You might also like
- Ishikawa IskemiaDocument2 pagesIshikawa IskemiaNiar MarhaliNo ratings yet
- Intestinal PathophysiologyDocument12 pagesIntestinal PathophysiologyNiar MarhaliNo ratings yet
- Ishikawa Iskemia-DikonversiDocument2 pagesIshikawa Iskemia-DikonversiNiar MarhaliNo ratings yet
- Rundown 26september - XLS'Document4 pagesRundown 26september - XLS'Niar MarhaliNo ratings yet
- Central Control of Body Weight and Appetite: J Clin Endocrinol Metab, November 2008, 93 (11) :S37-S50Document14 pagesCentral Control of Body Weight and Appetite: J Clin Endocrinol Metab, November 2008, 93 (11) :S37-S50Niar MarhaliNo ratings yet
- WJG 16 2978 PDFDocument13 pagesWJG 16 2978 PDFNiar MarhaliNo ratings yet
- Figure 1 Prevalence of Malnutrition Using The Pre-Set Definition and Five Screening ToolsDocument1 pageFigure 1 Prevalence of Malnutrition Using The Pre-Set Definition and Five Screening ToolsNiar MarhaliNo ratings yet
- Modeling AutismDocument15 pagesModeling AutismNiar MarhaliNo ratings yet
- GIE Colonscopy Prep and Diet GuideDocument4 pagesGIE Colonscopy Prep and Diet GuideNiar MarhaliNo ratings yet
- The DASH Diet PlanDocument50 pagesThe DASH Diet PlanNiar Marhali67% (3)
- Malnutrition in Acute Strok - ReviewDocument8 pagesMalnutrition in Acute Strok - ReviewNiar MarhaliNo ratings yet
- Hypokalemia MDRDocument7 pagesHypokalemia MDRNiar MarhaliNo ratings yet
- Weight Variation 2011 PDFDocument5 pagesWeight Variation 2011 PDFNiar MarhaliNo ratings yet
- Hypoalbumonemia in CKDDocument9 pagesHypoalbumonemia in CKDNiar MarhaliNo ratings yet
- Malnutrition in Acute Strok - ReviewDocument8 pagesMalnutrition in Acute Strok - ReviewNiar MarhaliNo ratings yet
- MikronutrienDocument13 pagesMikronutrienNiar MarhaliNo ratings yet
- Efek Konseling 2012 PDFDocument5 pagesEfek Konseling 2012 PDFNiar MarhaliNo ratings yet
- Skeletal Muscle Wasting Rev PDFDocument13 pagesSkeletal Muscle Wasting Rev PDFNiar MarhaliNo ratings yet
- Nutrition For Respiratory Disease PDFDocument46 pagesNutrition For Respiratory Disease PDFNiar MarhaliNo ratings yet
- D 800 Iu Indo 2009 PDFDocument5 pagesD 800 Iu Indo 2009 PDFNiar MarhaliNo ratings yet
- Dietary Antioxidant SupplementsDocument6 pagesDietary Antioxidant SupplementsNiar MarhaliNo ratings yet
- Nutr Suppl 2011 PDFDocument8 pagesNutr Suppl 2011 PDFNiar MarhaliNo ratings yet
- RecomendationDocument13 pagesRecomendationNiar MarhaliNo ratings yet
- Enteral Nutri On Copd PatientDocument7 pagesEnteral Nutri On Copd PatientRod Rafael De LeonNo ratings yet
- Antropoetri Pada LansiaDocument9 pagesAntropoetri Pada LansiaNiar MarhaliNo ratings yet
- Body Weight in TBDocument8 pagesBody Weight in TBNiar MarhaliNo ratings yet
- Update On Tuberculous Pleural EffusionDocument8 pagesUpdate On Tuberculous Pleural EffusionChristian TabarezNo ratings yet
- Natrium TuberculosisDocument2 pagesNatrium TuberculosisNiar MarhaliNo ratings yet
- Leptin and Energy MetabDocument7 pagesLeptin and Energy MetabNiar MarhaliNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- ZJZJP Roots Vauum PumpDocument8 pagesZJZJP Roots Vauum PumpAnonymous Tj3ApePIrNo ratings yet
- The Effects of Violent Video Games Research Paper English Comp2Document11 pagesThe Effects of Violent Video Games Research Paper English Comp2api-451442670No ratings yet
- J130KDocument6 pagesJ130KBelkisa ŠaćiriNo ratings yet
- G1 Series User Manual Ver. 1.2Document101 pagesG1 Series User Manual Ver. 1.2unedo parhusip100% (1)
- REV Description Appr'D CHK'D Prep'D: Tolerances (Unless Otherwise Stated) - (In)Document2 pagesREV Description Appr'D CHK'D Prep'D: Tolerances (Unless Otherwise Stated) - (In)Bacano CapoeiraNo ratings yet
- Tamilnadu Shop and Establishment ActDocument6 pagesTamilnadu Shop and Establishment ActShiny VargheesNo ratings yet
- 2005 Harley Davidson Sportster 883 66418Document136 pages2005 Harley Davidson Sportster 883 66418Josef Bruno SchlittenbauerNo ratings yet
- Pip-Elsmt01 P66 Midstream Projects 0 1/02/18: Document Number S & B Job Number Rev Date SheetDocument11 pagesPip-Elsmt01 P66 Midstream Projects 0 1/02/18: Document Number S & B Job Number Rev Date SheetAjay BaggaNo ratings yet
- Join Our Telegram Channel: @AJITLULLA: To Get Daily Question Papers & SolutionsDocument24 pagesJoin Our Telegram Channel: @AJITLULLA: To Get Daily Question Papers & SolutionsNaveen KumarNo ratings yet
- TC 10 emDocument7 pagesTC 10 emDina LydaNo ratings yet
- Thanks For Visiting Our Page!: Hi Doc!Document15 pagesThanks For Visiting Our Page!: Hi Doc!bey luNo ratings yet
- Intershield803 MDSDocument4 pagesIntershield803 MDSSahanNo ratings yet
- Multi-Wing Engineering GuideDocument7 pagesMulti-Wing Engineering Guidea_salehiNo ratings yet
- DPA Fact Sheet Women Prison and Drug War Jan2015 PDFDocument2 pagesDPA Fact Sheet Women Prison and Drug War Jan2015 PDFwebmaster@drugpolicy.orgNo ratings yet
- Carboset CA-600 - CST600 - CO - enDocument3 pagesCarboset CA-600 - CST600 - CO - enNilsNo ratings yet
- EXP 2 - Plug Flow Tubular ReactorDocument18 pagesEXP 2 - Plug Flow Tubular ReactorOng Jia YeeNo ratings yet
- Unit 8 Packet KeyDocument21 pagesUnit 8 Packet KeyHiddenNo ratings yet
- Ds0h Ufaa68 ProposalDocument11 pagesDs0h Ufaa68 Proposaledward baskaraNo ratings yet
- Care of Clients With Problems in OxygenationDocument5 pagesCare of Clients With Problems in OxygenationSkyla FiestaNo ratings yet
- Quality Factor of Inductor and CapacitorDocument4 pagesQuality Factor of Inductor and CapacitoradimeghaNo ratings yet
- DX340LC: Crawler ExcavatorDocument20 pagesDX340LC: Crawler ExcavatorFeristha Meriani TabitaNo ratings yet
- Unit-3.1.2-Sleeve and Cotter JointDocument18 pagesUnit-3.1.2-Sleeve and Cotter JointAsvath Guru100% (2)
- Republic Act No. 10389Document5 pagesRepublic Act No. 10389Marge RoseteNo ratings yet
- Itc LimitedDocument64 pagesItc Limitedjulee G0% (1)
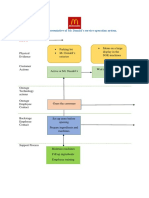
- Blueprint Huynh My Ky Duyen 2022 McDonald'sDocument2 pagesBlueprint Huynh My Ky Duyen 2022 McDonald'sHuỳnh Mỹ Kỳ DuyênNo ratings yet
- Jeremy A. Greene-Prescribing by Numbers - Drugs and The Definition of Disease-The Johns Hopkins University Press (2006) PDFDocument337 pagesJeremy A. Greene-Prescribing by Numbers - Drugs and The Definition of Disease-The Johns Hopkins University Press (2006) PDFBruno de CastroNo ratings yet
- Bisleri Water Industry: Project ReportDocument53 pagesBisleri Water Industry: Project ReportJohn CarterNo ratings yet
- 001 RuminatingpacketDocument12 pages001 Ruminatingpacketكسلان اكتب اسميNo ratings yet
- Dr. Sajjad Hussain Sumrra Isomerism (CHEM-305) Inorganic Chemistry-IIDocument48 pagesDr. Sajjad Hussain Sumrra Isomerism (CHEM-305) Inorganic Chemistry-IITanya DilshadNo ratings yet
- GEC - ReviewerDocument23 pagesGEC - ReviewerGlycel BagabagonNo ratings yet