You might also like
- Knowledge, Attitudes, and Perceptions of Preeclampsia Among First-Generation Nigerian Women in the United StatesFrom EverandKnowledge, Attitudes, and Perceptions of Preeclampsia Among First-Generation Nigerian Women in the United StatesNo ratings yet
- Morning Sickness Treatments: Review Shows Little EvidenceDocument8 pagesMorning Sickness Treatments: Review Shows Little EvidencePutri 'peoe' Nur AnnissaNo ratings yet
- Risk Factors For Repeat Elective Abortion: General GynecologyDocument6 pagesRisk Factors For Repeat Elective Abortion: General GynecologySan Maria SitompulNo ratings yet
- Content ServerDocument7 pagesContent ServerNi Wayan Ana PsNo ratings yet
- Reproductive Coercion and Co-Occurring Intimate Partner Violence in Obstetrics and Gynecology PatientsDocument8 pagesReproductive Coercion and Co-Occurring Intimate Partner Violence in Obstetrics and Gynecology PatientsAna AdamNo ratings yet
- 06 Chapter 2Document48 pages06 Chapter 2Prakash BalagurunathanNo ratings yet
- Perception ChildbearingDocument18 pagesPerception ChildbearingnorjumawatonshahruddNo ratings yet
- Estimating The Period Prevalence of Mothers Who Have Abortions: A Population Based Study of Inclusive Pregnancy OutcomesDocument7 pagesEstimating The Period Prevalence of Mothers Who Have Abortions: A Population Based Study of Inclusive Pregnancy OutcomesGiulianaNo ratings yet
- Psychosocial AdjustmentDocument7 pagesPsychosocial AdjustmentMirjana14No ratings yet
- Katherine J Gold Sheila M Marcus: Table 1Document4 pagesKatherine J Gold Sheila M Marcus: Table 1angelie21No ratings yet
- Family History As A Risk Factor For Pelvic Organ Prolapse: Original ArticleDocument7 pagesFamily History As A Risk Factor For Pelvic Organ Prolapse: Original ArticlepakemainmainNo ratings yet
- Javon WitherspoonDocument6 pagesJavon Witherspoonapi-445367279No ratings yet
- Miscarriage in India: A Population-Based Study: Tervals, Because It Was Not Possible From The Data Set ToDocument3 pagesMiscarriage in India: A Population-Based Study: Tervals, Because It Was Not Possible From The Data Set ToMutianaUmminyaKhanzaNo ratings yet
- Factors Associated With Resilience or Vulnerability To Hot Flushes and Night Sweats During The Menopausal TransitionDocument28 pagesFactors Associated With Resilience or Vulnerability To Hot Flushes and Night Sweats During The Menopausal TransitionKhoiro QonitaNo ratings yet
- English Progress Program: Nama: Nurul Hidayah NIM: 21117091Document12 pagesEnglish Progress Program: Nama: Nurul Hidayah NIM: 21117091nurul4hidayah-99No ratings yet
- Side Effects, Physical Health Consequences, and MortalityDocument5 pagesSide Effects, Physical Health Consequences, and MortalityGunja TandonNo ratings yet
- Mental HealthDocument7 pagesMental HealthMirjana14No ratings yet
- Depression Among Infertile Women in Gaza Strip PreDocument16 pagesDepression Among Infertile Women in Gaza Strip Pregamal attamNo ratings yet
- Psychological: Antecedents To Conception Among Abortion SeekersDocument8 pagesPsychological: Antecedents To Conception Among Abortion SeekersPoreh FarahiyahNo ratings yet
- Debate GUIDE PDFDocument8 pagesDebate GUIDE PDFBlesse PateñoNo ratings yet
- DP 203Document63 pagesDP 203charu parasherNo ratings yet
- Risk Factors For Eclampsia: A Population-Based Study in Washington State, 1987-2007Document7 pagesRisk Factors For Eclampsia: A Population-Based Study in Washington State, 1987-2007Syerra Saindari PutriNo ratings yet
- Psychosocial Factors and Obstetric Complications: B.ChalmersDocument7 pagesPsychosocial Factors and Obstetric Complications: B.ChalmersRafael BagusNo ratings yet
- BJOG - 2005 - Bartellas - Sexuality and Sexual Activity in PregnancyDocument5 pagesBJOG - 2005 - Bartellas - Sexuality and Sexual Activity in Pregnancyศุภชัย ศิลาวัชรพลNo ratings yet
- Womens Health Research Paper TopicsDocument5 pagesWomens Health Research Paper Topicsaflbrozzi100% (1)
- Parturition Events and Risk of Urinary Incontinence in Later LifeDocument16 pagesParturition Events and Risk of Urinary Incontinence in Later LifeMutia LailaniNo ratings yet
- Version of Record:: ManuscriptDocument36 pagesVersion of Record:: ManuscriptskyrollwnNo ratings yet
- Am. J. Epidemiol.-2001-Gold-865-74Document10 pagesAm. J. Epidemiol.-2001-Gold-865-74Nouchan NoupNo ratings yet
- Risk Factors For Uterine Fibroids Among Women Undergoing Tubal SterilizationDocument8 pagesRisk Factors For Uterine Fibroids Among Women Undergoing Tubal SterilizationWahyu Tri KusprasetyoNo ratings yet
- ABORTIONrevDocument18 pagesABORTIONrevAdrian Rey Cuartero DolorielNo ratings yet
- Psikologi N Emotional InfertilityDocument7 pagesPsikologi N Emotional InfertilityjawaralopangNo ratings yet
- McDonald Et Al-2015-BJOG - An International Journal of Obstetrics & GynaecologyDocument8 pagesMcDonald Et Al-2015-BJOG - An International Journal of Obstetrics & GynaecologyKevin LoboNo ratings yet
- Ellis, Wojnar, & Pettinato, 2015Document8 pagesEllis, Wojnar, & Pettinato, 2015Anonymous 75M6uB3OwNo ratings yet
- Coitus Late in PregnancyDocument8 pagesCoitus Late in PregnancyabdullahNo ratings yet
- Moreau 2016Document11 pagesMoreau 2016heni bayu putriNo ratings yet
- Ekwo 1993Document10 pagesEkwo 1993Nurul ImaniarNo ratings yet
- Abortion and Womens Health - April 2017Document28 pagesAbortion and Womens Health - April 2017Gabriel SantosNo ratings yet
- Waldenstrom 2004Document11 pagesWaldenstrom 2004andrea azevedoNo ratings yet
- Prevalence of Psychiatric Disorders in Infertile Women and Men Undergoing in Vitro Fertilization TreatmentDocument8 pagesPrevalence of Psychiatric Disorders in Infertile Women and Men Undergoing in Vitro Fertilization TreatmentMaria Galia Elias QuirogaNo ratings yet
- Early Prediction of Preterm Birth For Singleton, Twin, and Triplet PregnanciesDocument6 pagesEarly Prediction of Preterm Birth For Singleton, Twin, and Triplet PregnanciesNi Wayan Ana PsNo ratings yet
- A Maternal Vegetarian Diet in Pregnancy Is Associated With HypospadiasDocument7 pagesA Maternal Vegetarian Diet in Pregnancy Is Associated With HypospadiasancoursNo ratings yet
- Female and Male Lifestyle Habits and IVF: What Is Known and UnknownDocument25 pagesFemale and Male Lifestyle Habits and IVF: What Is Known and UnknownAdriana Carolina Morillo RomeroNo ratings yet
- Epidemiology of Dysmenorrhea Among Female Adolescents in CentralDocument7 pagesEpidemiology of Dysmenorrhea Among Female Adolescents in CentralRuth RachmawatyNo ratings yet
- Artikel 2 DheaDocument16 pagesArtikel 2 Dheadayana nopridaNo ratings yet
- Studiu de CazDocument27 pagesStudiu de CazAdina TomsaNo ratings yet
- Risk of Violence From The Man Involved in The Pregnancy After Receiving or Being Denied An AbortionDocument7 pagesRisk of Violence From The Man Involved in The Pregnancy After Receiving or Being Denied An AbortionapeNo ratings yet
- Lactation Induction in A Transgender WomanDocument6 pagesLactation Induction in A Transgender WomanM S de BarrosNo ratings yet
- Poa90046 931 936Document6 pagesPoa90046 931 936mmnahidNo ratings yet
- Author Information Kafaei Atrian MDocument9 pagesAuthor Information Kafaei Atrian MabdullahNo ratings yet
- Annotated Bibliography-4Document10 pagesAnnotated Bibliography-4api-645069403No ratings yet
- BMJ f6398Document13 pagesBMJ f6398Luis Gerardo Pérez CastroNo ratings yet
- The Effect of Abortion On Having and Achieving Aspirational One-Year PlansDocument10 pagesThe Effect of Abortion On Having and Achieving Aspirational One-Year PlansAhlfea JugalbotNo ratings yet
- Psych 401 Idea PaperDocument6 pagesPsych 401 Idea Paperapi-643487977No ratings yet
- Amn Inf2Document9 pagesAmn Inf2Melih CivanNo ratings yet
- Obesity and Diabetes Genetic Variants Associated With Gestational Weight GainDocument17 pagesObesity and Diabetes Genetic Variants Associated With Gestational Weight GainEgie Nugraha Fitriyan ApriyadiNo ratings yet
- EN Epidemiology of Dysmenorrhea Among FemalDocument6 pagesEN Epidemiology of Dysmenorrhea Among FemalRuth RachmawatyNo ratings yet
- Analytical Study of Intrauterine Fetal Death Cases and Associated Maternal ConditionsDocument5 pagesAnalytical Study of Intrauterine Fetal Death Cases and Associated Maternal ConditionsNurvita WidyastutiNo ratings yet
- A Prospective Cohort Study of Pregnancy Risk Factors and Birth Outcomes in Aboriginal WomenDocument5 pagesA Prospective Cohort Study of Pregnancy Risk Factors and Birth Outcomes in Aboriginal WomenFirman DariyansyahNo ratings yet
- Abortion and Mental Health Disorders: Evidence From A 30-Year Longitudinal StudyDocument8 pagesAbortion and Mental Health Disorders: Evidence From A 30-Year Longitudinal StudyuntakegersanganNo ratings yet
- Endo Met RitisDocument9 pagesEndo Met RitisabdullahNo ratings yet
- Sychological Spects of Enopause: H. P. Rosemeier, B. Schultz-ZehdenDocument9 pagesSychological Spects of Enopause: H. P. Rosemeier, B. Schultz-Zehdenchie_8866No ratings yet
- Psychosocial Adjustment Needs of Menopausal Women: Dimkpa, D. IDocument15 pagesPsychosocial Adjustment Needs of Menopausal Women: Dimkpa, D. Ichie_8866No ratings yet
- Anth 13 2 131 11 679 Mushtaq S TTDocument5 pagesAnth 13 2 131 11 679 Mushtaq S TTchie_8866No ratings yet
- Epidemiol Rev 2006 Robinson 81 7Document7 pagesEpidemiol Rev 2006 Robinson 81 7chie_8866No ratings yet
- Prof. Sujata Patel Department of Sociology, University of Hyderabad Anurekha Chari Wagh Department of Sociology, Savitribaiphule Pune UniversityDocument19 pagesProf. Sujata Patel Department of Sociology, University of Hyderabad Anurekha Chari Wagh Department of Sociology, Savitribaiphule Pune UniversityHarish KumarNo ratings yet
- Romeo and Juliet: Unit Test Study GuideDocument8 pagesRomeo and Juliet: Unit Test Study GuideKate Ramey100% (7)
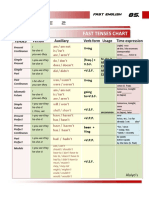
- Table 2: Fast Tenses ChartDocument5 pagesTable 2: Fast Tenses ChartAngel Julian HernandezNo ratings yet
- Travel Services AgreementDocument36 pagesTravel Services AgreementEllijala VarunNo ratings yet
- Urban Transportation System Design and Feasibility Analysis A Case Study of Lagos Mega-CityDocument8 pagesUrban Transportation System Design and Feasibility Analysis A Case Study of Lagos Mega-CityKaren EstradaNo ratings yet
- 1 PDFDocument176 pages1 PDFDigna Bettin CuelloNo ratings yet
- Dr. Nimal SandaratneDocument12 pagesDr. Nimal SandaratneDamith ChandimalNo ratings yet
- First Summative Test in TLE 6Document1 pageFirst Summative Test in TLE 6Georgina IntiaNo ratings yet
- Module 2 2023Document14 pagesModule 2 2023ubpi eswlNo ratings yet
- Joseph Minh Van Phase in Teaching Plan Spring 2021Document3 pagesJoseph Minh Van Phase in Teaching Plan Spring 2021api-540705173No ratings yet
- A Wolf by The Ears - Mattie LennonDocument19 pagesA Wolf by The Ears - Mattie LennonMirNo ratings yet
- Top Notch 1 Unit 9 AssessmentDocument6 pagesTop Notch 1 Unit 9 AssessmentMa Camila Ramírez50% (6)
- Timeline of American OccupationDocument3 pagesTimeline of American OccupationHannibal F. Carado100% (3)
- Land Laws (MOHD AQIB SF)Document18 pagesLand Laws (MOHD AQIB SF)Mohd AqibNo ratings yet
- Entrepreneurship: The Entrepreneur, The Individual That SteersDocument11 pagesEntrepreneurship: The Entrepreneur, The Individual That SteersJohn Paulo Sayo0% (1)
- Sales-Management Solved MCQsDocument69 pagesSales-Management Solved MCQskrishna100% (3)
- Macquarie Equity Lever Adviser PresentationDocument18 pagesMacquarie Equity Lever Adviser PresentationOmkar BibikarNo ratings yet
- Project Report On "Buying Behaviour: of Gold With Regards ToDocument77 pagesProject Report On "Buying Behaviour: of Gold With Regards ToAbhishek MittalNo ratings yet
- Adidas Case StudyDocument5 pagesAdidas Case StudyToSeeTobeSeenNo ratings yet
- NegotiationDocument29 pagesNegotiationNina LeeNo ratings yet
- 240 Marilag v. MartinezDocument21 pages240 Marilag v. Martinezdos2reqjNo ratings yet
- Alkyl Benzene Sulphonic AcidDocument17 pagesAlkyl Benzene Sulphonic AcidZiauddeen Noor100% (1)
- Admin Law ReviewerDocument5 pagesAdmin Law ReviewerNirvana Time Sulivan Estiva100% (1)
- NEERJA 7th April 2016 Pre Shoot Draft PDFDocument120 pagesNEERJA 7th April 2016 Pre Shoot Draft PDFMuhammad Amir ShafiqNo ratings yet
- Iso 14001 Sample ProceduresDocument19 pagesIso 14001 Sample ProceduresMichelle Baxter McCullochNo ratings yet
- NSBM Student Well-Being Association: Our LogoDocument4 pagesNSBM Student Well-Being Association: Our LogoMaithri Vidana KariyakaranageNo ratings yet
- RF05 UAMS and School ConcernsDocument8 pagesRF05 UAMS and School ConcernsAngel Ann Pascua LuibNo ratings yet
- Scott Kugle-Framed, BlamedDocument58 pagesScott Kugle-Framed, BlamedSridutta dasNo ratings yet
- B. Contract of Sale: D. Fraud in FactumDocument5 pagesB. Contract of Sale: D. Fraud in Factumnavie VNo ratings yet
- PRIMER - CFC Young Couples ProgramDocument3 pagesPRIMER - CFC Young Couples Programgeorgeskie8100% (2)