Preterm InfantsDocument7 pagesClinical Pediatrics: Postdischarge Feeding Patterns in Early-And Late-Preterm InfantsCleoanne GallegosNo ratings yet
- CKDDocument15 pagesCKDMarielle Cattis SiadorNo ratings yet
- NICUDocument11 pagesNICUCleoanne GallegosNo ratings yet
- Clinical Nursing Research: Noise Intervention Minimizing Preterm Infants' Exposure To NICU Light andDocument23 pagesClinical Nursing Research: Noise Intervention Minimizing Preterm Infants' Exposure To NICU Light andCleoanne GallegosNo ratings yet
- PH MaternalDocument10 pagesPH MaternalCleoanne GallegosNo ratings yet
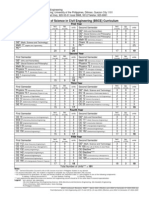
- Bsce CurriculumDocument1 pageBsce CurriculumCleoanne GallegosNo ratings yet
- De So 2 de Kiem Tra Giua Ki 2 Tieng Anh 8 Moi 1677641450Document4 pagesDe So 2 de Kiem Tra Giua Ki 2 Tieng Anh 8 Moi 1677641450phuong phamthihongNo ratings yet
- FCE Listening Test 1-5Document20 pagesFCE Listening Test 1-5Nguyễn Tâm Như Ý100% (2)
- Toolkit:ALLCLEAR - SKYbrary Aviation SafetyDocument3 pagesToolkit:ALLCLEAR - SKYbrary Aviation Safetybhartisingh0812No ratings yet
- Inline check sieve removes foreign matterDocument2 pagesInline check sieve removes foreign matterGreere Oana-NicoletaNo ratings yet
- ms3 Seq 01 Expressing Interests With Adverbs of FrequencyDocument3 pagesms3 Seq 01 Expressing Interests With Adverbs of Frequencyg27rimaNo ratings yet
- Detailed Lesson PlanDocument5 pagesDetailed Lesson PlanHazel Mae HerreraNo ratings yet
- Neligence: Allows Standards of Acceptable Behavior To Be Set For SocietyDocument3 pagesNeligence: Allows Standards of Acceptable Behavior To Be Set For SocietyransomNo ratings yet
- Aladdin and the magical lampDocument4 pagesAladdin and the magical lampMargie Roselle Opay0% (1)
- College Wise Form Fillup Approved Status 2019Document4 pagesCollege Wise Form Fillup Approved Status 2019Dinesh PradhanNo ratings yet
- Sangam ReportDocument37 pagesSangam ReportSagar ShriNo ratings yet
- Tata Hexa (2017-2019) Mileage (14 KML) - Hexa (2017-2019) Diesel Mileage - CarWaleDocument1 pageTata Hexa (2017-2019) Mileage (14 KML) - Hexa (2017-2019) Diesel Mileage - CarWaleMahajan VickyNo ratings yet
- Tennessee Inmate Search Department of Corrections LookupDocument9 pagesTennessee Inmate Search Department of Corrections Lookupinmatesearchinfo50% (2)
- National Family Welfare ProgramDocument24 pagesNational Family Welfare Programminnu100% (1)
- My PDSDocument16 pagesMy PDSRosielyn Fano CatubigNo ratings yet
- R19 MPMC Lab Manual SVEC-Revanth-III-IIDocument135 pagesR19 MPMC Lab Manual SVEC-Revanth-III-IIDarshan BysaniNo ratings yet
- Step-By-Step Guide To Essay WritingDocument14 pagesStep-By-Step Guide To Essay WritingKelpie Alejandria De OzNo ratings yet
- Consumer Behavior Paper PLDTDocument6 pagesConsumer Behavior Paper PLDTAngeline Santiago100% (2)
- Equity Inv HW 2 BHDocument3 pagesEquity Inv HW 2 BHBen HolthusNo ratings yet
- List of Parts For Diy Dremel CNC by Nikodem Bartnik: Part Name Quantity BanggoodDocument6 pagesList of Parts For Diy Dremel CNC by Nikodem Bartnik: Part Name Quantity Banggoodyogesh parmarNo ratings yet
- Mayflower Compact - WikipediaDocument4 pagesMayflower Compact - WikipediaHeaven2012No ratings yet
- Toxicology: General Aspects, Types, Routes of Exposure & AnalysisDocument76 pagesToxicology: General Aspects, Types, Routes of Exposure & AnalysisAsma SikanderNo ratings yet
- Javascript The Web Warrior Series 6Th Edition Vodnik Test Bank Full Chapter PDFDocument31 pagesJavascript The Web Warrior Series 6Th Edition Vodnik Test Bank Full Chapter PDFtina.bobbitt231100% (10)
- Improve Your Social Skills With Soft And Hard TechniquesDocument26 pagesImprove Your Social Skills With Soft And Hard TechniquesEarlkenneth NavarroNo ratings yet
- RA 4196 University Charter of PLMDocument4 pagesRA 4196 University Charter of PLMJoan PabloNo ratings yet
- Corporate Law Scope and RegulationDocument21 pagesCorporate Law Scope and RegulationBasit KhanNo ratings yet
- Sri Lanka Wildlife and Cultural TourDocument9 pagesSri Lanka Wildlife and Cultural TourRosa PaglioneNo ratings yet
- Arx Occasional Papers - Hospitaller Gunpowder MagazinesDocument76 pagesArx Occasional Papers - Hospitaller Gunpowder MagazinesJohn Spiteri GingellNo ratings yet
- Ethiopian Civil Service University UmmpDocument76 pagesEthiopian Civil Service University UmmpsemabayNo ratings yet
- 740LIDocument13 pages740LIm FaisalNo ratings yet
- Science 10-2nd Periodical Test 2018-19Document2 pagesScience 10-2nd Periodical Test 2018-19Emiliano Dela Cruz100% (3)