You might also like
- The A EsseyDocument16 pagesThe A EsseyFunky121212121415163No ratings yet
- British Parliamentary StyleDocument15 pagesBritish Parliamentary StyleFunky121212121415163No ratings yet
- British Parliamentary StyleDocument15 pagesBritish Parliamentary StyleFunky121212121415163No ratings yet
- British Parliamentary StyleDocument15 pagesBritish Parliamentary StyleFunky121212121415163No ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Drug Dose Frank Shann 2017pdfDocument173 pagesDrug Dose Frank Shann 2017pdfrezafahlevi31290No ratings yet
- CHAPTER 6 ANAPHY TransesDocument13 pagesCHAPTER 6 ANAPHY TransesHoly HaeinNo ratings yet
- Fluids and Electrolytes 1Document9 pagesFluids and Electrolytes 1Mariel AbatayoNo ratings yet
- Summary-Parathormo-Set WashoutDocument2 pagesSummary-Parathormo-Set Washouthemato servisNo ratings yet
- TáchDocument18 pagesTáchQuỳnh TrâmNo ratings yet
- BSC 251 t2 QuestionsDocument38 pagesBSC 251 t2 QuestionssarahreyNo ratings yet
- Secondary Hyperparathyroidism - Pathogenesis, Disease Progression, and Therapeutic OptionsDocument9 pagesSecondary Hyperparathyroidism - Pathogenesis, Disease Progression, and Therapeutic OptionsJuanita GonzálezNo ratings yet
- Metabolic: Bone Disease of PrematurityDocument11 pagesMetabolic: Bone Disease of PrematurityPii TaNo ratings yet
- Assessment and Management of Patients With DiabetesDocument25 pagesAssessment and Management of Patients With DiabetesaliNo ratings yet
- Endocrinology Part 2Document6 pagesEndocrinology Part 2Prabhjot MundiNo ratings yet
- Assignment For Calcitonin HormoneDocument6 pagesAssignment For Calcitonin HormoneSAKARIYE MAXAMEDNo ratings yet
- Endocrine System BulletsDocument28 pagesEndocrine System Bulletswinner gift flowersNo ratings yet
- Parathyroid Gland: Dr. Mustafa Abdalgadir Khandgawi Ibrahim 2016Document24 pagesParathyroid Gland: Dr. Mustafa Abdalgadir Khandgawi Ibrahim 2016Mustafa KhandgawiNo ratings yet
- Chapter 13 Endocrine System NotesDocument12 pagesChapter 13 Endocrine System NotesJane XuNo ratings yet
- Peripheral and Central Giant Cell Lesions: Etiology, Origin of Giant Cells, Diagnosis and TreatmentDocument7 pagesPeripheral and Central Giant Cell Lesions: Etiology, Origin of Giant Cells, Diagnosis and TreatmentYeni PuspitasariNo ratings yet
- WEEK 5 LAB EXERCISE - Skeletal SystemDocument19 pagesWEEK 5 LAB EXERCISE - Skeletal SystemChristian GallardoNo ratings yet
- PREETI and RahulDocument22 pagesPREETI and Rahulnitinkhandelwal2911No ratings yet
- Drugs & DialysisDocument34 pagesDrugs & DialysisZulfkar Latief QadrieNo ratings yet
- Parathyroid (Hyper & Hypo)Document1 pageParathyroid (Hyper & Hypo)Vishal100% (1)
- Endocrine NursingDocument8 pagesEndocrine NursingBunny Bonny100% (5)
- TAS Exam Oct 2019: StatisticDocument253 pagesTAS Exam Oct 2019: StatisticMahbub RahmanNo ratings yet
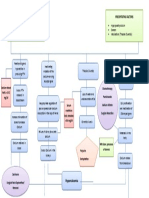
- Concept Map Hypercalcemia FinalDocument1 pageConcept Map Hypercalcemia FinalQueenie Rose Arsenal100% (1)
- Endocrine SystemDocument11 pagesEndocrine SystemDayledaniel SorvetoNo ratings yet
- Ms Test-Questio 2Document24 pagesMs Test-Questio 2Jackie AbarraNo ratings yet
- HYPOCALCEMIADocument27 pagesHYPOCALCEMIAJeffri SetiawanNo ratings yet
- Parathyroid, HyperparathyroidismDocument4 pagesParathyroid, Hyperparathyroidismjamil aoudeNo ratings yet
- Endocrine SystemDocument7 pagesEndocrine SystemMabes100% (1)
- Digital Sat Test 17Document28 pagesDigital Sat Test 17Kenan Nabil50% (2)
- The Peat WhispererDocument85 pagesThe Peat Whispererzarrin77100% (6)
- MA Bone CellsDocument10 pagesMA Bone CellskristinaNo ratings yet